
Abstract
Introduction:
The COVID-19 pandemic has challenged outpatient mental health clinics. This article compares care delivery and patient characteristics before and during the COVID-19 pandemic in outpatient mental health clinics within an academic health system.
Methods:
A retrospective cohort study was conducted in patients who received outpatient psychiatric services at two clinics (A and B). The investigators compared care delivery with patients with mental health conditions prepandemic (January 1–December 31, 2019) and midpandemic (January 1–December 31, 2020) periods. Care delivery was defined as the number and type of new and return visits (telehealth and face-to-face visits), patients with recorded measurement-based care (MBC) outcomes, and communication capability between patients and providers.
Results:
During the prepandemic period, 6,984 patients were seen in Clinics A and B, resulting in 57,629 visits. In the midpandemic period, 7,110 patients were served, resulting in 61,766 total visits. Medication management visits increased from 2019 to 2020; number of visits with documented outcome measures increased by 90% in Clinic A and 15% in Clinic B. The number of MyChart messages per patient increased more than twofold during the midpandemic period. The number of new visits with primary diagnosis of anxiety disorders increased in CY2020 and the number of visits with primary diagnosis of major depressive/mood disorders decreased in CY2020. Payor mix did not vary between the two periods although there was variability between payor mix at the two primary clinic locations.
Discussion:
The study suggests that there was no detrimental impact on access to care between the prepandemic and midpandemic periods within the health system. Mental health visits while pivoting to telehealth increased during the midpandemic period. Transition to telepsychiatry improved the ability to administer and document MBC.
Introduction
Since the onset of the COVID-19 pandemic, health care systems around the world have been forced to adapt delivering services with the evolving spread of the novel coronavirus (SARS-CoV-2). Medical care options have broadly moved to telehealth or hybrid availability, which facilitates patient engagement and mitigates the risk of disease spread. 1 Telehealth is particularly useful for services that do not require in-person examinations of patients. For psychiatry, in particular, telehealth has reduced barriers to care for many patients and decreased no-show rates. 2,3
Outpatient psychiatric care delivery quickly evolved to keep pace with the increased demand for services and decreased risk of infection transmission. Large hospital systems across the United States converted in-person appointments to telehealth visits, and record number of appointments were conducted virtually. 3 The demand for mental health services has grown with increased levels of psychological distress, loneliness, self-harm behavior, and decreased levels of subjective well-being associated with the pandemic. 4
Overall, patients and mental health professionals have adapted favorably to an increased reliance on telepsychiatry services. One study found that 73% of mental health providers using video modalities rated their experience as excellent. 5 Similarly, patients with mental health disorders have reported an increase in effectiveness, safety, appropriateness, access, and timeliness as reasons why they would continue to use videoconferencing to access services long term. 6
Measurement-based care (MBC) is the practice of guiding clinical treatment with evidence-based clinical practice guidelines in conjunction with patient-reported rating scales that provide an objective assessment of patient progress throughout treatment. Research has demonstrated that implementation of MBC in psychiatry has been shown to improve clinical outcomes, inform collaborative care efforts, enhance treatment decision-making processes, and increase patient engagement in treatment. 7 The Generalized Anxiety Disorder-7 (GAD-7) and Patient Health Questionnaire-9 (PHQ-9) are brief, well-validated, and self-report measures that efficiently screen for anxiety and depression symptoms in clinical and research settings. 8 –11
The PHQ-9 is a dual-purpose instrument that can establish depressive disorder diagnoses and measure depressive symptom severity. The availability of MBC standard measures in both hard copy and electronic formats allows clinicians in psychiatric and medical contexts to easily incorporate MBC into their practices and improve outcomes for their patients. 12 This is particularly applicable in the context of the COVID-19 pandemic causing the transition to wide telehealth use.
In addition to changing service delivery demands, the rates of psychiatric illnesses increased both as a result of COVID-19 infections and COVID-19-related lifestyle changes after March 2020. Preliminary research indicates that COVID-19 survivors are at an increased risk of psychiatric sequelae, including mood and anxiety disorders. 13 This association continued to be observed in subsequent waves of the pandemic. 14 In addition, some researchers found an increase in suicide attempts among those in counties hit hardest by the pandemic. 15
This article compares care delivery before and during the COVID-19 pandemic in outpatient mental health clinics within an academic health system offering subspecialty services to a large county in Southern California. This article will outline the changes put in place and detail their impact on patients seeking psychiatry and psychotherapy services.
Methods
SETTING
The study was conducted at two ambulatory clinics (Clinics A and B) in one of the region's largest providers of behavioral and mental health services, housed within an academic health system. Clinic A is a multidisciplinary clinic that offers outpatient psychiatric services including medication management, individual psychotherapy, group psychotherapy, interventional psychiatry (e.g., injections and transcranial magnetic stimulation treatment [TMS]), and case management. The largest program within Clinic A is the general psychiatry clinic that offers general psychiatric care for common mental health conditions.
