
Abstract
Introduction:
Obstructive sleep apnea (OSA) is a condition whereby the airway gets partially or totally obstructed during sleep. Gold standard treatment for moderate to severe OSA is continuous positive airway pressure (CPAP). However, compliance with treatment is often poor, with low hours of usage and patients stopping treatment.
Methods:
A nonblinded, single-center, randomized controlled trial was conducted with patients randomized to 1 of 3 arms (arm 1, standard care; arm 2, modem; and arm 3, modem and DreamMapper™ app). Ninety patients diagnosed with OSA requiring CPAP were recruited. Data, including CPAP compliance, apnea/hypopnea index (AHI), and Epworth sleepiness score (ESS), were collected at baseline and 14 and 180 days post-CPAP initiation.
Results:
Of the group participants (N = 90), 68% were male and 32% female with a mean age of 52.0 ± 13.13 years, mean body–mass index of 36.4 ± 7.91 (kg/m2), mean ESS of 10.19 ± 5.75, and mean AHI of 43.5 ± 21.92 (events/hour). There was no statistically significant difference between the three arms in mean hours of CPAP usage in 24 hours at 14 days: arm 1, 6.22 ± 2.15; arm 2, 5.47 ± 2.25; and arm 3, 6.44 ± 1.54 (p = 0.256). There were also no statistically significant differences between the three arms in mean hours of CPAP usage in 24 hours at 180 days: arm 1, 6.20 ± 1.27; arm 2, 5.57 ± 1.49; and arm 3, 6.26 ± 1.29 (p = 0.479).
Discussion and Conclusion:
Compliance with CPAP treatment showed no significant differences between the three arms, with high compliance observed in all arms.
Introduction
Obstructive sleep apnea (OSA) is defined as temporary absence or cessation of breathing during sleep, which results in brief awakening from sleep to restore normal breathing. 1 OSA is a globally prevalent health disorder that affects up to 10% of the population 2 and is associated with increased risk of comorbidities such as hypertension, cardiovascular events, stroke, and myocardial infarction. 3 –5 OSA is also associated with symptoms of excessive daytime sleepiness (EDS), with EDS often associated with an increased risk of car accidents and accidents at work. 6
Continuous positive airway pressure (CPAP) is the gold standard and first-line treatment for moderate to severe OSA and indicated for patients with mild sleep apnea if conservative treatment has failed and there are significant daytime symptoms. 7 CPAP delivered through a mask acts a pneumatic splint, thus preventing the upper airway from collapsing during sleep. CPAP has been shown to improve self-reported daytime sleepiness, cognitive function, mood, and quality of life. 1,7
Despite the clinical evidence that CPAP has a positive effect on OSA symptoms, patient compliance with treatment can be problematic, with up to 30% of individuals stopping treatment within the 1st year. 8 There is an expectation that the CPAP machine should be worn while the patient is sleeping with optimal use agreed to be >4 hours per night for 70% of the time. 8 –10
In recent years, several technologies to improve patient compliance have been developed and introduced, including remote monitoring, educational packages, and remote clinical support. However, research evidence supporting increased patient compliance when using these interventions is conflicting, with the American Academy of Sleep Medicine calling for further research. 11 This call was supported by a recent meta-analysis that concluded the effectiveness of e-health intervention adherence remains to be determined. 12
Telemedicine may have the ability to improve CPAP compliance by improving access to specialist care. The aim of this study was to assess compliance with CPAP treatment and compare whether telemedicine interventions improve or offer similar compliance as standard care by randomizing participants to 1 of 3 arms, standard care (arm 1), virtual modem monitoring (arm 2), and virtual modem monitoring and a health application (DreamMapper™) accessed by the patient through a smart device to monitor their own CPAP use and data (arm 3).
Comparing two different telemedicine interventions against standard care offers the ability to explore further whether all telemedicine technologies are comparable or whether the type of intervention has an impact on patient compliance.
