
Abstract
Background:
Internet medical services (IMS) have been rapidly promoted across China, especially since the outbreak of COVID-19. However, a nationwide study is still lacking.
Objective:
To unveil the whole picture of IMS across tertiary and secondary hospitals in China, and to evaluate potential influence of the hospital general characteristics, medical staff reserve, and patient visiting capacity on IMS provision.
Methods:
An online cross-sectional survey was conducted, and 1,995 tertiary and 2,824 secondary hospitals completed questionnaires from 31 administrative regions in China during July 1 and October 31, 2021. Those hospitals are defined having abilities of providing IMS if at least one following service are available: (1) online appointment of diagnoses and treatments; (2) online disease consultation; (3) electronic prescription; and (4) drug delivery. The logistic regression models are used to detect the possible roles on developing IMS.
Results:
A majority (68.9%) of tertiary hospitals and 53.0% secondary hospitals have provided IMS (p < 0.01). Tertiary hospital also had much higher proportions than secondary hospitals in online appointment of diagnoses and treatments (62.6% vs. 46.1%), online disease consultation (47.3% vs. 16.9%), electronic prescription (33.2% vs. 9.6%), and drug delivery (27.8% vs. 4.6%). In multivariate model, IMS hospitals may be associated significantly with having more licensed doctors (≥161 vs. <161: odds ratio [OR], 1.30; 1.13–1.50; p < 0.01), having more frequency of registration appointments (≥3,356 vs. <3,356: OR, 1.77; 1.54–2.03; p < 0.01), having higher frequency of patient follow-ups (≥1,160 vs. <1,160: OR, 1.36; 1.15–1.61; p < 0.01), having laboratory test appointments (Yes vs. No: OR, 1.25; 1.06–1.48; p = 0.01), and having treatment appointments (Yes vs. No: OR, 1.27; 1.11–1.46; p < 0.01) in the past 3 months.
Conclusions:
The coverage of IMS is appreciable in China, but the IMS market is still greatly extended and improved. The provision of IMS depends primarily on the scales of the hospitals, including medical staff reserve and patient visiting capacity.
Introduction
Medical care is a critical issue that is related to national economy and people's livelihood. With rising threats of chronic diseases and the rapid increase of residents' health awareness in China, more and more prominent contradiction between supply and demand in terms of medical resources has to be faced by health source and service administrations. From the perspective of supply, however, insufficient and uneven distribution of medical resources renders it difficult to meet such rapidly growing medical demands. High-quality services are mainly provided in developed regions, while patients from less-developed regions have limited access to these high-level services due to financial pressure and inefficient resource sharing. 1 At the end of 2021, the number of graded hospitals in China has exceeded 26 thousand, but tertiary hospitals only account for 12%, which have to meet about half of medical demands in the whole country. 2
Developed countries mainly focus on the use of electronic information and telecommunication technologies to support long-distance clinical health care, patient and professional health-related education, health management, and public health. 3 –5 China initiated telemedicine since the late 1980s. 6 In 2018, more than 3,000 hospitals have been enrolled into telemedicine network across the country, and regional telemedicine centers were established across almost all of the 31 administrative regions as in mainland China at the end of 2019. 7 To a certain extent, telemedicine provides an important alternative for patients and medical institutions in remote and impoverished areas so that the gap between rural and urban in the capability and quality of medical services could be reduced. 8 However, unbalanced development of telemedicine services is still inevitable due to the disequilibrium of technical framework, the disunity of data transmission standards, and the construction of disparate system architecture across regions and health care facilities. 7,9 –12
INTERNET MEDICAL SERVICE IN CHINA
China has made remarkable achievements in controlling the COVID-19 epidemic, while the great challenge was also brought to hospitals and individuals on the access and delivery of medical services. 13 On the other hand, COVID-19 is also transforming the landscape of online health care with breathtaking speed, especially after the normalization of the epidemic. 13,14 Internet medical service (IMS) can be not only as simple as using the internet to make appointments to hospital and obtain own medical records, but also provide an alternative option of face-to-face consultation with doctors through internet pages or public therapeutic platforms, 14 the latter of which is the top priority. The online diagnosis consultation and return-visit treatment are not just provided by registered hospitals to patients, and group consultation across various hospitals and/or various specialties by using online health care platform are also included in China. 9 In addition, auxiliary services regarding online appointments and mobile payment aim at taking advantage of the convenience of the internet to improve the quality and efficiency of medical service in hospital environments. 15
Hence, IMS has great potential in alleviating this prominent contradiction due to the shortage of medical resources and large disease burdens of population base in China.
