
Abstract
Introduction:
The 2019 Coronavirus Disease (COVID-19) pandemic necessitated a mass transition in genetics clinics nationwide from in-person care to virtual care through telehealth. Before the COVID-19 pandemic, there was limited research on the use of telehealth in genetics specialties. Therefore, the COVID-19 pandemic presented a unique opportunity to study this emerging mode of care delivery in the setting of genetics clinics. This study described the scope of telehealth use in genetics clinics nationally and determined how COVID-19 influenced patients' decisions regarding their genetic care.
Methods:
Two anonymous surveys for patients and providers were developed. The patient survey was offered online to all genetics patients seen through telehealth at a Manhattan-based practice between March and December 2020. The provider survey was distributed through several listservs to genetics providers nationwide.
Results:
Patients (n = 242) and providers (n = 150) responded. Telehealth was used in all specialty genetics clinics for both initial and follow-up visits. Telehealth was both effective and satisfactory to patients for both visit types and across specialties; however, Asian and Hispanic/Latino patients had significantly lower mean satisfaction scores compared with White patients (p = 0.03 and 0.04, respectively). Patients appreciated telehealth for its convenience and to avoid COVID-19 exposure. Providers across specialties and provider types preferred telehealth for follow-up rather than initial visits. Several clinic initiatives related to telehealth were identified.
Discussion:
Telehealth was generally well received by both patients and providers, and is expected to become permanent option in genetics clinics. Further studies are needed to identify barriers to accessing telehealth.
Introduction
Before the 2019 Coronavirus Disease (COVID-19) outbreak, telehealth was an emerging tool in genetics. Access to medical genetics services due to geographical distance, cost, and long wait times due to a paucity of providers is a known issue. 1,2 Due to COVID-19, the slow shift to telehealth rapidly accelerated in the United States. Prior research has been limited to comparative analyses of differences in cost and patient outcomes for hereditary breast and ovarian cancer (HBOC). 2 –12
Telehealth was found to be generally noninferior to in-person HBOC counseling in knowledge gained, improved psychosocial outcomes, and genetic counseling satisfaction; however, these results are from small, homogenous populations (White women) and fail to investigate patient motivations behind their choice of service delivery method. 5 –9 While prior research was largely conducted for pretest counseling, there is also evidence suggesting that telehealth is an acceptable method to disclose HBOC testing results. 8,10,12
Further investigation is needed to discern how telehealth is implemented and perceived in noncancer specialties, and to assess how telehealth programs have evolved at different institutions in the wake of COVID-19. 13,14
Notably, there has been little research into the motivations behind patient choice between in-person and telehealth options. During the pandemic, a more diverse patient population than ever had access to telehealth due to Medicare's coverage of these visits and the lifting of restrictions on practicing across state lines. 15,16 Patients and providers were faced with the challenge of engaging in complex, fraught sessions through videoconferencing or phone calls in specialties that had not previously used telehealth.
Several studies have described the shift to telehealth in genetics during the COVID-19 pandemic: one reproductive genetics clinic noted a drastic increase in access to their services, but barriers included insurance coverage, and subsequent unwillingness to shoulder the telehealth implementation costs without guaranteed reimbursement. 17,18 Challenges reported by genetic counselors included difficulty identifying nonverbal cues of patients' emotional response, insurance billing, technology issues, and coordination of sample collection and paperwork. 18 –21
Previous research has explored several facets of telehealth in genetics clinics with an emphasis on patient perceptions, especially in HBOC. However, understanding patient outcomes and perceptions in noncancer settings, genetics provider perceptions (especially nongenetic counselors), and the patients' decision-making processes when selecting a service delivery mode is lacking. With temporary changes in insurance coverage and mandatory shelter-in-place orders, the patient population that was using telehealth was more diverse in race and ethnicity, socioeconomic status, insurance status, and technological savvy. Therefore, the COVID-19 pandemic presented a unique opportunity to gather diverse opinions on this emerging mode of health care delivery.