Methods
PARTICIPANTS
The study was a three-armed, nonblinded, randomized controlled study of consecutive patients with suspected OSA referred to the Respiratory and Sleep Department at the Isle of Wight NHS Trust, United Kingdom. Patients were referred from both General Practice and Secondary Care. Patients were diagnosed with sleep apnea following an overnight home cardiorespiratory sleep study (SOMNOtouch, Somnomedics, UK) with OSA confirmed by an apnea/hypopnea index (AHI) ≥513 and symptoms of EDS (Epworth sleepiness score [ESS] >10). 14
Inclusion criteria for participants were 18–80 years old and confirmed OSA (AHI ≥5). Exclusion criteria were pregnant women, patients outside the age range, any mental or physical disability that made it difficult for the patient to manage their own treatment, patients with complex sleep apnea (central sleep apnea and Cheyne–Stokes respiration), and patients who did not understand or have access to technology such as a smart device required to transmit data from their CPAP device through Bluetooth.
Health Research Authority ethics approval was granted on July 1, 2020 (Ref. No. 280212), and study recruitment and data collection took place between September 2020 and January 2022.
PROTOCOL
The study pathway is shown in Figure 1. Participants who met the inclusion criteria were sent information concerning the study before their appointment. Participants were consented and randomized to 1 of 3 arms using a random number generator (Excel, version 2108) by the lead clinician (Clinical Respiratory/Sleep Physiologist).
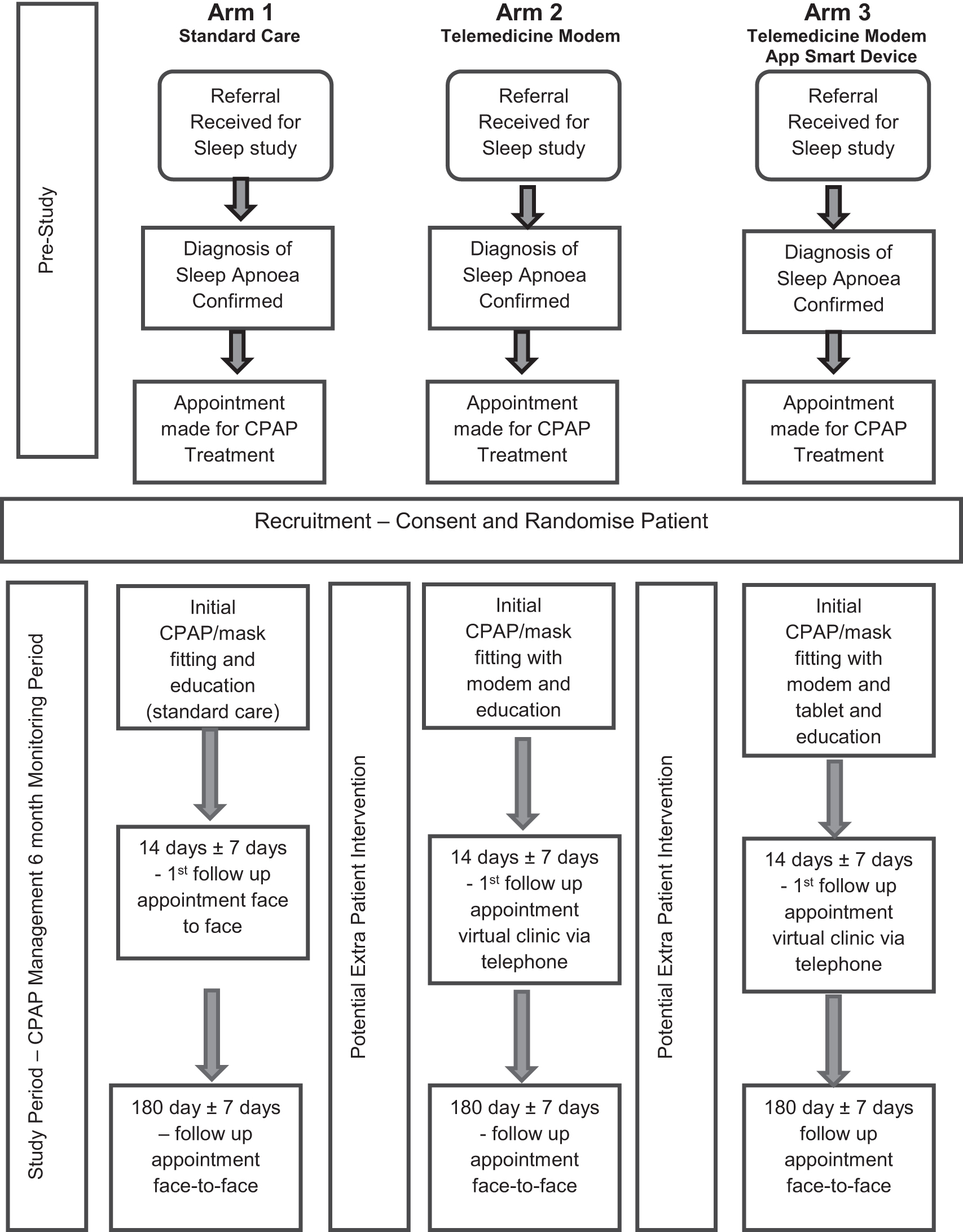
Study design. CPAP, continuous positive airway pressure.