There are also subspecialty programs including Senior Behavioral Health, Women's Reproductive Mental Health, College Mental Health Program, Interventional Psychiatry, Child and Teen Clinic, and the Substance Treatment and Recovery Program. This ambulatory clinic has >30,000 visits per year and ∼60 providers.
Clinic B is primarily a general psychiatry clinic. It also houses the cognitive assessment and risk evaluation program for early psychosis assessment, treatment, and research. Clinic B has >15,000 visits per year with ∼30 providers.
At the start of the pandemic in 2020, outpatient services quickly pivoted to telehealth appointments to offer ongoing psychiatric care to patients. Telehealth was already established at Clinic B in a limited capacity to be able to offer psychiatric care to patients in remote locations. Telehealth video visits were primarily offered through My Chart Video Visits (MCVV) through the electronic medical record system. When patients could not connect to MCVV due to technical problems, Health Insurance Portability and Accountablity Act-compliant Zoom or Doximity was offered as alternatives.
Telephone visits were offered to those without video capability. On March 18, 2020, Clinic A offered MCVV to patients due to the pandemic mandated shutdown. Clinical support staff first prioritized converting appointments to MCVV for patients aged 70 years and higher (i.e., at high risk for COVID-19) and for follow-up visits. As of March 30, 2020, all appointments were offered through MCVV including new visits.
Owing to ongoing concerns about COVID-19, not only for patients but also for providers, the option to work remotely was allowed and encouraged for all providers between April 15, 2020, and May 26, 2020. Remote work was again encouraged during subsequent surges from December 21, 2020, to March 1, 2021, and from January 3, 2022, to February 14, 2022. During periods when COVID-19 was not surging, both in-person and telehealth options were widely available.
At Clinic B, all providers except resident trainees had access to video services by March 16, 2020. By March 18, 2020, 51.6% of all sessions were MCVVs at Clinic B. By March 20, 2020, all residents were able to provide video visits and by March 28, 2020, all providers had the option of working from home. Remote work was encouraged during subsequent surges during the same time frames as Clinic A.
The biggest challenges were technology problems at clinics (e.g., insufficient internet bandwidth across buildings and audio problems), or with patients having difficulties with access to internet or devices.
STUDY DESIGN AND MEASURES
A retrospective cohort study was conducted in patients who received outpatient psychiatric services at a west coast academic health system. The investigators compared the care delivery with patients with mental health conditions prepandemic (January 1–December 31, 2019) and midpandemic (January 1–December 31, 2020) periods. Care delivery was defined as the number of new and return visits (telehealth and face-to-face visits), the number of different types of visits, the number of patients with recorded MBC outcomes, and ease of communication between patients and providers. Patient characteristics (age, race, primary diagnosis, and payor mix) were also compared between the two time periods. All data were retrieved by an analyst using the electronic medical record Epic Systems Corporation database.
The types of psychiatric services included in this study were medication management, individual therapy, and combined medication management and therapy. The services were retrieved using current procedural terminology codes. For the purposes of this investigation, combined medication management and therapy visits were counted as medication management visits, and intensive outpatient programs and transcranial magnetic stimulation (TMS) visits were excluded from the study. Unique patients and total number of visits were captured for medication management and therapy visits as well as telehealth and face-to-face (in-person) visits during the two time periods. The visits are coded as telehealth (video or telephone) or face-to-face visits.
The quality-of-care delivery was measured by the number of patients with documented PHQ-9 and GAD-7 scores, primary diagnoses for new patients (further recoded by investigators into groups of diagnoses), and communication capability between patients and providers (using the number of MyChart accounts established as well as the number of messages received).
Patient demographics were also compared between the pre- and midpandemic periods including age, gender, race/ethnicity (as self-selected at time of patient registration), and insurance type (commercial, private, Medicaid, Medicare, other government, and self-pay). The project was determined not to be Human Subjects Research by the Human Research Protections Program.
STATISTICAL ANALYSIS
For all new and return visits, the types of services were compared between the two time periods. Statistical analysis could only be conducted on new (or unique) visits and was evaluated using chi-square analysis (p < 0.05 considered significant).
Results
In the prepandemic period (CY2019), 6,984 patients were seen in Clinics A and B, resulting in 57,629 total visits (Table 1). In the midpandemic period, a total of 7,110 unique patients were served that resulted in 61,766 total visits. This was an increase of 126 unique patients and 4,137 total visits from prepandemic to midpandemic periods. Most patients were White and ranged in age groups of 18–29 and 30–39 years.