OBJECTIVE
At present, most studies on Chinese online services focuses on specific diseases, 11,16 –18 regional online services, 7,9,19 and patient satisfaction surveys. 20,21 A recent national study reported the development of IMS from multiple aspects based on 161 tertiary hospitals across 29 provinces, autonomous regions, and municipalities in mainland China. 12 However, although tertiary hospitals are the main providers of IMS, governments have made great efforts to promote IMS in secondary hospitals over the past few years. A nationwide survey of overall status quo and influencing factors for IMS is needed. Therefore, we aim to conduct a multidimensional survey to unveil the whole picture of IMS in the whole of mainland China. Additionally, potential influence factors are explored for further IMS improvements and scalabilities.
Methods
HOSPITAL RECRUITMENTS
An online questionnaire was made available on the website of the Intelligent Hospital Grading Evaluation Platform by the National Institute of Hospital Administration, National Health Commission of the People's Republic of China. According to the reports released by the National Center for Health Statistics Yearbook 2022, 10,404 secondary and 2,996 tertiary hospitals have been recorded at the end of 2020, 2 who were eligible to be recruited into this study and voluntary response sampling was used. Each hospital had only one opportunity to fill in the questionnaires, and staffs in charge of the relevant works were required to provide the data in the questionnaire. Finally, a total of 5,337 hospitals completed the questionnaire from July 1, 2021 to October 31, 2021. The questionnaires from 4,819 hospitals (90.3%) were complete and valid, among these 2,020 hospitals are located in the Eastern regions, 1,139 hospitals in the Central regions, and 1,660 hospitals in the Western regions. The numbers of secondary hospitals and tertiary hospitals were 2,824 and 1,995, respectively.
DATA COLLECTION
This is a cross-sectional study to collect the following data: (1) basic hospital information: hospital name, location, the grade of the hospital, and the type of hospital; (2) medical staff reserve: licensed doctor numbers, licensed nurse numbers, and licensed pharmacist numbers; (3) patient visiting capacities in the past 3 months: total visiting appointment frequency and its components, including patient registration, inpatient application, follow-ups, referrals, laboratory testing, imaging, treatment, outpatient surgery, etc.; and (4) available ranges of IMS: those hospitals are defined having abilities of providing IMS if at least one following service are available, including online appointment of diagnoses and treatments, online disease consultation, electronic prescription, and drug delivery. Otherwise, hospitals are defined as having no abilities, if any one service is not chosen.
STATISTICAL ANALYSES
Data were processed and analyzed by the Statistical Analysis System software 9.4 (SAS Institute, Inc., Cary, NC). Due to skewed distribution, quantitative variables are shown as the median and interquartile range, and qualitative variables as percentages (%) and numbers. The primary outcome is the prevalence of IMS hospitals. Four secondary outcomes of IMS components are also assessed, including online appointment of diagnoses and treatments, online disease consultation, electronic prescription, and drug delivery. The comparison between hospitals with and without IMS was conducted using the two-sample nonparameter Wilcoxon tests for continuous variables and the chi-square tests for categorical variables. Unconditional logistic regression models were used to calculate odds ratios and corresponding confidence intervals (CIs) for IMS and its potential factors. Continuous variables were transferred into dichotomous variables using respective medians, which are further taken as variable selection for stepwise approach, if significance is at the level of 0.20 under univariate analyses. Subgroup analyses are conducted by hospital grades.