At the patient's first appointment, demographics, including height, weight, body–mass index (BMI), collar size, and gender, were recorded. A full clinical history and daytime sleepiness score (ESS) examination was also completed. Patients were started on an automatic CPAP device at default pressure of 4–20 cmH2O (DreamStation 1, Philips). This included an individual standardized appointment of 1 hour, with information given about diagnosis and principles of OSA, CPAP use, and care and cleaning. Individual fitting of the nasal or oronasal mask was conducted.
Arm 1 participants were recruited to standard care, which consisted of an individual standardized appointment to fit their CPAP device and follow-up appointments that were face to face with the clinician. Participants in arm 1 did not have any access to their own CPAP data, other than at the review appointment with their clinician. The clinician was also limited to accessing patient CPAP data at the face–face appointment through the digital card data download.
Telemedicine was used in arms 2 and 3. Participants in arm 2 received a cellular modem that was installed as an accessory to the DreamStation CPAP device at their first appointment. The cellular module has a certified cellular radio module that requires a 3G connection to transmit and receive data. The cellular modem automatically makes a daily call as long as the CPAP device has power and the blower is turned off. The cellular modem transmits CPAP therapy data wirelessly at a bandwidth of 1,250 KHz to a cloud-based website (EncoreAnywhere, Philips), allowing the clinician to remotely monitor treatment through a browser.
The cellular modem is also able to receive data such as CPAP prescription changes from the clinician on its daily call. The modem did not provide any information or feedback to the patient in real time. Device data were provided by the clinician at the patient review appointment, which was conducted through telephone (virtual).
Patients recruited to intervention arm 3 received a cellular modem and mobile smart device application (DreamMapper, Philips), which enabled the CPAP device to transmit data to a smart device through Bluetooth; information could also be accessed using any browser. DreamMapper provided the patients with real-time feedback concerning their own therapy progress every night, including hours used, mask fit, and AHI score. DreamMapper also allowed patients to preset their own goals such as how many consecutive days of CPAP use they wished to achieve within the app and to track that progress. The app also provided educational videos and tips for using and maintaining equipment.
The number of standard appointments was the same in each arm (0 days, 14 ± 7 days, and 180 ± 7 days), with arms 2 and 3 receiving their follow-up appointments by telephone (virtually). Ad hoc appointments were triggered by both patient and clinician and occurred for several reasons, including poor compliance, dryness requiring humidification, mask reviews due to leak, and/or pressure sores requiring change of mask.
In all arms, patient's CPAP data were reviewed on the day of their appointment; however, in the event of the patient contacting the clinician due to problems with their treatment, the clinician was able to access the CPAP data in real time for participants in arms 2 and 3. This had the potential for the clinician to make quicker decisions around treatment changes in the patient groups with telemedicine.
FOLLOW-UP
The participants in each arm were reviewed by a clinician at 14 ± 7 days and 180 ± 7 days to check their compliance data, hours of CPAP usage within 24 hours, percentage of days CPAP was used, percentage of days CPAP was used for >4 hours, mask fit (leak percentage), AHI, and daytime sleepiness using ESS. Standard care (arm 1) participants were seen face to face with their data downloaded through a secure digital card from their device.