Demographics
There was a total of 3,832 new visits in 2019, which decreased to 3,523 in 2020. Among these, the proportion of medication management visits slightly increased from 2019 to 2020 (chi [df = 1/N = 7,355] = 4.53, p = 0.033; Table 2). The breakdown of new visits as a function of visit type (medication management vs. therapy) and modality (in-person vs. telehealth) is shown in Figure 1. The timeline of telehealth and face-to-face visits for both clinics are depicted in Figure 2 for both prepandemic and midpandemic periods. As expected, the number of face-to-face visits declined dramatically at the start of the COVID-19 pandemic, whereas telehealth visits increased for both medication and therapy types of visits.
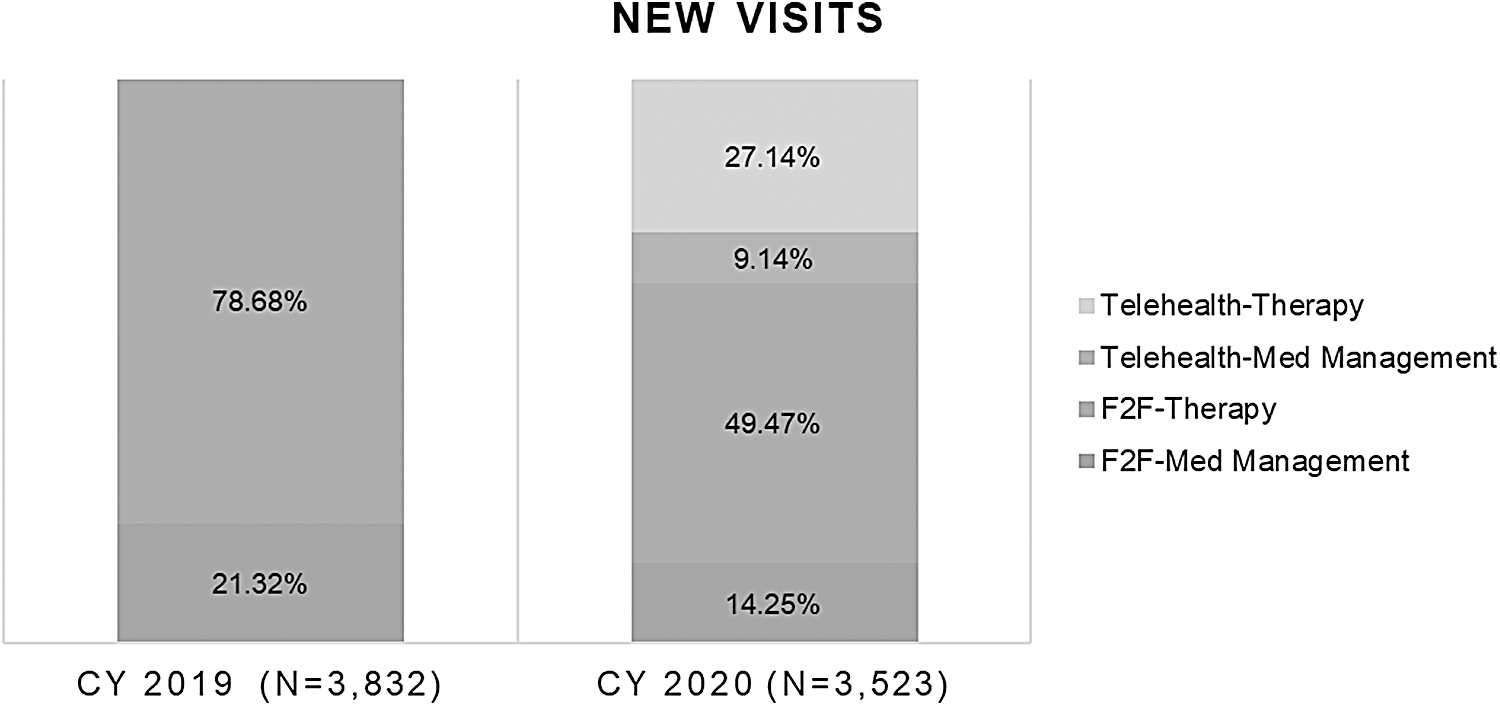
Telehealth and F2F visits during 2019 and 2020. F2F, face-to-face.