Methods
PATIENT SURVEY
Questions were adapted from validated questionnaires for the following domains: Telehealth Satisfaction, Telehealth Ease of Use, Future Preference Regarding Telehealth Use, and the Impact of the Coronavirus on their Genetics Clinic experience. 14,22 –25 Total Satisfaction Scores (TSS), Total Effectiveness Scores (TES), and Perceived Coronavirus Threat Scores (PCTS) were calculated. The patient survey was available in English and Spanish.
PROVIDER SURVEY
After a detailed literature review, provider questions were developed by the investigators to measure provider satisfaction with telehealth and preference for telehealth versus in-person appointments. In addition, subspecialty differences were assessed. The provider survey was offered in English only.
Both surveys were hosted by REDCap.
PATIENT RECRUITMENT
Participants were recruited from patients who completed a telehealth appointment in the Division of Medical Genetics and Genomics at Icahn School of Medicine at Mount Sinai (ISMMS) from March to December 2020. Patients/parents were given the option to participate through a message sent through the electronic medical record patient portal (Epic MyChart). This message was automated to be sent after the genetics provider closed the telehealth encounter.
PROVIDER RECRUITMENT
All providers offering services in genetics clinics were targeted, including medical geneticists, genetic counselors, dieticians, nurses, and nurse practitioners. Provider participants had to have direct patient contact in a medical genetics setting and worked during the pandemic to participate. Genetics providers nationwide were invited to participate through the National Society of Genetic Counselors (NSGC) member listserv, the New York State Genetics Task Force, Medical Geneticists Facebook groups, and the Mount Sinai Medical Genetics Training program alumni network.
This study was approved by the COVID-19 Protocol Review Committee at the ISMMS, and this research was determined to be exempt by the Institutional Review Board at the ISMMS. Informed consent was obtained from all participants. “Telehealth” was limited to the use of videoconferencing to remotely deliver medical genetics care, including genetic counseling.
STATISTICAL ANALYSES
Descriptive statistics were calculated for both patient and provider responses. Patient responses were analyzed as three scores; higher PCTS indicates greater fear of contracting the coronavirus, higher TSS and TES indicate greater visit satisfaction and more effective communication, respectively. Comparisons between groups were performed using Chi-square, Fisher's exact, T-tests, analysis of variance (ANOVA), Pearson's correlation, or linear regression as appropriate. All analyses were done using SAS® Enterprise Ver 3.8 (SAS Institute, Inc., Cary, NC), and considered exploratory using a significance level of 0.05.
Free-text responses were analyzed using thematic analysis in which codes were generated by two reviewers, and initial conflicting results were resolved through discussion until concordance was reached.
Results
PATIENT DEMOGRAPHICS
A total of 274 patients responded, 242 were included in the analyses. The patient respondents' demographics are shown in Table 1. The majority (67%) completed the survey after an initial visit with their genetics provider, while 79 (33%) had a follow-up visit. Most were seen for cancer genetic counseling (110, 45%) and reproductive counseling (87, 36%). Patients were more commonly seen for initial visits across all subspecialties except for Metabolic/Lysosomal Storage Diseases Clinics.
Patient Characteristics (n = 242)
SD, standard deviation.
SATISFACTION, EFFECTIVENESS, AND PCTS
Mean TSS was high (39.9 ± 4.95), as was mean TES (21.4 ± 2.8), indicating that overall patients were highly satisfied with and received effective genetics care through telehealth (Table 2). TSS, TES, and PCTS were compared across patient demographics, specialty, and visit type (initial vs. follow-up). Mean TSS was significantly lower among Asian (mean 36.4) and Hispanic/Latino (mean 39.3) respondents compared with White respondents (mean 40.3) (p = 0.03 and 0.04, via T-test, respectively), although the TSS was generally high regardless of self-reported race and ethnicity.
