
Abstract
Purpose:
Extension for Community Health Outcomes (ECHO) is a model of continuing medical education meant to connect academic medical center-based specialists with community providers to increase capacity in managing complex health conditions. The purpose of this study was to evaluate the effectiveness of a shortened “bootcamp” ECHO model in increasing participant competence with topics related to transgender and gender diverse (TGD) health care and the impact of “bootcamp” participation on enrollment in an ongoing ECHO series.
Methods:
An ongoing monthly ECHO series was instituted on topics of TGD health. After 2 years, the team implemented a four-session “bootcamp” for four consecutive weeks during March 2022 to introduce foundational topics for new participants who had joined or were considering joining the ongoing series. Qualitative and quantitative results were collected from self-reported pre-/post-surveys as well as from in-session quizzes.
Results:
There were 71 participants in the “bootcamp” including health care providers and support staff. Attendees reported a 10.3% increase (p = 0.02) in self-reported comfort providing care to transgender patients. Pre-/post-knowledge improved in areas of health inequities (50% vs. 74% correct pre/post), surgical requirements (33% vs. 74%), and effects of masculinizing (55% vs. 70%) and feminizing (64% vs. 89%) hormone therapy. Prescribing providers reported a significant change across four areas of practice competency. Among 71 “bootcamp” participants, 15 registered for the ongoing program.
Conclusion:
Use of a “bootcamp” highlights ways to increase participant comfort and knowledge in providing TGD health care in a shortened timeframe and recruit new participants to an ongoing ECHO curriculum.
Introduction
Approximately 1.6 million people in the United States, 0.5% of adults and 1.4% of youth aged 13–17 years, identify as transgender and gender diverse (TGD). 1 Of the adults who identify as transgender, 25.6% identified as gender nonconforming, whereas 38.5% identified as transgender women and 35.9% as transgender men (Table 1). 1 As more TGD patients are seeking medical care, it is crucial that medical providers have the knowledge and cultural responsiveness to care for patients in both primary care and specialty settings. A survey of TGD patients in Colorado showed that those who perceived their providers as transgender-inclusive were more likely to receive wellness examinations and less likely to delay care due to fear of discrimination. 2 Furthermore, those with inclusive providers reported lower rates of depression, suicidal thoughts or attempts, and fewer days of poor mental health in the past month. 2
Terminology
Although access to gender-affirming hormone therapy has been associated with decreased suicidal ideation, many TGD adults continue to report lack of access to and negative interactions with the health care system. 2 –4 Both primary care and specialty providers, in turn, report a lack of training, gaps in knowledge and/or discomfort in providing care to TGD patients. 5 –8 These studies call for more TGD-specific education in health professional schools' curricula and more descriptions of interventions to improve knowledge, comfort, and other aspects of TGD care.
In the setting of an increasing number of recent proposed and active bans on gender-affirming care in the United States, especially for TGD youth, providers of such care also fear these actions will lead to worsening mental health and increased suicidality among TGD patients. 9 There have also been calls for gender-affirming health care policies to be informed by clinicians. Increasing provider education and comfort with gender-affirming care can better equip clinicians to advocate for their TGD patients. 9,10
Extension for Community Health Outcomes (ECHO) is a collaborative model of continuing medical education, community practice support, and telementoring whose purpose is to connect academic medical center-based specialists with community providers to increase capacity in managing complex health conditions. Originally created by the University of New Mexico to support providers in the care management of patients with hepatitis C, the model has been used to address a wide range of training topics with evidence for the effectiveness of the model demonstrated for a range of conditions. 11 ECHO uses a combination of didactics with de-identified case-based presentations to allow for collegial interactions between the organizers and the participants.