Results
THE PREVALENCE OF IMS
Overall, 4,819 hospitals were used for final analyses, among which 59.6% (2,871/4,819) have provided at the least one IMS. IMS are much higher in tertiary hospitals than secondary hospitals (68.9% vs. 53.0%, p < 0.01). The geographical China map are segmented into the Eastern, Central, and Western regions, indicating 43.8% hospitals recruited in the Eastern regions, 30.2% in the Central regions, and 41.0% in the Western regions (the top of Fig. 1). IMS provision in the Eastern regions (63.1%) is much higher than that in the Central regions (56.8%) and Western regions (57.2%). The variations were observed across 31 administrative regions, which are illustrated on the bottom of Figure 1. Among the Top 10 provinces of IMS ranking, 6 are located in the Eastern regions (Zhejiang, Shanghai, Jiangsu, Beijing, Shandong, and Tianjin), 2 from the Central regions (Hubei, and Shanxi), and 2 from the Western regions (Ningxia, and Xinjiang).
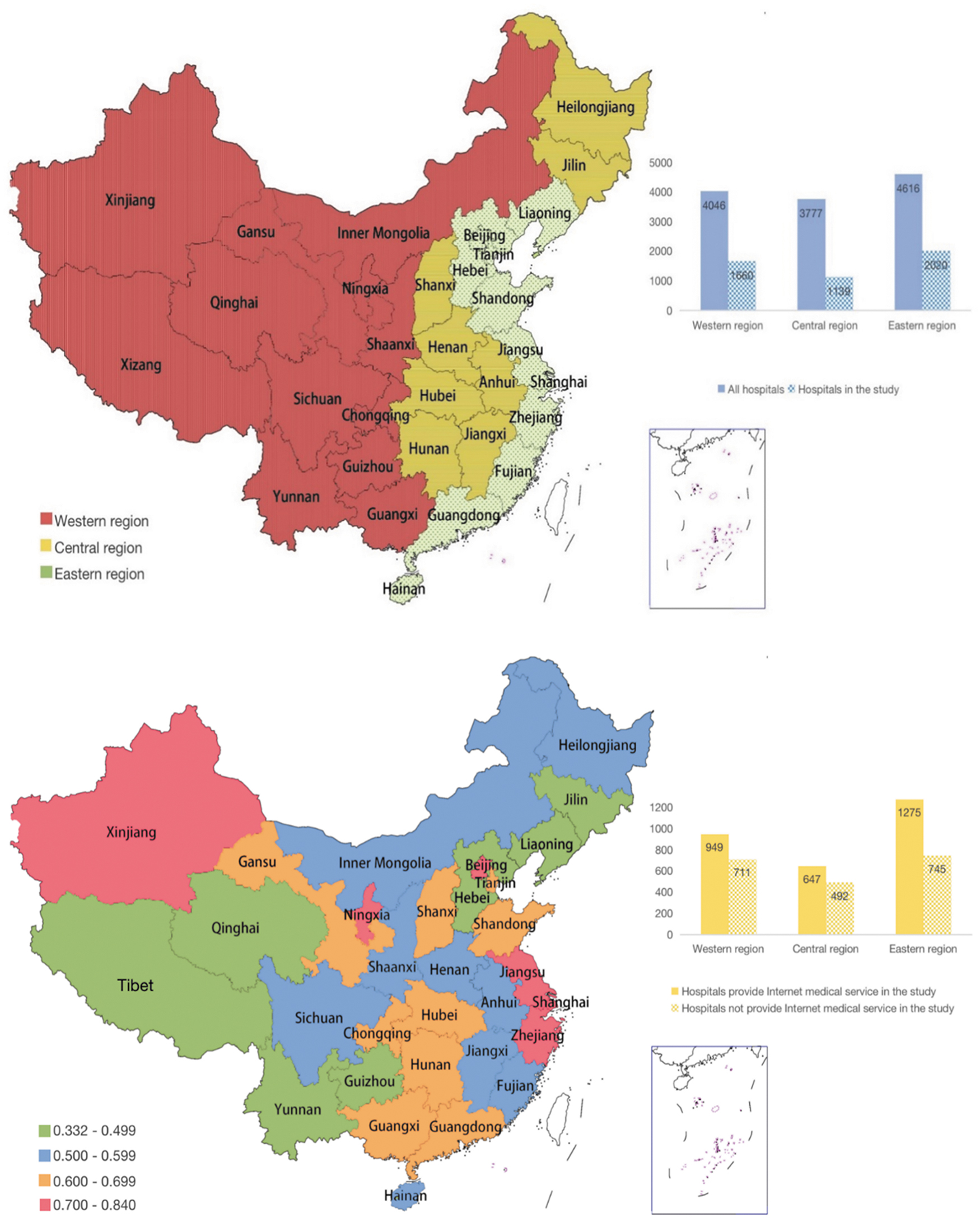
China map for the prevalence of IMS hospital. IMS, internet medical service.