Descriptive Statistics of Perceived Coronavirus Threat Score, Total Satisfaction Score, and Total Effectiveness Score
Max possible score 28.
Max possible score 45.
Max possible score 25.
PCTS, Perceived Coronavirus Threat Score; TES, Total Effectiveness Score; TSS, Total Satisfaction Score.
Mean TES was significantly lower for Asian (mean 19.2), Hispanic/Latino (mean 20.2), and Black (mean 20.0) patients compared with White patients (mean 21.9) (p = 0.009, 0.006, and 0.03, via T-tests, respectively); however, overall TES was also high across all groups.
TES was also impacted by visit type: patients seen for an initial visit had significantly lower mean TES compared with patients seen for follow-up visits (initial mean = 20.7, follow-up mean = 22.1, p = 0.003 via T-test). There was no significant difference in TSS between visit types. There were no significant differences in mean TES or TSS among different specialties. The correlation between scores showed high correlation between TES and TSS (0.7), and low correlation between TES and PCTS (−0.02), and TSS and PCTS (0.1) (Pearson's correlation coefficient).
PATIENT PERSPECTIVES ON CURRENT AND FUTURE TELEHEALTH USE
Patient views on telehealth use and future choice of service delivery method were explored. Regarding future choice between telehealth and in person, 81% of patients reported being likely to choose telehealth, while only 4% reported they were unlikely to choose telehealth. Future choice was not significantly associated with PCTS, age, visit type, or specialty.
When asked to select all reasons they might choose telehealth over in person in the future (when COVID-19 is no longer a threat), 61% of patients indicated that telehealth saves them time, the technology was easy to use, and that telehealth was equivalent to being in person. Of those who said telehealth was equivalent to in-person visits (49%), 40 (33%) were seen for follow-up visits and 78 (66%) were seen for initial visits (Fig. 1A).
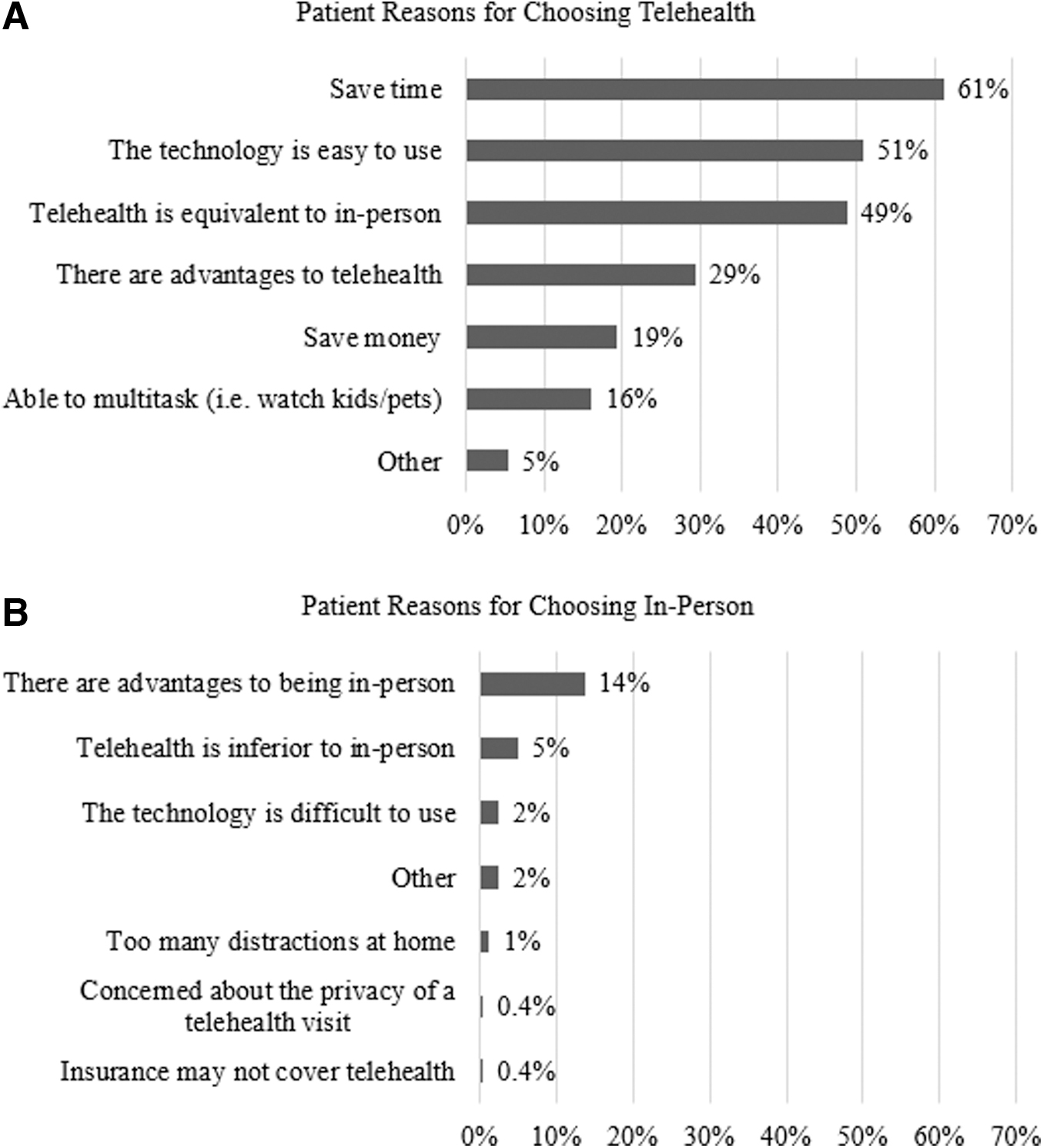
Reasons for patient future preference for
When asked about preferences for future telehealth use in genetics clinics major themes included convenience (15/33), saves time (12/33), and saves money (4/33). One patient remarked that telehealth “allows access to specialists that otherwise wouldn't be practical.” Another patient wrote, “For a more serious genetic issue, I may prefer to have the option for in person. For something more likely benign, telehealth works.”