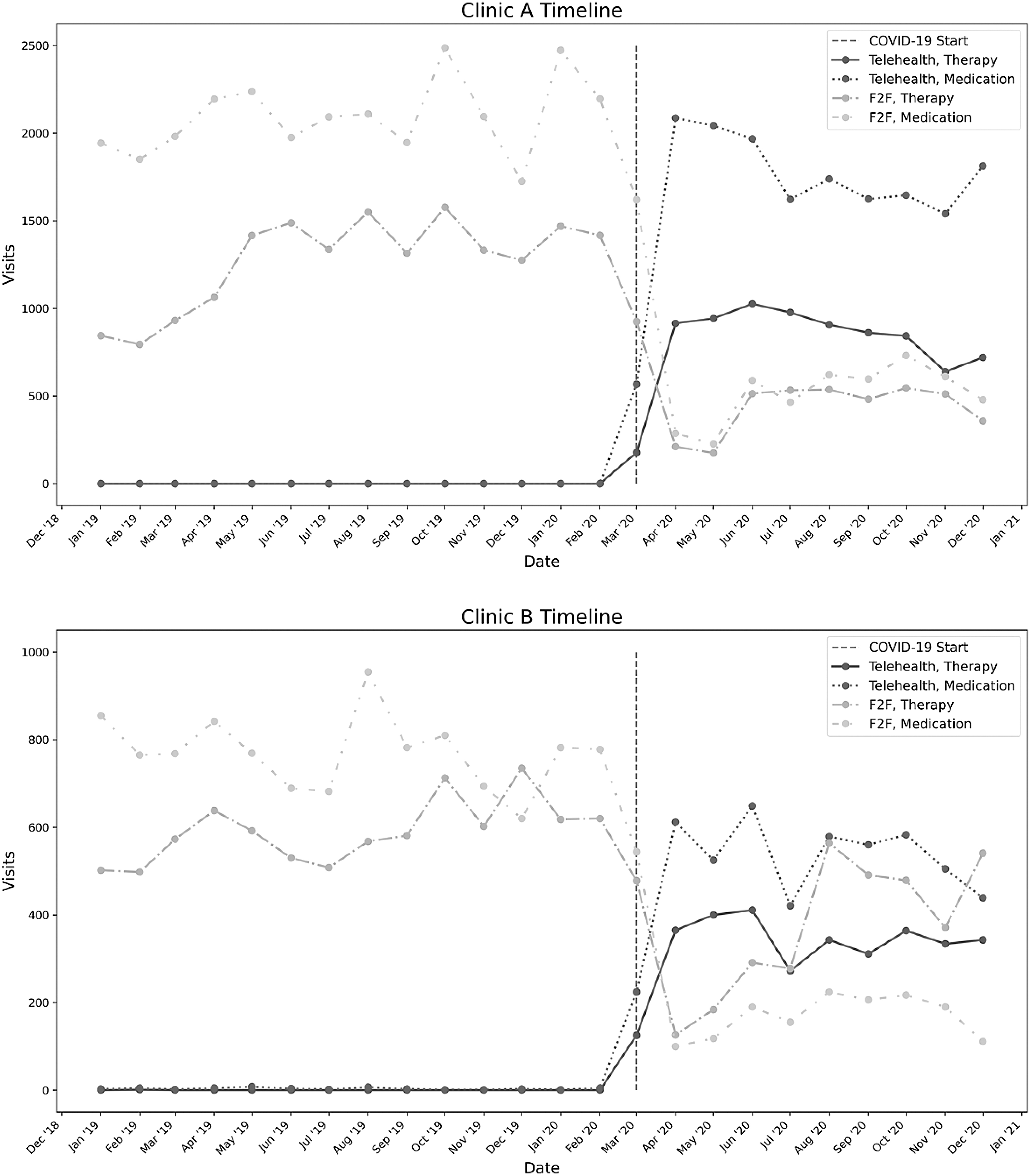
Timeline of telehealth and F2F visits for Clinics A and B.
Number and Type of New Visits Provided During 2019 and 2020
Chi-square (df = 1) = 4.53, p = 0.033.
The number of visits with either a PHQ-9 or GAD-7 during each calendar year was captured by clinic location for both CY2019 and CY2020 (Fig. 3). In Clinic A, there was an increase of 1,486 visits with a documented outcome measure (reflecting 90% increase) compared with only an increase of 295 visits (reflecting 15% increase) for Clinic B from 2019 to 2020. In 2019, 3,654 out of 57,629 visits (6%) had measurement-based outcomes, whereas in 2020, 5,435 out of 61,766 visits (9%) had measurement-based outcomes.