Tertiary hospital also had much higher proportions than secondary hospitals in online appointment of diagnoses and treatments (62.6% vs. 46.1%; p < 0.01), online disease consultation (47.3% vs. 16.9%; p < 0.01), electronic prescription (33.2% vs. 9.6%; p < 0.01), and drug delivery (27.8% vs. 4.6%; p < 0.01), which is illustrated on the top of Figure 2. The bottom of Figure 2 exhibits the difference of IMS component numbers between tertiary hospitals and secondary hospitals (p < 0.01), and the prevalence of all four IMS component provision is much higher in tertiary hospitals than that in secondary hospitals (25.5% vs. 3.0%).

The comparison of IMS components between tertiary and secondary hospitals.
COMPARISON BETWEEN IMS HOSPITALS AND NON-IMS HOSPITALS
Table 1 compares the difference in general characteristics among hospitals with and without IMS, and hospitals in Eastern regions have significantly higher IMS coverage (63.1%) than that in the Western (56.8%) and Central regions (57.2%), which is more pronounced in tertiary hospitals (73.7% vs. 63.7% and 65.4%, p < 0.01). However, no significant difference is detected in secondary hospitals (45.6% vs. 42.8% and 45.0%, p = 0.65). The comparisons are conducted between specialty hospitals and general hospitals, as well as between public hospitals and other hospitals, but it has failed to find a significance (p > 0.05). IMS hospitals have much more licensed medical staffs and higher frequency of patient visiting in the past 3 months than non-IMS hospitals, including patient registration, inpatient application, follow-ups, referrals, laboratory testing, imaging, treatment, outpatient surgery, and other relevant medical services, in which significance was kept in tertiary and secondary hospitals (all p < 0.01).
General Characteristics Among Chinese Hospitals Providing and Not Internet Medical Services by Hospital Grade
APM, appointment.
IMPACT FACTORS FOR TOTAL IMS PROVISION
Table 2 presents the results from the univariate logistic regression models for IMS, and significant difference was detected between IMS hospitals and non-IMS hospitals in almost all possible factors, except in hospital types (general hospitals vs. specialty hospitals) and public hospitals (Yes vs. No). It is worth mentioning that tertiary hospitals in the Eastern regions have higher IMS proportions than those in Western and Middle regions (p < 0.05), while secondary hospitals have similar levels in IMS across various regions (p > 0.05). Multivariate logistic regression models in Figure 3 revealed that hospitals were considered to be more possible to provide IMS if they have more than 161 licensed doctors (adjusted odds ratio [AOR], 1.30; 95% CI, 1.13–1.50; p < 0.01), registration appointments are larger than 3,356 in the past 3 months (AOR, 1.77; 95% CI, 1.54–2.03; p < 0.01), patient follow-up frequency in the past 3 months is >1,160 (AOR, 1.36; 95% CI, 1.15–1.61; p < 0.01), hospitals can offer laboratory test appointments (AOR, 1.25; 95% CI, 1.06–1.48; p = 0.01), and treatment appointments (AOR, 1.27; 95% CI, 1.11–1.46; p < 0.01).