When asked to select all reasons they might choose in person over telehealth in the future, 33 (14%) noted there are advantages to an in-person visit (23 initial and 10 follow-up visits) (Fig. 1B). The most common theme for perceived advantages to being in person was that it better facilitates relationship building with the provider (9/26).
Regarding feelings about having access to their genetics providers during the pandemic, major themes included concern for COVID-19 safety; 28/116 expressed that they may not have booked an appointment if they had to come in person. Several respondents reported that having access improved their mental health during the pandemic. Patients reported overwhelmingly positive feelings about having access to their genetics provider through telehealth during the pandemic.
PROVIDER DEMOGRAPHICS
One hundred fifty providers completed the survey, and their characteristics are summarized in Table 3. The majority were genetic counselors (91, 61%), followed by nutritionists (31, 21%) and physician geneticists (22, 15%). The most common specialties were metabolic/lysosomal storage disorders (26%), multiple specialties (23%), and cancer (20%). Nutritionists, physician assistants, and nurse practitioners were combined into an “Other” category. Most physician geneticists reported working in multiple clinics. Reproductive, cardiovascular, and cancer were overwhelmingly represented by genetic counselors.
Provider Characteristics (n = 150)
PROVIDER PERSPECTIVES ON CURRENT AND FUTURE TELEHEALTH USE
Providers' prepandemic telehealth use revealed that 50 respondents (34%) were using it to some degree before, although most were using it infrequently (less than five telehealth sessions in the 6 months before the pandemic). There was no significant association between prior telehealth use and provider type or specialty. Prepandemic telehealth use was more common in follow-up visits compared with initial visits. This was true across all specialties except for reproductive. Almost all providers (147, 98%) reported using telehealth during the pandemic. As expected, a drastic increase was observed for both visit types and across all specialties.