To bridge the gap between patient needs and provider education in the field of TGD medicine, our team launched the ongoing series: “Transgender Health: Comprehensive Approaches in Primary Care” in February 2020. Other ECHO programs exist in the United States to provide care around topics related to gender diverse patients, but most are cohort based, with a set curriculum that is repeated over time to new participants. 12 Our ECHO Colorado effort was intentionally designed as an ongoing monthly series to facilitate longitudinal learning. The hub team continually generates new topics for the curriculum from review of evaluations, new literature findings, and/or specific questions from participants.
With this unique model, however, we found that as new participants joined, some expressed concerns that they missed foundational topics covered during earlier sessions. We, therefore, developed the four-session “bootcamp” series, “Transgender Health: Core Concepts for Primary Care,” to enhance knowledge for new participants who were considering joining the longitudinal curriculum and conducted these sessions in March 2022. The primary aims of this study were to (1) evaluate the effectiveness of the “bootcamp” model in increasing participant comfort and knowledge with topics related to TGD health care and (2) measure the impact of “bootcamp” participation on enrollment in the longitudinal ECHO series.
Methods
CURRICULUM
The March 2022 sessions included (1) the role of mental health care in gender diverse patients, (2) medical management of feminizing hormones, (3) medical management of masculinizing hormones, and (4) introduction to gender-affirming surgery. These topics were considered foundational by the hub team. Each hour-long session included a 20-min didactic followed by interactive discussion and case-based presentations. Sessions were led by primary care physicians, endocrinologists, psychiatrists, and plastic surgeons. Presentations included data from the World Professional Association in Transgender Health (WPATH) Standards of Care as well as guidelines from the Endocrine Society and other medical literature as appropriate to the topic. 13,14
PARTICIPANT RECRUITMENT
ECHO Colorado promoted the “bootcamp” series through both the ECHO Colorado website and outreach to a dedicated listserv comprising >12,000 individuals interested in the ECHO Colorado program. Participants enrolled through the ECHO Colorado Learning Management System Connect. Recruitment for the series was aimed at “prescribing primary care providers in North America” and was open to individuals who work with TGD populations in all aspects as well as those in a variety of health-related setting who expressed interests in better understanding gender-affirming hormone therapies. In addition, 1 h of Continuing Medical Education credit was offered for completing each of the four sessions.
DATA COLLECTION
Evaluation of the March 2022 “bootcamp” series utilized a pre-/post-survey design. Baseline and follow-up data were collected before and after the series. The evaluation also assessed knowledge before and after each session. This evaluation was reviewed by the Colorado Multiple Institutional Review Board and designated as “Not Human Subject Research” (#21-5040).
Series baseline data
Baseline data were collected when participants registered for the series on a web-based portal ECHO Connect. This included a 26-item registration questionnaire for an inclusive registration process and unified data collection. Registrants self-reported information regarding demographics (i.e., gender, race, and ethnicity), professional background (i.e., credentials and profession), and practice characteristics (e.g., populations served, care setting, and location of practice). A custom question was added for this series to capture participants' self-reported comfort with providing primary care to both cisgender and transgender patients (response options were a 4-point scale: very uncomfortable, uncomfortable, comfortable, and very comfortable). One hundred one (n = 101) individuals registered for the series and of those 71 participated by attending at least one of four sessions.
Series follow-up data
Follow-up data were collected after the series ended. Participants, which included individuals who had attended at least one of the four sessions, were e-mailed a survey through Qualtrics survey software, 15 with three reminder e-mails. The survey captured self-reported comfort in providing care to cisgender and transgender patients, and four retrospective pre-/post-questions in which participants rated their perceived competence in each of the practice areas of focus of the sessions (response options were a 5-point Likert scale: novice, advanced beginner, competent individual, proficient individual, and expert). Of the 71 that participated, 25 completed the survey.
Session pre-/post-data
Participant's knowledge related to transgender care was assessed at the beginning and end of each of the four sessions. Data were collected using Zoom's polling feature. Eight questions (two per session) assessed topics such as health inequities, surgical requirements, and management of both masculinizing and feminizing hormone therapies. Sample sizes varied by session.