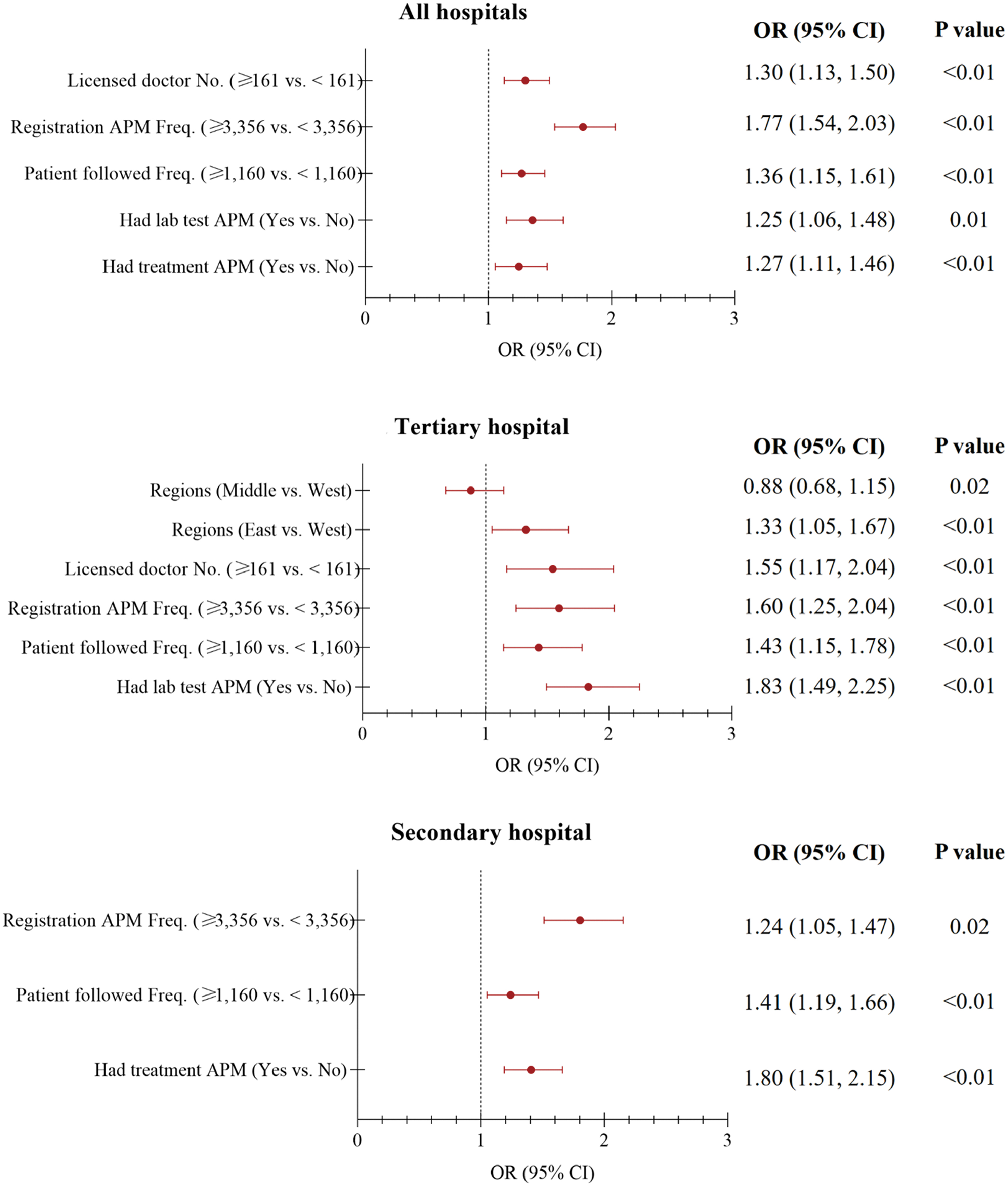
Adjusted associations of IMS with its potential influence factors by hospital grades.