Providers were asked to report all issues that they experienced in conducting telehealth appointments; the most reported were patient user error (103, 69%), patient access to the necessary technology (97, 65%), and nonuser-related technical issues (52, 35%). The majority of providers (79%) expect patients to continue to choose telehealth for visits (79% for initial, 97% for follow-up) after the pandemic. There were no significant differences in responses by provider type or specialty.
Providers were also asked about their own future preference between telehealth and in person; ∼45% of providers had no preferred service delivery mode for either visit type. However, there was a significant difference in preference between initial (14% preferred telehealth) and follow-up (39% preferred telehealth) visit types (p ≤ 0.0001 via Chi-square), indicating a preference to conduct initial visits in person and follow-up visits using telehealth. There were no significant associations between provider future preference and specialty, provider type, years in practice, or provider age for either visit type.
Providers were asked to describe any new institutional initiatives regarding telehealth use that had been created or accelerated by the pandemic. Major themes included making telehealth permanent (18/54), adding virtual or remote resources to improve the telehealth experience (e.g., e-sign software, electronic patient questionnaires, integrating facial analysis software with videoconferencing or photograph submissions, etc.) (8/54), changing the telehealth billing process (4/54), and pushing for genetic counselor licensure laws (5/54).
Discussion
This study explored patient and provider experiences and perceptions of telehealth use in genetics clinics during a global pandemic. Analysis of patient TES and TSS indicates that telehealth use at this single, large institution was both effective and satisfactory across all specialties, and for both initial and follow-up visit types. These results are consistent with previous research both before and during COVID-19, 18,20,21,26 but this study was able to expand these findings to a more diverse patient sample and a greater variety of genetics specialties. Satisfaction and effectiveness were not correlated with coronavirus fear, indicating that these scores may also be high outside of a pandemic.
The finding that mean TES was slightly but significantly lower for initial visits compared with follow-up visits may indicate that patients are better served by having their initial visit in person or through a hybrid model where some portions of the visit are done through telehealth and others in person, while follow-up visits were largely satisfactory through telehealth.
A possible explanation for this difference could be differences in patient–provider rapport between the visit types; patients lack established rapport in initial visits, whereas they can rely on an established relationship in follow-up visits. This is supported by the fact that providers have reported greater difficulty in building rapport over telehealth compared with in person. 27 Analysis of provider responses showed that providers across all specialties preferred to continue using telehealth for follow-up visits more so than initial visits, indicating that telehealth will likely remain in use in all specialties post-COVID-19.
Patient self-reported race and ethnicity was significantly associated with lower TSS and TES, which may be related to a lack of diversity among providers at this institution. Previous research has demonstrated that patient satisfaction and health outcomes improve when there is patient–physician racial concordance. 28 Furthermore, White genetic counselors have reported feeling less effective with minority patients compared with White patients in both telehealth and in-person sessions. 6
This study also found that patients are motivated in their choice between in person and telehealth by convenience, the desire to form a connection with their provider, and COVID-19 safety concerns. This information provides initial insight into patient choice between service delivery modes that can help guide genetics clinics in determining under which circumstances to offer each; for example, complex initial visits may be better in person, or through a hybrid model where counseling occurs through telehealth with in-person follow-up for certain procedures (e.g., physical examination, genetic testing), while simple follow-up visits may be better through telehealth with mobile phlebotomy appointments or local laboratory collections if needed. Patients expressed their interest in telehealth outside of a pandemic setting, consistent with other studies. 26
The major issues reported by providers were patient user error and access to technology, similar to reports from other studies. 20,21 However, there may be biases in these responses, as providers may not realize or report their own user error. Furthermore, these issues did not translate into lower patient satisfaction with telehealth. This finding is limited to the patient population seen in the Mount Sinai Health System.