DATA ANALYSIS
Data were analyzed using SPSS 25 software. 16 Participant demographics, professional background, and practice characteristics were analyzed using descriptive statistics. Comfort in providing care and participant's perceived competence in practice areas were analyzed using paired t-tests. The 4- and 5-point Likert scales for these questions were converted into numeric values (1 = very uncomfortable to 4 = very comfortable and 1 = novice to 5 = expert, respectively). Significance for paired t-tests was set at p ≤ 0.05. Finally, session pre-/post-knowledge questions were analyzed by comparing the percentage of participants who answered correctly. Samples for knowledge questions were not matched due to limitations of the Zoom polling at the time of the series.
Results
“Bootcamp” participants (n = 71) included 78% clinical staff or health care providers and 9% behavioral health providers (Table 2 Demographics). With more than one option available on the survey, most participants self-identified as a direct care provider (90%), primary care provider (68%), and/or Medicaid provider (68%). Almost half (44%) reported working with an underserved population and 23% in a federally qualified health center. The estimated percentage of patients on participant panels who use Medicaid or are uninsured were 0% patient (9% respondents), 1–20% (32%), 21–40% (18%), 41–60% (14%), and >60% (27%).
Participants' Demographics
Of the participants, 82% identified as cisgender females, 8% as cisgender males, 1% as transgender female, and 7% as genderqueer or gender nonconforming. Eighty-two percent identified as White, 6% as Asian, 3% as American Indian/Alaskan native, 1% as Black/African American, 1% as Middle Eastern, and 1% as “other.” States represented among participants other than Colorado included Kansas (n = 3), and one person from each of the following: Maine, Massachusetts, Montana, New Mexico, Oregon, Wyoming, and Washington, DC. Participants attended an average of 2.6 sessions out of 4, with 53% attending 3 or more and 24% attending all 4 sessions. Fourteen participants from the ongoing series were registrants for the “bootcamp” and after completion, 15 people from the “bootcamp” joined the ongoing series.
The survey data showed an overall increase in comfort providing care for both transgender patients and cisgender patients. Participants reported a 10.3% increase (2.9–3.2 on a 4-point scale, p = 0.02) in overall comfort in providing care to patients who are transgender and a nonsignificant increase (3.6–3.8 on a 4-point scale) in comfort providing care for patients who are cisgender (Fig. 1). Prescribers showed improvement in self-reported competency across four areas of practice readiness on a 5-point scale from (1) novice, (2) advanced beginner, (3) competent, (4) proficient, and (5) expert. There was a significant change (p ≤ 0.007) among prescribing providers (n = 17) across four areas of reported practice (Fig. 2). There was also an increase in knowledge as determined by percent correct (Fig. 3) in domains of health inequities (50% vs. 74% correct pre/post), gender-affirming surgeries (33% vs. 74% correct pre/post), and masculinizing and feminizing hormone therapy (55% vs. 70% correct pre/post and 64% vs. 89%, respectively).