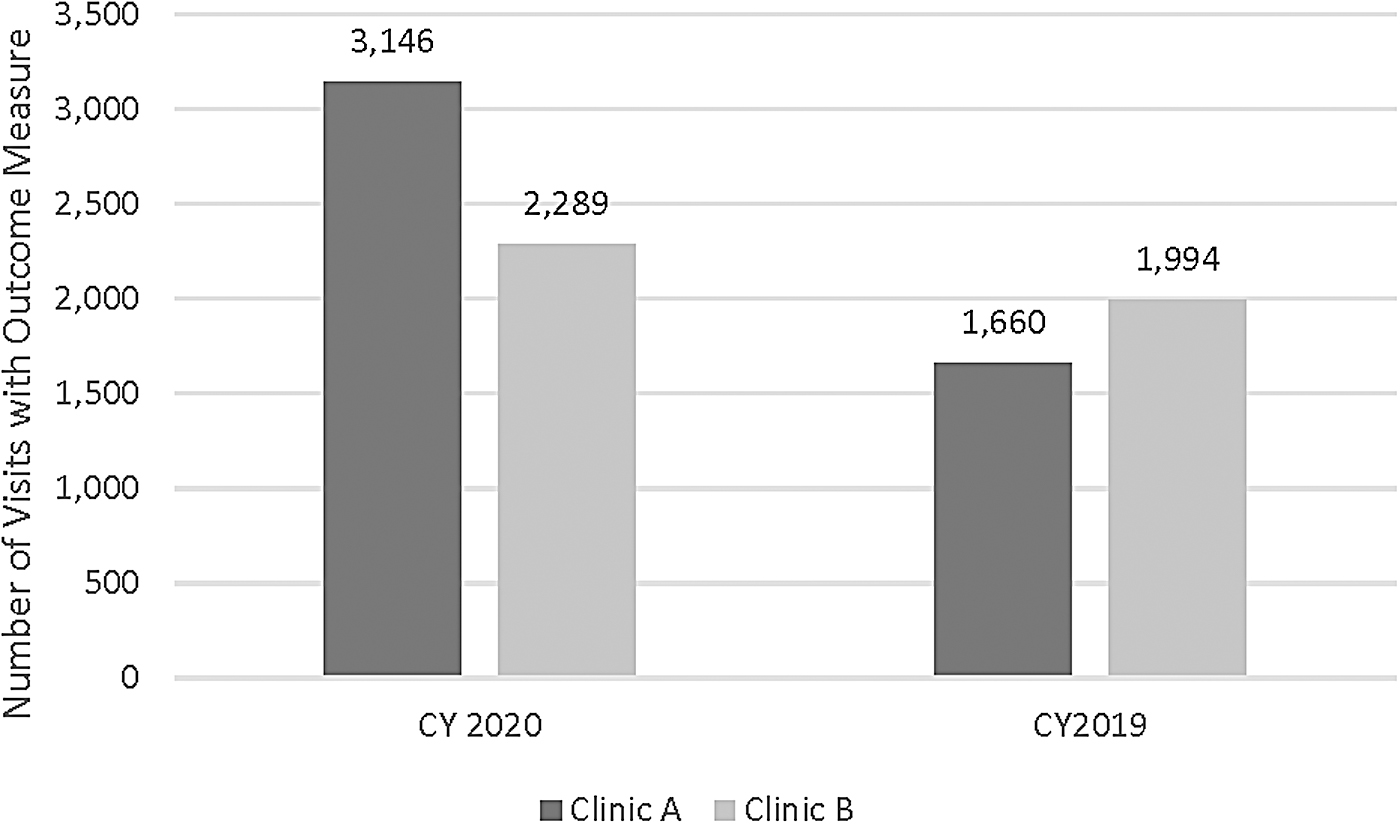
Number of total visits with measurement-based care outcomes.
During the prepandemic period, the number of MyChart accounts for an individual patient that was activated was 5,841; the number of total messages received for these patients was 190,208, reflecting ∼33 messages per patient. In the midpandemic period, the number of MyChart accounts that were activated was 6,603, which resulted in 453,962 messages, reflecting ∼69 messages per patient (i.e., more than twice as many messages per year and per patient relative to the prepandemic period). The number of patients who declined MyChart access was 211 in the prepandemic period compared with 67 in the midpandemic period.
Primary diagnoses were compared for new visits between CY2019 and CY2020. The number of new visits was similar between the 2 calendar years (3,553 for CY2020, 3,879 for CY2019). The top 10 disorders are presented in Figure 4. The three most common disorders were major depressive/mood disorders, anxiety disorders, and post-traumatic stress disorder and related disorders. The number of new visits with primary diagnoses of anxiety disorders increased in CY2020 and the number of visits with primary diagnoses of major depressive/mood disorders decreased in CY2020.