The telemedicine intervention group (arms 2 and 3) participants were reviewed through the telephone with CPAP data available through modem transmission.
SAMPLE SIZE CALCULATION
A power analysis was conducted to determine the required sample size. Data as reported by Munafo 15 –17 suggested that a 50% rate of compliance was expected in the CPAP control group (standard care) and that a suggested rise in compliance to 70% would be clinically important. 9,11
Based on a difference in compliance rate of 20% between the control and traditional face-to-face group (50%) and the telemedicine group (70%) conditions, with an effect size of d = 0.72, it was calculated that 30 patients in each arm (total of 90 participants) would be needed to achieve a power of 0.80 (i.e., 80% chance to detect a true difference) at the 5% significance level. 18 We continued to recruit until the sample size was achieved, allowing for dropout patients.
STATISTICAL ANALYSES
Results are reported as mean and standard deviation for continuous variables with normal distribution. Baseline demographics are reported for each arm, with group differences analyzed using one-way analysis of variance (ANOVA). CPAP compliance data, ESS, and AHI at 14 and 180 days within and between each arm were compared using ANOVA (one-way and two-way ANOVAs).
Effect size for compliance data was calculated between each arm (one-way ANOVA) with values of η 2 = 0.01 small, η 2 = 0.06 medium, and η 2 = 0.014 large effects. For all tests, a value of p < 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS statistics (version 27).
Results
PARTICIPANTS
A total of 116 patients diagnosed with OSA were approached between September 2020 and April 2021, of which 5 patients declined and 10 patients did not meet the recruitment criteria. The remaining 101 patients were consented to the study, although 10 patients subsequently dropped out (2 from arm 1, 4 from arm 2, and 4 from arm 3) and 1 patient was lost to follow-up (arm 1).
Reasons for dropout included poor compliance for a variety of reasons, including claustrophobia, nasal congestion, reduced quality sleep, not able to tolerate pressure, and depression with discontinuation of treatment occurring within the first 3–12 weeks of the patients commencing CPAP treatment. Participants without completed data at 180 ± 7 days were not included in the data analysis (n = 11), leaving 90 patients for full analysis. Full data collection was completed by January 2022.
All complete cases were included in the analysis. Boxplots of compliance (hours the CPAP device was used in 24 hours) demonstrated some outliers, with one patient demonstrating unusually excessive use of 12.09 hours (arm 1) and three patients with very poor compliance of 0.02 hours (arm 2) and 0.34 and 1.27 hours (arm 3). These data were included in the full analysis, the rationale being that clinical evidence shows that CPAP compliance is variable and therefore excluding these patients would possibly add bias into the analyses.
The total sample (N = 90) consisted of 61 males (68%) and 29 females (32%) with a mean age of 52 ± 13.13 years. The mean BMI of participants was 36.4 ± 7.91 (kg/m2), mean ESS was 10.19 ± 5.75, and mean AHI was 43.5 ± 21.92 (events/hour). Of the 90 participants, 2% had been previously diagnosed with mild OSA (AHI 5–14), 32% with moderate OSA (AHI 15–29), and 66% with severe OSA (AHI ≥30).
BASELINE DEMOGRAPHICS
Baseline demographics, including AHI and ESS, for each arm are shown in Table 1. A one-way between-subjects ANOVA was conducted to test for any significant differences in baseline measures between each arm of the study. This revealed no significant baseline differences for age, gender ratio, weight, height, BMI, or collar size. However, significant differences were found for AHI and ESS.
Baseline Demographics of Study Participants in the Total Group and Within Each Arm
Data are presented as mean ± SD. p-Values are calculated with one-way ANOVA.
p < 0.05 is considered significant.
p-Value calculated with Pearson chi-square.
AHI, apnea/hypopnea index; ANOVA, analysis of variance; BMI, body–mass index; ESS, Epworth sleepiness score (of 24); SD, standard deviation.
