
Abstract
Background:
Telemedicine can be defined as the use of telecommunication technology for performing medical acts remotely by health professionals. Currently in anesthesia, teleconsultation (TC) is becoming widespread, although the benefit and quality have not been well evaluated. The objective of this study was to assess the quality, the patient satisfaction, as well as the ecological and medicoeconomic impacts of the preanesthesia TC.
Methods:
This prospective observational multicentric study was approved by the Société Française d'Anesthésie-Réanimation ethics committee. The study took place from October 2020 to March 2021, in eight French health care institutions. Every adult patient requiring TC before elective surgery could be included. Unavailability of videoconferencing for the patient was the main exclusion criteria. Five hundred three (n) patients, scheduled for surgery, were included. Their files were analyzed for quality, 375 were successfully interviewed for the second part of the study evaluating satisfaction and medicoeconomic impact. The study's evaluation criteria were the quality of the TeleMed-Cs, the satisfaction and comprehension for the patient, and the medicoeconomic impact of a remote evaluation compared with the face-to-face consultation with the surgeon.
Results:
Of the 503 files, 478 (95%) were reviewed and met all the high authority of health quality criteria. The electronic format of records was associated with higher completion rate. The median satisfaction was 10.0 (IQR 8.25–10.0). The cost of a TC in anesthesia was significantly lower than that of a face-to-face surgical consultation with a median cost of 1.49€ (IQR 0.8–1.99) versus 34.81€ (IQR 14.01–91.7) p < 0.001.
Conclusions:
TC in anesthesia seems to be a good alternative in terms of quality, patient satisfaction, and medicoeconomic gain for our patients. By facilitating access to preoperative evaluation, it could be adopted worldwide and thus reduce surgery-related morbidity and mortality in our patients.
Keypoints
Teleconsultation (TC) is quickly becoming more widespread in anesthesia.
TC could have a medicoeconomic benefit while maintaining quality and security.
Making the consultation accessible to all could strengthen safety in anesthesia.
Introduction
Telemedicine can be defined as the use of telecommunication technology for performing medical acts remotely by health professionals. The application of this practice in the field of anesthesia expands to preoperative assessment and patient preparation, remote perioperative monitoring, and postsurgical follow-up. 1
The first cases of preanesthesia teleconsultation (TC) were reported in 2004. 2 It was initially attempted for patients living in rural areas with difficult access to tertiary health care centers. 2,3 TCs could be a promising alternative to inpatient consultations in the era where technology has been making remote communication accessible, effective, and comfortable.
In 2020, the world faced the COVID-19 pandemic, 4,5 as a consequence, a spike in preanesthesia TCs was observed in the following months in hopes of reducing hospital visits and the risk of exposure to potentially contagious patients and staff. 6,7 Although TCs were widely used in 2020, their quality and benefits have not yet been evaluated.
In this study, we aimed to assess the quality of the preanesthesia evaluation by TCs, through the patient satisfaction questionnaire, as well as the ecological and medicoeconomic interests/impacts.
Methods
This prospective multicentric study, involving no risk or constraint, was approved by the Société Française d'Anesthésie-Réanimation ethics committee (IRB 00010254-2021-113).
All patients were informed of the collection of their data in a dedicated register and gave an oral consent.
From October 2020 to March 2021, patients scheduled for elective surgery were included consecutively. Eight health centers were involved: three public hospitals (Pitié-Salpetrière Hospital APHP Paris, Saint-Antoine Hospital APHP Paris, Cochin Hospital APHP Paris) and five private clinics (Clinique Drouot Sport and Arthrose Paris, Clinique Jouvenet Paris, Clinique du sport Mérignac, Clinique Lille-Sud Lesquin, Groupe des cliniques Saint Roch et Clémentville Montpellier). Every adult patient requiring TC before surgery was eligible to be included, however, unavailability of videoconferencing capability for the patient was the main exclusion criteria.
The TCs were defined as a videoconference between the patient and an anesthesiologist without assistance of another health professional (i.e., a nurse). In all participating centers, TCs were carried out through a dedicated website (Medaviz, Doctolib, ORTIF), approved for telemedicine. The consultation data were recorded on a dematerialized file in a dedicated software, or in paper format.