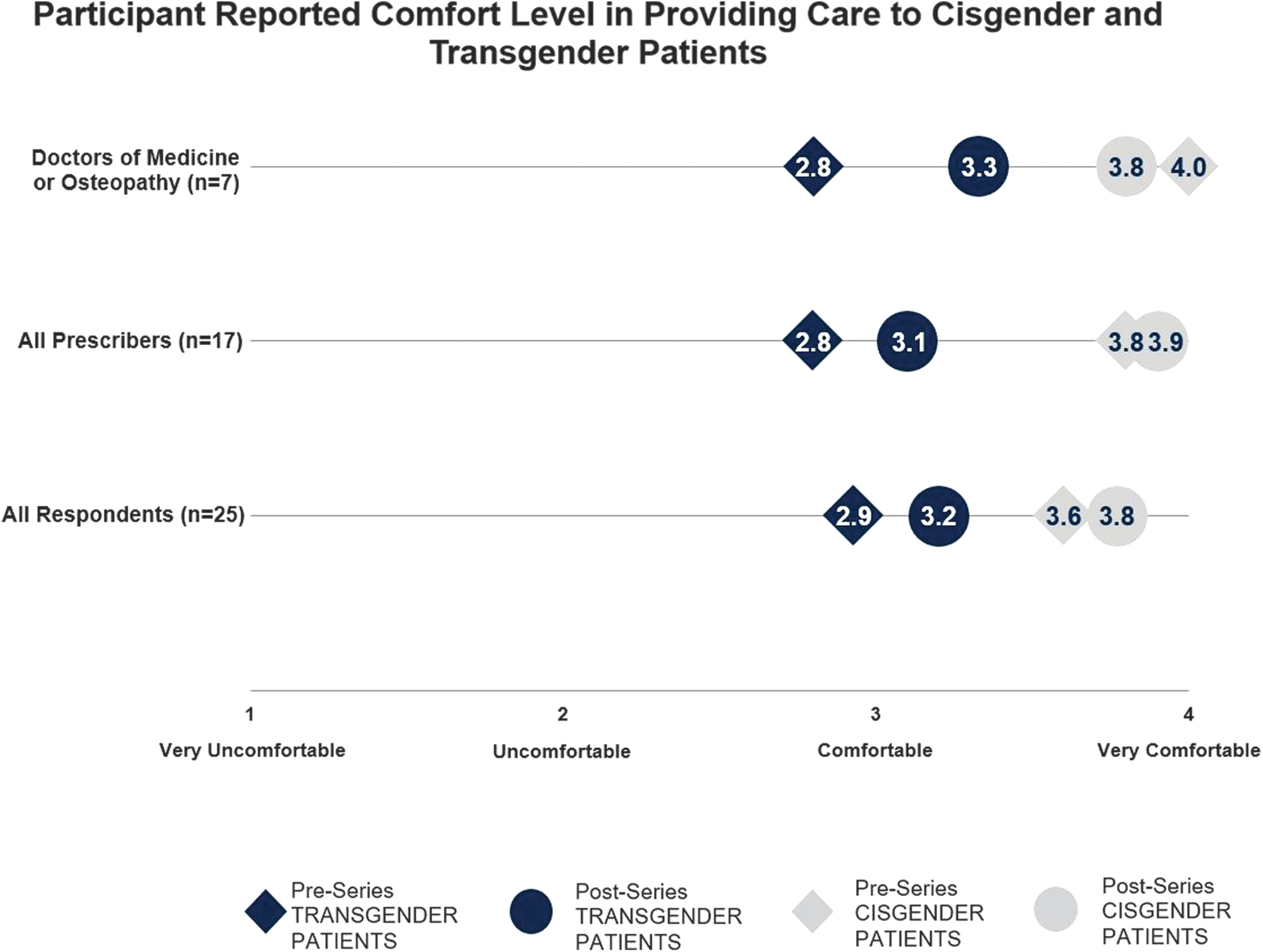
Pre- and post-comfort level.

Pre- and post-self-reported competency.