Univariate Odds Ratios and 95% Confidence Intervals for Internet Medical Services and Its Potential Impact Factors
CI, confidence interval; OR, odds ratio.
Besides abovementioned influence factors, in subgroup analyses by hospital grades, tertiary hospitals in Eastern regions were more likely to conduct IMS relative to those in Western regions (AOR, 1.33; 95% CI, 1.05–1.67; p < 0.01). However, licensed doctor numbers and having treatment appointment are not independent factors for IMS in secondary hospitals.
IMPACT FACTORS FOR FOUR IMS COMPONENTS
Four IMS components are also analyzed separately as sensitivity analyses. Figure 4 illustrates multivariate analysis results for four IMS components, and there are three independent factors for all four IMS components, including hospital grades, registration appointment frequency, and had treatment appointment.
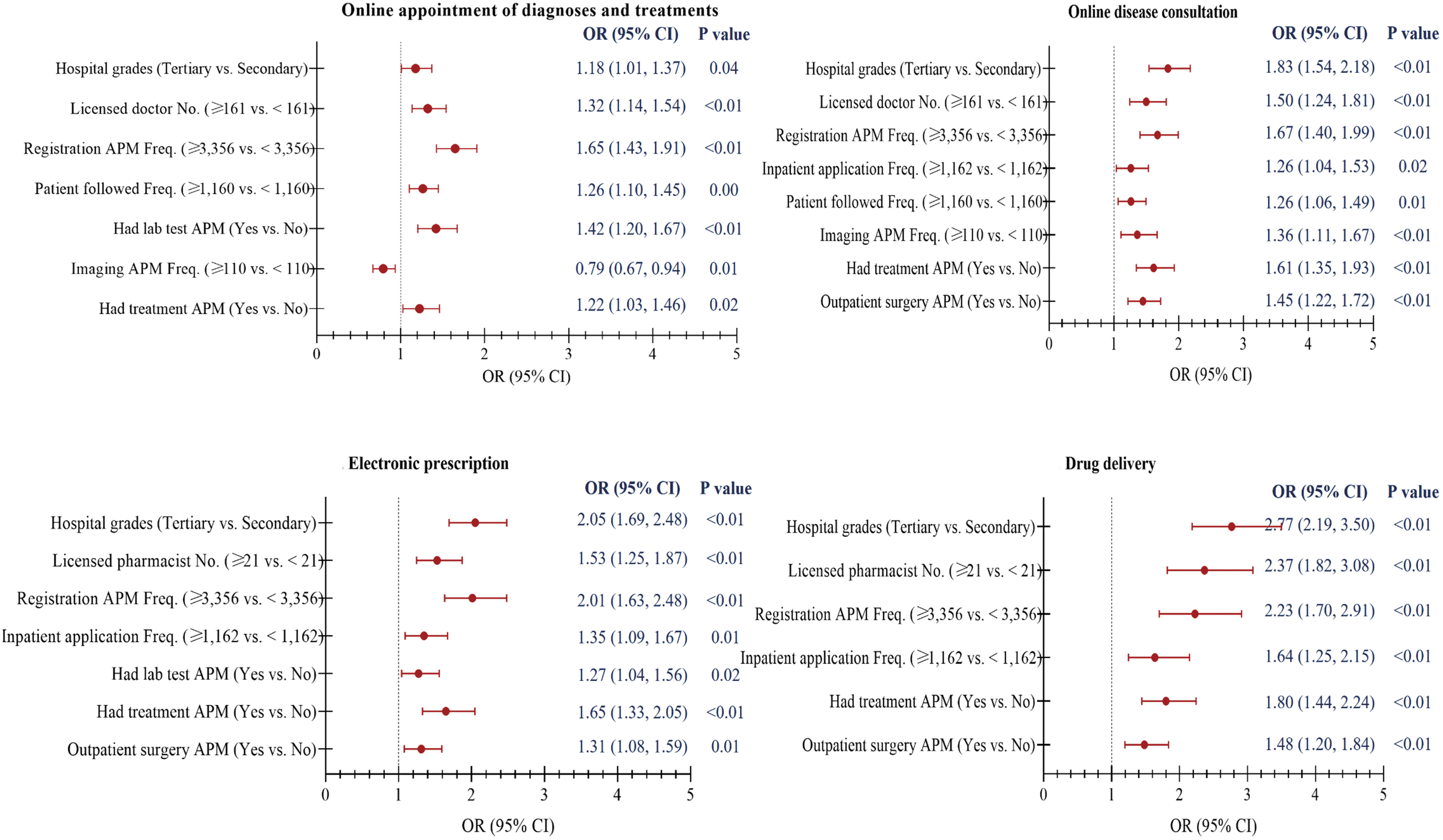
Adjusted associations of IMS with its potential influence factors by IMS components.