A one-way ANOVA conducted on AHI at baseline between each arm did show a statistically significant difference (p = 0.013) with the post hoc test showing a significant difference in arm 1 versus 2 (p = 0.03) and in arm 2 versus 3 (p = 0.025).
A one-way ANOVA conducted on Epworth scores did show a statistically significant difference within groups (p = 0.049); however, post hoc tests (two-way ANOVA) showed no significant difference between arms. A one-way between-subjects analysis of covariance was carried out on AHI and ESS with no statistically significant impact on compliance.
COMPLIANCE DATA
Follow-up at 14 days
Participants were followed for 14 days (±7 days) after commencing CPAP treatment. A one-way ANOVA was conducted on CPAP compliance variables, including hours of CPAP usage in 24 hours, percentage of days CPAP was used, and percentage of days CPAP was used for ≥4 hours. There were no statistically significant differences between all the three arms in any of the compliance variables (Table 2), including average hours of CPAP usage in 24 hours in each arm (p = 0.256). No significant difference was also evident in percentage of days CPAP was used (p = 0.695) and percentage of days CPAP was used for ≥4 hours (p = 0.172). In all three arms, CPAP compliance was high.
Compliance Data of Study Participants in the Total Group and Within Each Arm at First Follow-Up (14 ± 7 Days) and Second Follow-Up (180 ± 7 Days)
Data are presented as mean ± SD. Percentage change in AHI calculated for each arm using baseline AHI and post-CPAP treatment AHI at 1st follow-up and 2nd follow-up; p and η 2 values are calculated with one-way ANOVA.
CPAP, continuous positive airway pressure.
Participants in all three arms showed an improvement in mean baseline subjective sleepiness score (ESS) post-CPAP treatment ( Tables 1 and 2 ), with no statistically significant differences observed between arms at the 14-day follow-up (p = 0.755). All patients showed an improvement in AHI compared with baseline after commencing CPAP treatment ( Tables 1 and 2).
All arms showed a significant percentage decrease in AHI from baseline at the 14-day follow-up. No statistically significant differences were observed in each arm at the 14-day follow-up (p = 0.644), with an effective improvement in sleep apnea score (AHI). Mask leak was acceptable (<10% per night) in all arms, with no significant difference observed between arms (p = 0.733).
Follow-up at 180 days
Participants were followed up at a second data point 180 days (±7 days) after commencing CPAP treatment. A one-way ANOVA was conducted on the same CPAP compliance variables as at 14 days. There were no statistically significant differences between all three arms in any of the compliance variables (Table 2). The average hours of CPAP usage in 24 hours in each arm showed no statistically significant difference (p = 0.479). No significant difference was also evident in percentage of days CPAP was used (p = 0.878) and percentage of days CPAP was used for ≥4 hours (p = 0.527). In all three arms, CPAP compliance was high.
Patients in all three arms continue to show an improvement in ESS and AHI (from baseline) at 180 days of CPAP treatment, with no statistically significant difference between each arm and each data point.
Participants in arm 3 who received the smart device application, DreamMapper, self-reported their weekly (7 days) usage of the app at 14 and 180 days (Fig. 2). A majority (94%) of patients in arm 3 report accessing the app at least once during a 7-day period at the 14-day follow-up, with this dropping to 84% of participants continuing to access the app at least once during a 7-day period at the 180-day follow-up.