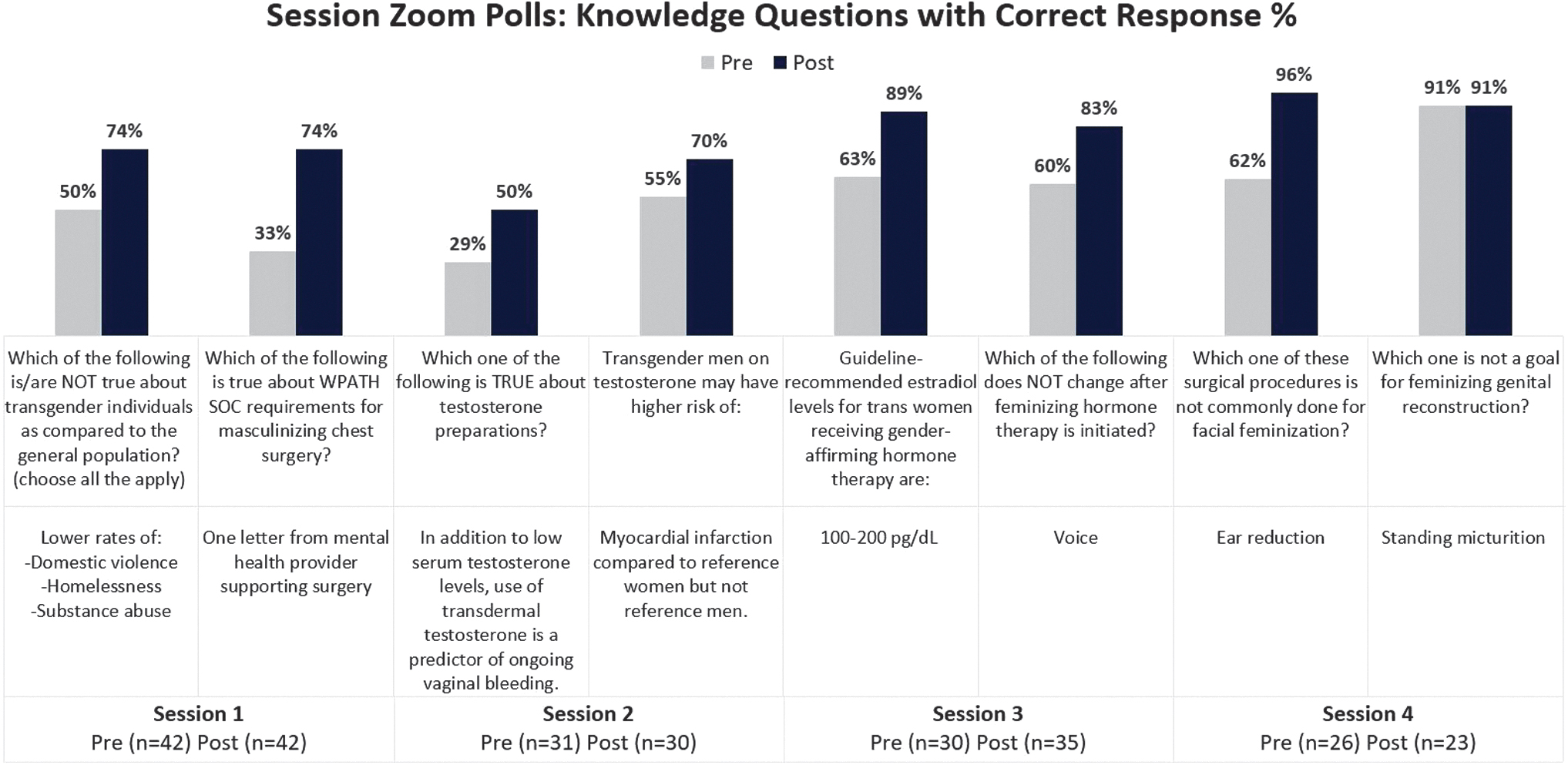
Pre- and post-knowledge questions.
Participants' qualitative responses reflected gratitude for the sessions, a desire for ongoing education and more in-depth review of many of the topics. Suggestions for improvement included expansion of the “bootcamp” to include additional content on topics such as behavioral health, pediatric/adolescent populations, addressing the determinants of health, and improving the clinic infrastructure to be more inclusive. Other challenges reported included the logistics of holding the sessions across time zones, the diverse backgrounds of participants with some feeling the content was more directed at prescribing providers, and the variation in baseline level of experience with TGD care (ranging from novice to advanced).