Higher inpatient application frequency and outpatient surgery appointment are detected as predictors for three IMS components, including online disease consultation, electronic prescription, and drug delivery. Hospitals having more licensed doctors, higher patient followed frequency and imaging appointment frequency are likely to provide online appointment of diagnoses and treatment, and online disease consultation. If electronic prescription (AOR, 1.53; 95% CI, 1.25–1.87; p < 0.01) and drug delivery (AOR, 2.37; 95% CI, 1.82–3.08; p < 0.01) are available, enough licensed pharmacists are being employed by hospitals.
Laboratory test appointment is found as an independent factor for hospitals with online appointment of diagnoses and treatments (AOR, 1.42; 95% CI, 1.20–1.67; p < 0.01), together with electronic prescription (AOR, 1.27; 95% CI, 1.04–1.56; p = 0.02).
Discussion
PRINCIPAL FINDINGS
This is the first study to analyze the development of IMS in 1,995 tertiary and 2,824 secondary hospitals across 31 provinces, autonomous regions, and municipalities of mainland China. In addition, we also evaluate the potential roles of the hospital general characteristics, medical staff reserve, and patient visiting capacity on IMS provision in medical institutions. Around 68.9% tertiary hospitals and 46.1% secondary hospitals have abilities to provide IMS to patients in 2021, and tertiary hospitals also possess more substantial capacities in the diversity of IMS than secondary hospitals, especially for tertiary hospitals in the Eastern regions. Adequate medical staff reserves together with sufficient patient visits and appointments seem to be the foundation for hospitals to provide IMS.
To our knowledge, however, uniform standards and definitions are lacking for IMS in China so far. Our study pioneers to consist IMS of four constituents based on the classification of internet hospital services and national policy documents, 14,22 including online appointment of diagnoses and treatments, online disease consultation, electronic prescription, and drug delivery. In our study, 59.6% hospitals have provided at least one IMS. On the whole, IMS development in the Central (56.8%) and Western regions (57.2%) basically lags behind the Eastern regions (63.1%), and the hospital grade is also an important factor affecting the IMS implementation. Tertiary hospitals in Eastern regions had about 10% higher IMS coverage than that in Western and Central regions in 2021, while secondary hospitals across these 3 regions have similar IMS coverage at around 42%, which may be owing to the imbalanced dispensation of health technicians and medical resources between tertiary and secondary hospitals in developed regions.