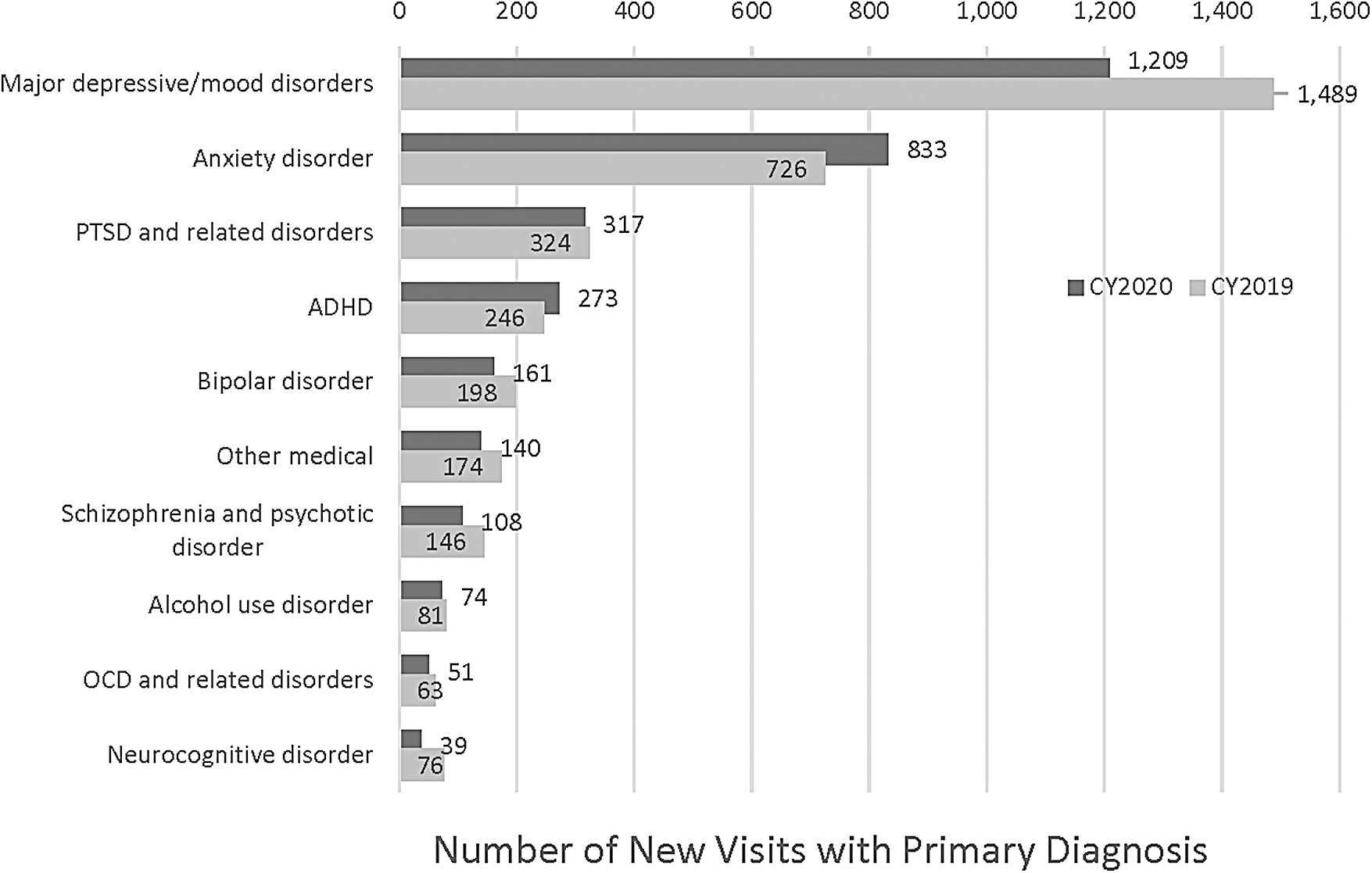
Top primary diagnoses for new visits. ADHD, attention-deficit hyperactivity disorder; OCD, obsessive-compulsive disorder; PTSD, post-traumatic stress disorder.
Payor mix did not vary between the 2 calendar years although there was variability between payor mix at the two primary clinic locations within the health system (Fig. 5). Commercial payors were the predominant payor for visits in both CY2019 and CY2020, as well as for both clinic locations. However, at Clinic B, there was more diversity of payors beyond commercial, including Medicaid, other government, Medicare, and self-pay.