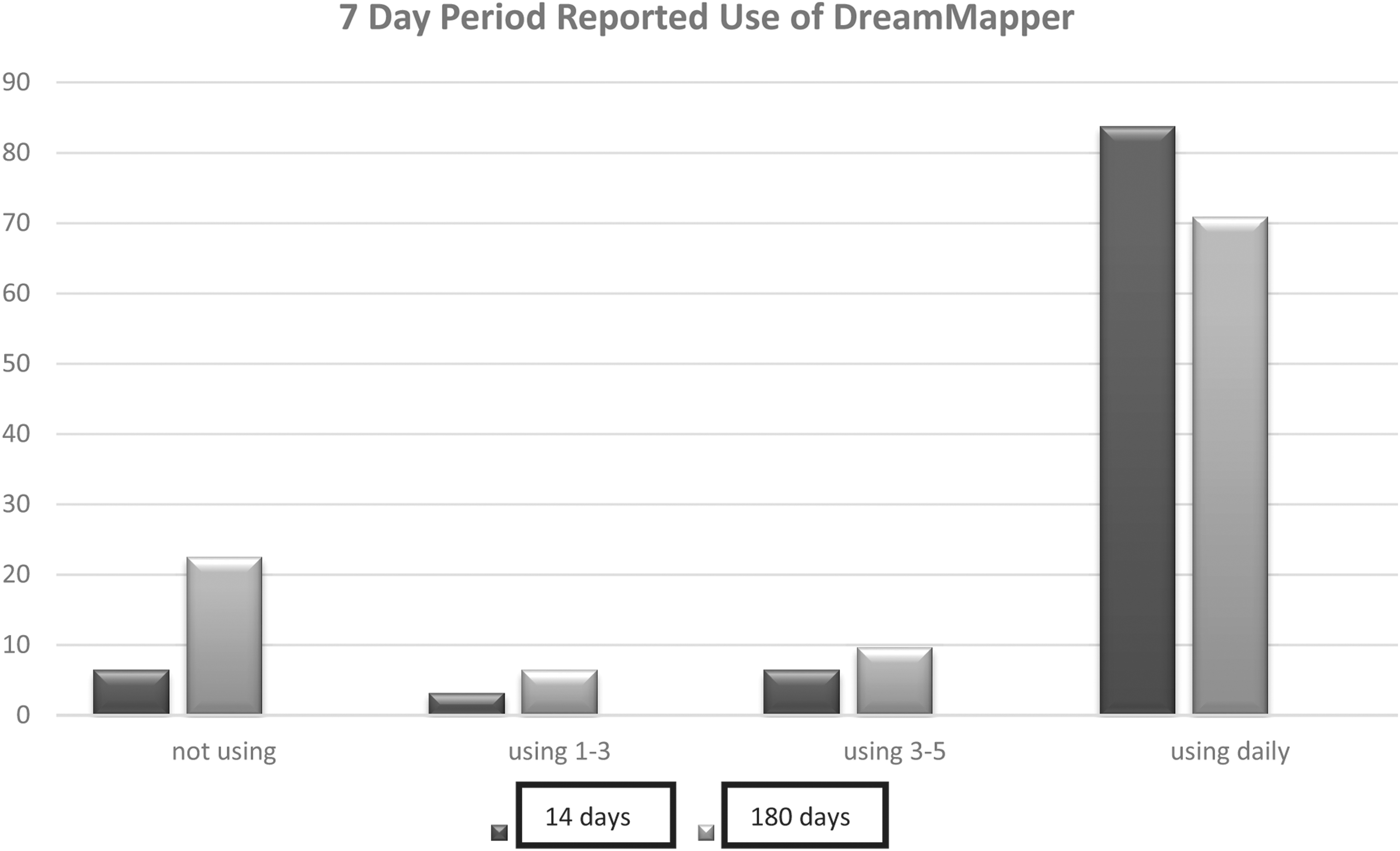
Percentage of participants (arm 3) issued a modem and smart device application (DreamMapper™) and self-reported use per 7-day period.
Discussion
The aim and uniqueness of the study were to compare standard care with two different methods of telemedicine and to explore the impact on CPAP compliance. Participants were randomized to remove bias (although not blinded), with telemedicine used in arms 2 and 3 to support remote monitoring and virtual appointments. Arm 3 participants were also supported by an app on a smart device (DreamMapper) that allowed participants access to motivational videos and daily feedback on their CPAP use and compliance and allowed the patient to preset goals using a smart device.
The participants were representative of the general population diagnosed with OSA (United Kingdom), with a spilt of two males to one female and mean age 52 years, and representative of study participants seen in previous studies when comparing age, gender ratio, and BMI. 19 –21
A high compliance rate was found (hours used in 24 hours) in all arms of the study at 14 and 180 days. The study did not show any statistically significant difference in compliance between standard care and telemedicine in arm 2 or 3 (Table 2) at 14 or 180 days of CPAP use.