The issue of patient access to technology highlights the population that was unreachable by the survey distribution methods used in this study; patients who do not have access to the devices or connectivity required to participate in a telehealth visit. These patients may be left behind as the health care industry begins to rely more heavily upon telehealth. One way to increase telehealth accessibility to these patients could be in the form of a spoke-and-hub model of care, wherein a patient travels to a local clinic to be connected to a telehealth visit with their remote genetics provider. 5 However, this solution does not address the pandemic scenario in which travel to any clinic is a safety risk.
One study in a reproductive clinic found that non-English-speaking patients were more likely to be seen in person in the COVID-19 pandemic, indicating that translation needs are not currently being met by telehealth. 29 As well, increased use of phone visits may improve reach to rural areas with limited internet connectivity. Further research is needed to identify and address these barriers to telehealth to reduce disparities in access.
Finally, this study provides strong evidence that the large-scale use of telehealth triggered by the COVID-19 pandemic will likely continue in the postpandemic era. Important considerations for future use are long-term solutions to the temporary telehealth policy changes that were put in place during the pandemic. For example, Medicare temporarily changed its policy to include coverage of telehealth visits. 15 Similarly, state licensure bodies temporarily allowed providers to see patients through telehealth across state lines, and many states have required insurance companies to waive copays for telehealth visits. 16 There is much work to be done to develop lasting changes to insurance coverage, billing, and state licensure policies to better incorporate long-term telehealth use. 18
Initiatives on the institutional level that can improve long-term telehealth use include the development of electronic patient questionnaires and educational materials, and the incorporation of e-sign software and mobile or local laboratory visits into the clinical workflow to improve remote offerings. Additional initiatives reported by providers include the integration of facial dysmorphology analysis software into video visits and improved integration of interpreters or live translation software in telehealth visits.
This study has several limitations. First, there may have been a self-selection bias in the patient population; patients who appreciated telehealth may have been more willing to complete a survey. Patients who had difficulty with telehealth technology may have also had difficulty completing the survey. In addition, our patient population was limited to those who completed telehealth visits through the MyChart portal.
Second, while this study improves upon previous research in terms of sample size and diversity, these findings are limited due to poor representation in some participant categories, such as some of the genetic specialties and provider types. We were not able to collect data on primary language, and therefore, cannot determine whether this impacted satisfaction with telehealth.
The patient survey was only offered in English and Spanish; although these are the most common languages spoken by our patient population, it is likely patients who spoke other primary languages were not able to participate. Some subgroup analyses are limited by sample size. Generalizability of the patient survey findings is limited by the fact that all patient respondents were seen at a single site. As well, a general visit satisfaction scale was not used, which could have been compared with in-person visits. In addition, this study does not address perspectives and experiences of patients who were unable to access telehealth services during the pandemic.
Finally, due to the anonymous nature of the patient survey we were unable to link patient responses to additional information such as insurance carrier, primary language, or other socioeconomic factors. Regarding the provider survey race/ethnicity was not collected, and therefore we cannot comment on the diversity of that sample.
Overall, this study found that telehealth was satisfactory and effective to a diverse group of patients, and accepted by genetics providers across specialties, with several significant findings that may guide future use. Additional work needs to be done to increase diversity among providers to meet the needs of diverse patients. Follow-up visits may be more appropriate to conduct through telehealth than initial visits in some genetics specialties.
Footnotes
Acknowledgments
We thank the patients who participated in this study. This work was completed in partial fulfillment of the requirements of a Master's degree in Genetic Counseling at the Icahn School of Medicine at Mount Sinai by Julia Martinez in May 2021.
Authors' Contributions
J.M.M. designed conceptualization, methodology, investigation, formal analysis, writing-original draft, and visualization; R.E.Z. and G.A.D. contributed to methodology, writing-reviewing and editing; H.N. assisted with conceptualization, methodology, investigation, writing-reviewing and editing, supervision, and resources.
Disclosure Statement
No competing financial interests exist.
Funding Information
Funding was provided by the Master's program in Genetic Counseling at the Icahn School of Medicine at Mount Sinai.