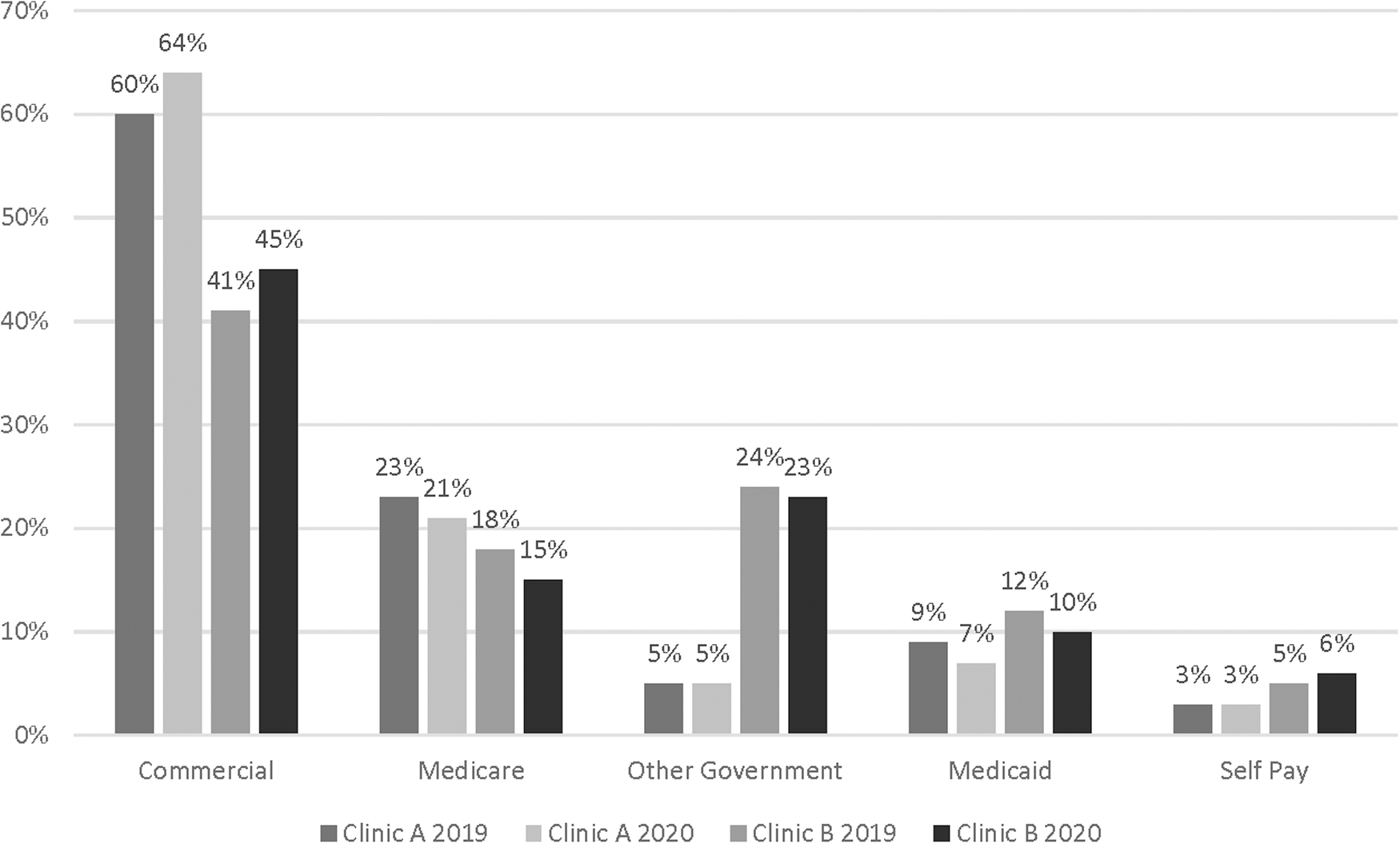
Payor mix for Clinics A and B during 2019 and 2020.
LIMITATIONS
There were a few limitations to this study. The data source was an electronic health record that was designed to capture health services, not research data. Individual level data were not available; therefore, associations or causality could not be established. The study was conducted at only one health system and, therefore, demographics of the population studied may not be representative of other geographic regions. Generalizability to other health systems or regions may be limited.
Discussion
The COVID-19 pandemic has undoubtedly impacted the mental health of those in the United States and worldwide. 16 –18 Access to mental health services is critical especially to those who may be the most vulnerable. There is evidence from this investigation that there was no detrimental impact on access to care between the prepandemic and midpandemic periods within our health system. Patient characteristics who were served during the two time periods did not change based upon payor mix. Mental health visits appropriately pivoted to telehealth and, in fact, the number of unique patients and visits increased during the midpandemic period.
This is not surprising given the measured impact of the pandemic on mental health, substance use, and suicidal ideation. 15,17 Although face-to-face visits are preferred for most medical practices, there can be challenges within telehealth psychiatric practices, including lack of patient engagement during therapy visits, difficulty evaluating nonverbal symptoms of disorders, and difficulty objectively evaluating medication side effects (tardive dyskinesia, vital signs, and weight). 3 It is important to recognize that reimbursement for telehealth services allowed us to provide these services in a time of crisis and continued advocacy for telehealth is needed.
Patients continue to use telehealth services to reduce risk of contracting COVID-19, and to more easily access care with fewer barriers (e.g., transportation, mobility, and time). Moreover, it is important to continue advocacy for populations with inequitable access to mental health care more broadly.