On the contrary, IMS development in secondary hospitals have fallen behind, even though in developed regions. After an initial period of development in IMS, therefore, more medical resources should be assigned to low-grade medical institutes, and tertiary hospitals are also responsible for heading and assisting secondary hospitals in IMS development as well as the diagnoses and treatments of complicated and miscellaneous diseases. 7 Additionally, our study also found that between-provincial disparity of IMS development is obvious within regions, which depends on local economic levels and policy orientation. 23 It is particularly obvious that Xinjiang and Ningxia have over 70% IMS provision, ranked the third and fifth among 31 administrative regions, since the “internet + medical and health” policies were explored as typical area of the Western China since 2016. 22,24 To accelerate digitization course of medical institutes in the whole China, policy orientation is needed to decrease the gaps between developed and developing regions. 8
Registration difficulties and/or long waiting times to see a doctor is problematic in China, especially for famous experts in tertiary hospitals, and the Chinese government launched Web-based appointment systems (WAS) to provide a solution to outpatient appointments and services since 2009 as a part of nationwide health care reforms. 25 –27
Internet provides convenience for traditional medical services, which could help patients to operate online to simplify offline procedures of diagnosis and treatments, including intelligent guidance, registration, mobile payment, inspection report query, cost query, medical feedback, and health education. 28 Online appointment of diagnoses and treatments are the most popular IMS components, in which tertiary hospital had much higher proportions than secondary hospitals in our study (62.6% vs. 46.1%), which depends mainly on the numbers of licensed doctors and the appointment frequencies of patient registration, follow-up, laboratory tests, imaging, and treatment.
Hence, the construction of the comprehensive appointment system does not seem urgent now in less-developed regions and low-grade hospitals due to low outpatient volume. In other words, the developments of online appointment in Chinese hospitals are still structured as complements to traditional health care procedures, not the goal of completely digitizing the entire medical service system in China. Therefore, appropriate policy orientation and incentive mechanism may be beneficial for the implementation of comprehensive appointment system in underdeveloped regions.
Besides, the number of licensed technicians plays a significant role in the IMS development. China has strict regulations that online medical consultants need at least 3 years of clinical experiences, and only prescription for common diseases and chronic disease are allowed to provide online. 29
It makes no doubt that online consultation, electronic prescription, and drug delivery are mainly supplied by professional physicians and pharmacists. In these respects, tertiary hospitals have more advantages in the number of licensed medical staffs than secondary hospitals. Our results also confirm this common view, indicating that tertiary hospitals had absolute predominance in online disease consultation (47.3% vs. 16.9%), electronic prescription (33.2% vs. 9.6%), and drug delivery (27.8% vs. 4.6%), compared with secondary hospitals, all of which may be prosperous directions of IMS development during and after consultation in the future. However, IMS goes beyond these. More IMS components should be expanded, such as online nursing, online disease management, and online medicine training and sharing, etc. 14,30 –34
Besides medical technicians, more supporting technicians should be recruited to promote IMS diversities further, who are proficient in the infrastructure construction, medical information technology, and backend operation and management.
LIMITATIONS
Our study has several limitations. First, although this study is a national hospital survey and hospitals across 31 administrative regions were included, voluntary response sampling was used to collect data from July 1, 2021 to October 31, 2021. The generalization of the results still needs caution. Second, a cross-sectional study was conducted; verification of causality hypothesis is needed by a cohort study. Moreover, IMS in China is still at a rapid developing stage, and dynamic change of IMS in various hospitals may be large in 2022. Another survey is planned, and more contents will be added into new questionnaire, including IMS costs, preferences of online health care across various clinical divisions, and the differences between first consultation and follow-up consultation services. Third, this study mainly focused on hospitals rather than patients or doctors, so the specific needs of patients and the willingness of doctors were not investigated, which are also important to improve the quality and diversity of IMS.
Finally, potential role of hospital levels, medical staff reserve, and patient visiting capacity on IMS provision were performed using traditional stepwise strategies, but model efficacy are not enough owing to some possible factors not considered, such as the hardware and software, supporting infrastructure for IMS implementation.
Conclusions
Based on the data of 4,819 tertiary and secondary hospitals nationwide, this study makes a quantitative analysis for the status quo of IMS in China, and further confirms that tertiary hospitals are providing higher quality of IMS and more multifarious IMS than secondary hospitals. The IMS development of medical institutes is largely determined by hospital levels, medical staff reserve, and patient visiting capacity. However, the policy-oriented role is equally important, especially in the Western regions. Therefore, individualized IMS implementation and extension should be considered to decrease the gaps between developed and less-developed regions as well as between tertiary and secondary hospitals.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.