Discussion
After the completion of four sessions of the “bootcamp” ECHO, our respondents demonstrated increase in knowledge and reported a statistically significant increase in their self-efficacy and competence with providing primary care for transgender patients. Our results reinforce findings that the ECHO model leads to a statistically significant increase in self-efficacy and confidence in treating specific demographics and condition. 11,17
More education on TGD health is important as there is limited exposure to this training in health professional schools. 18,19 Inadequate education can then contribute to the lack of confidence and comfort of providers in treatment modalities such as gender-affirming care. Cooper et al. conducted a systematic review of 36 studies evaluating affirming and inclusive medical school training and noted that the most effective ways to increase comfort, confidence, and skills are through modalities such as case studies. 19 ECHO provides a well-studied model of education and case-based practice support whose effectiveness is consistent with these findings. Our study builds on this literature and demonstrates how a short-term curriculum can also be effective at increasing participants' sense of self-efficacy, confidence, and knowledge in managing a population needing complex care. It also points out the need for longitudinal curricula and a place where providers can discuss complex patient cases.
Previous studies have evaluated the use of telementoring for providers on topics around TGD health, but in time-limited or cohort-based series. A Veterans Health Association study showed that providers' comfort and confidence increased regarding topics of transgender health after 14 sessions over 7 months. 17 Trans ECHO, a program run out of Fenway Health in Boston, recently reported that from 2016 to 2020, their model of year-long cohorts improved self-efficacy scores and lowered perceived barriers in providing care to TGD patients. 12
These findings are consistent with previous reports of ECHO curricula in other area, such as done by Lewiecki et al., which demonstrated increased comfort and confidence after a series of 10 or more sessions. 11 In our ECHO “bootcamp” model, participants completed the number of sessions (four) and demonstrated an increase in knowledge. Given that 15 of 71 “bootcamp” attendees went on to attend the longitudinal curriculum, this demonstrates a useful way to familiarize new participants with concepts of an ongoing ECHO curriculum and allows them to join in without feeling “behind” other participants.
LIMITATIONS
Despite the overall success of this project, as defined by increasing self-efficacy, competence, and knowledge and overall program satisfaction, there are a few limitations. One limitation is response rate, with 25/71 participants responding to the post-survey questions. We suspect survey fatigue played into the limited response rate. Since the survey was sent in an e-mail after the fact as opposed to giving the survey during the final session, this may have also contributed to decreased response as participants became busy returning to their work/clinic schedules. Another limitation was that the participants were predominantly from Colorado. Although other states were represented, applicability to other regions will need to be investigated by future projects. Further research could also be warranted to evaluate the reasons why participants want to join the ongoing series or not.
Conclusions
The ECHO model is an effective tool to increase providers' comfort and knowledge with care management for TGD patients. The novel use of a “bootcamp” also highlights a way to introduce new participants to an ongoing ECHO curriculum and increase their competence in providing TGD health care. The results of this study imply this “bootcamp” model could be effective for increasing knowledge and introducing/recruiting new participants to longitudinal ECHO series on other health care topics.
Footnotes
Acknowledgments
The authors thank all attendees to the ECHO “bootcamp” for their participation and feedback. In addition, the authors would like to thank the staff of the ECHO Colorado program center, including Ashley Clark, Kristen Young, and Dr. Granger Petersen, in their roles in marketing and recruitment and in implementing, managing, and evaluating this series.
Authors' Contributions
Writing—original draft and writing—review and editing by A.H.-H. Investigation, writing—original draft, and writing—review and editing by S.J.I. and R.S.L. Investigation and writing—review and editing by D.R.S. and R.D.D. Data curation and formal analysis by N.A.C. Writing—review and editing by A.C. ECHO Program Center support allocation and writing—review and editing by J.F.T. Investigation, supervision, writing—original draft, and writing—review and editing by M.S.R.
Disclosure Statement
No competing financial interests exist.
Funding Information
Funding for this project was from the Colorado Upper Limit Payment Grant. S.J.I. received funding through a National Institutes of Health/University of Colorado Building Interdisciplinary Research Careers in Women's Health (BIRCWH) K12 grant (supported by NIH 5K12 HD057022, PIs: Regensteiner JG and Santoro NF).