The opportunity to utilize MBC was enhanced using telehealth visits and there was a significant increase in the number of patients with documented PHQ-9 and GAD-7 scores. In CY2020, the number of visits with an outcome measure documented was almost double the number of visits recorded in CY2019 at Clinic A. Even accounting for the increased volume of patient visits, there was an increase in the number of visits with an outcome measure. The electronic check-in process for telehealth visits eased the ability to capture PHQ-9 and GAD-7 measurements, compared with manual entry during in-person visits.
MBC allows providers to use data to evaluate and customize treatment planning for their patients and has been demonstrated to improve treatment outcomes. 19,20 It should be noted that our transition to telepsychiatry improved our ability to perform and document MBC (PHQ-9, GAD-7).
Access to providers was also measured indirectly by activation of MyChart accounts and messages received by the providers. The number of accounts that were activated midpandemic did increase, but not proportional to the number of telehealth visits. This suggests that not everyone was able to activate their accounts, did not have access to mobile devices, or simply did not want to activate their accounts. However, the large increase in message volume midpandemic suggests that patient–provider engagement and communication were improved with the conversion to telehealth modalities.
The increased volume may also reflect the increase in number of patients with anxiety disorders requiring frequent assurance from providers during the pandemic. This tool helps patients to advocate for their care and helps clinicians to provide patients with resources and recommendations in a timely manner. Future research should focus on the impact of these increased communication and workload on provider and staff burnout, lack of revenue for these nonbillable activities, and decreased morale.
The top primary diagnoses that were encountered pre- and midpandemic also did not differ appreciably, with the exception of anxiety disorders, which increased during the pandemic and major depressive/mood disorders that decreased during the pandemic. 17 Future investigations may be focused on whether increase in visits by certain populations (e.g., children and young adults) contributed to this pattern in diagnoses.
Although the rapid adjustment to telehealth during the pandemic was beneficial in many ways, including allowing ongoing access to mental health care, there are also common barriers. Some patients may have difficulty accessing and using the technology needed for virtual visits. They may not have access to the necessary devices or stable Wi-Fi, or they may not have the technology literacy to navigate virtual appointments. 21 These technological barriers are particularly applicable for older adults, especially those lacking caregiver support to help with the technology. 22
Older adults may also have hearing and vision impairments that can limit the ability to engage in telehealth visits. 23 Low socioeconomic status is also associated with financial barriers to access the technology and less freedom of leveraging the technology when and where one wants. 24 Another barrier noted in the literature is the desire for more personalized care and interactions with the provider. 25
Prepandemic, private insurance and Centers for Medicare & Medicaid Services reimbursement rules have disincentivized clinics to use telehealth visits. These barriers need to be overcome to continue providing quality care moving forward. There are still limitations with providers having to provide visits in which they are licensed and the location of the patient. Increasing use of remote work may present challenges going forward.
Future research should focus on impact on socioeconomically disadvantaged patients who may be unable to access providers if telehealth modalities were not offered.
Conclusion
The COVID-19 pandemic had a significant impact worldwide. Despite the disruption to our personal and professional lives, this study demonstrated that the outpatient psychiatric care provided to patients during the pandemic did not have detrimental impacts. In fact, some areas, such as the ability to measure clinical outcomes, improved as well as communication between patients and providers through electronic platforms. Telehealth modalities should continue to be available to improve access and ultimately clinical outcomes for patients with mental health needs.
Footnotes
Acknowledgments
The authors thank Susan Varites, Paven Lidstone, and Jeremy Bass for their help.
Authors' Contributions
Conceptualization of the study was carried out by K.C.L., K.L.D., E.L., A.L.C., S.G.B., and K.H. Data curation was done by K.C.L. and A.L.C. Formal analysis was carried out by K.C.L., K.L.D., and K.H. Funding acquisition is not applicable. Investigation was taken care by K.C.L. and K.H. Methodology was taken care by K.C.L., K.L.D., E.L., A.L.C., S.G.B., and K.H. Project administration was by K.C.L. and A.L.C. Resources were taken care by K.C.L. and A.L.C. Supervision was done by K.C.L. and A.L.C. Visualization was done by K.C.L., K.L.D., E.L., A.L.C., S.G.B., and K.H. Writing (original) of the article was by K.C.L., K.L.D., E.L., A.L.C., S.G.B., and K.H. Writing (review/editing) of the article was by K.C.L., K.L.D., E.L., A.L.C., S.G.B., and K.H.
Disclosure Statement
Authors have no conflicts to disclose.
Funding Information
This research was supported by the Veterans Health Administration (IK2CX001584 awarded to Dr. Harlé).