These findings demonstrated that face-to-face appointments and virtual appointments supported by telemedicine in the form of a modem and/or DreamMapper app were as effective as standard care. This is supported by the improvement in self-reported daytime sleepiness symptoms (ESS). There was improvement in AHI and percentage change in AHI post-CPAP treatment in all arms (Table 2), with no statistically significant difference in all arms.
The use of telemedicine in CPAP is still an emerging technology, with previous studies reporting mixed results. Munafo et al., 15 Turino et al., 22 and Stepnowsky et al. 23 found no significant improvement in CPAP compliance in the telemedicine group when compared with standard care. However, Sparrow et al. 21 and Fox et al. 24 found a significant difference in patients who received telemedicine when compared with standard care, with Fox reporting a difference of 87 minutes (p < 0.0001) in the telemedicine group.
However, previous studies demonstrating a significant statistical improvement in the telemedicine group compared with standard care appear to have a somewhat low compliance rate in their standard care arm. 19,20 With compliance in the standard care arm often as low as 2–3 hours, 18,23,24 which is well below the compliance guidance of ≥4 hours for 70% of the time 7 and much lower than standard care, participants in arm 1 within our study had average CPAP usage per 24 hours of 6 hours 22 minutes.
The previous low compliance with standard care demonstrated in previous studies may explain the lack of statistical difference in standard care compared with telemedicine within our study as the standard care arm had a very high level of compliance (6 hours 22 minutes). This high level of compliance in the standard care arm was also demonstrated and supported in previous studies that had reported no significant difference in compliance. 15,22,23
Further exploration of the reasons for the low level of compliance with standard care demonstrated in some of the studies may explain the differences between standard care and telemedicine. It is possible that this could be due to other differences in care rather than the telemedicine intervention itself.
LIMITATIONS
There is a possibility that our study was underpowered and this is supported by the compliance data effect size (Table 2), which shows a small to medium effect. This is possibly due to the assumptions made previously concerning CPAP compliance rates observed in standard care. Power calculations for compliance were assumed to be 50% in standard care, 15 with an expected improvement of 70%; however, within the standard care arm of our study, compliance was at 79.2% (percentage of days CPAP was used >4 hours a night) at 14 days and 75.5% at 180 days, limiting the possibility of significant improvement due to achievement of maximum treatment.
Our study was a single-center study with a mainly white demographic within the United Kingdom and therefore may not represent the multiethnic diversity of the United Kingdom and the acceptance of technology. Very few studies are focused on patients in the United Kingdom and therefore the comparison of our study results of standard care and telemedicine may be skewed due to differences in health care systems (national health care and private health care), differences in access to technology, and social–economic differences.
Conclusions
The use of telemedicine in CPAP to improve patient compliance has shown no significant difference compared with standard care, but it has been found to be no less effective, with high compliance observed in all treatment arms. Telemedicine has the potential to support patients with their CPAP treatment and to offer a virtual pathway to individual patients.
Further exploration of differences observed in standard care across different studies and their reasons would bring greater understanding of why baseline compliance rates in multiple studies differ so greatly.
Future Research
A larger multicenter study would offer the potential to explore further the use of telemedicine in a boarder range of patient groups. It would also offer the opportunity to standardize standard care and therefore ensure that compliance change is due to the telemedicine intervention and not due to differences in standard care.
Future research examining different methods of telemedicine support available to CPAP patients and exploring further whether there is any significant difference between interventions offered and their impact on compliance should be conducted. Future research exploring and investigating the patient experience when using telemedicine and technology and accessing virtual appointments to manage their own CPAP treatment will improve patient engagement in creating patient-led pathways and a holistic approach.
Footnotes
Acknowledgment
The authors would also like to thank Dr Darren Van Laar for statistical assistance.
Disclosure Statement
This is not an industry-supported study. DreamMapper is a registered product of Philips Respironics. No financial support was provided, and the authors indicate no financial conflicts of interest.
Funding Information
This research was supported by the sleep team at St Mary's Hospital, Isle of Wight, and University of Portsmouth, School of Health and Care Professions.