OUTCOMES AND DATA COLLECTION
The quality of the TCs was assessed using the French health authority quality criteria, which should be present in an anesthesia record: patient identity, practitioner identity, patient's treatment, American Society of Anesthesiologists Classification (ASA) status, anesthesia technique, and upper airway evaluation. TC medical reports of preanesthesia evaluation were reviewed by two investigators. One point was attributed for each criterion. Basic patient characteristics, as well as type of intervention, were also recorded.
In the second part of the study, we attempted to contact all the patients, and when successful these files were those we analyzed for quality. During this phone call, always made before the surgery, the following information/characteristics were collected: professional status, distance between home and hospital, technical difficulties encountered during the TC, and the need of assistance to carry out the TC.
Then two specific questionnaires on a subsection of the cohort were carried out.
Some patients were questioned on satisfaction, information received, and their understanding of the preoperative instructions. We used an eight question 5-point Likert scale questionnaire to assess patient satisfaction (Supplementary Material Appendix SA1). The items of the questionnaire were inspired by two validated scores: EVAN G score (autoquestionnaire for satisfaction of general anesthesia) and G-MISS questionnaire. 8,9 Only questions applicable to preanesthesia evaluation were used, covering multiple domains (information, comprehension, satisfaction, and relief).
Comprehension was evaluated by question number 8 (“I know how to prepare myself for surgery (ex: if I need to manage my medication, do additional lab work, fast before surgery?”) and by asking the patients whether they remember the type of anesthesia they would undergo as well as the fasting rules. A satisfaction score of 0 to 10 was also noted.
Another part of the cohort was questioned on medicoeconomic and ecological criteria: occupation, salary range, days off requested, need for an accompanying person, time taken for the TC, and purchase of additional materials for TC (i.e., equipment and internet package). In addition, the elements related to the corresponding face-to-face surgical consultation were noted: time spent in the structure, time in consultation, mode of transport, and accompanying person.
Each patient would be his or her own control to evaluate the difference between the cost of the anesthetic TC and the cost of the face-to-face consultation with the surgeon. The distance between the patient's home and the hospital as well as the type of vehicle used made it possible to calculate the carbon impact of a trip compared with the carbon impact of a TC.
To summarize, all the files were analyzed for the quality criteria but only one group of patients participated in the satisfaction and comprehension questionnaire while the other group was questioned only on the medicoeconomic and ecological data.
We decided to evaluate the medicoeconomic aspects and the satisfaction–understanding aspects separately to limit the length of the phone evaluation to <5 min to maximize the number patients willing to participate.
To finish, we asked one designated anesthesiologist at each health center to fill out a questionnaire describing the practice of TC at their location. This would allow for a more accurate and careful interpretation of the results since the methods employed are often different at each establishment.
STATISTICS
Data were collected using a spreadsheet program (Microsoft Excel®). Data analysis was performed with R® software (R Foundation for Statistical Computing, Vienna, Austria) version 3.4.3.
For quantitative variables, the median as well as the first and third quartile will be presented. For qualitative variables, the number over the total number and the percentage will be presented.
We performed a univariate statistical analysis to evaluate the factors influencing the completion rate of the files and patients' satisfaction. For the categorical variables, a χ 2 test was used if the conditions of validity were met or a Fisher test in other cases. For quantitative variables, nonparametric tests were performed (Mann–Whitney test). Logistic regression model was used to analyze the factors that could explain a patient's preference for TC versus in-person visit.
Concerning the difference in costs, due to a quantitative variable on a matched sample (each patient having their own parameters), we proceeded with a Wilcoxon test.
A p-value <0.05 is considered statistically significant.
Missing data were excluded from the analyses.
The sample size was not predetermined.
Results
Between October 2020 and March 2021, 503 files were analyzed for quality criteria. Among these patients, we managed to contact 375 (75%) of them, 200 (40%) answered the questionnaire on medicoeconomic and ecological impact of TC and 175 (35%) answered the questionnaire evaluating satisfaction and understanding (Fig. 1).
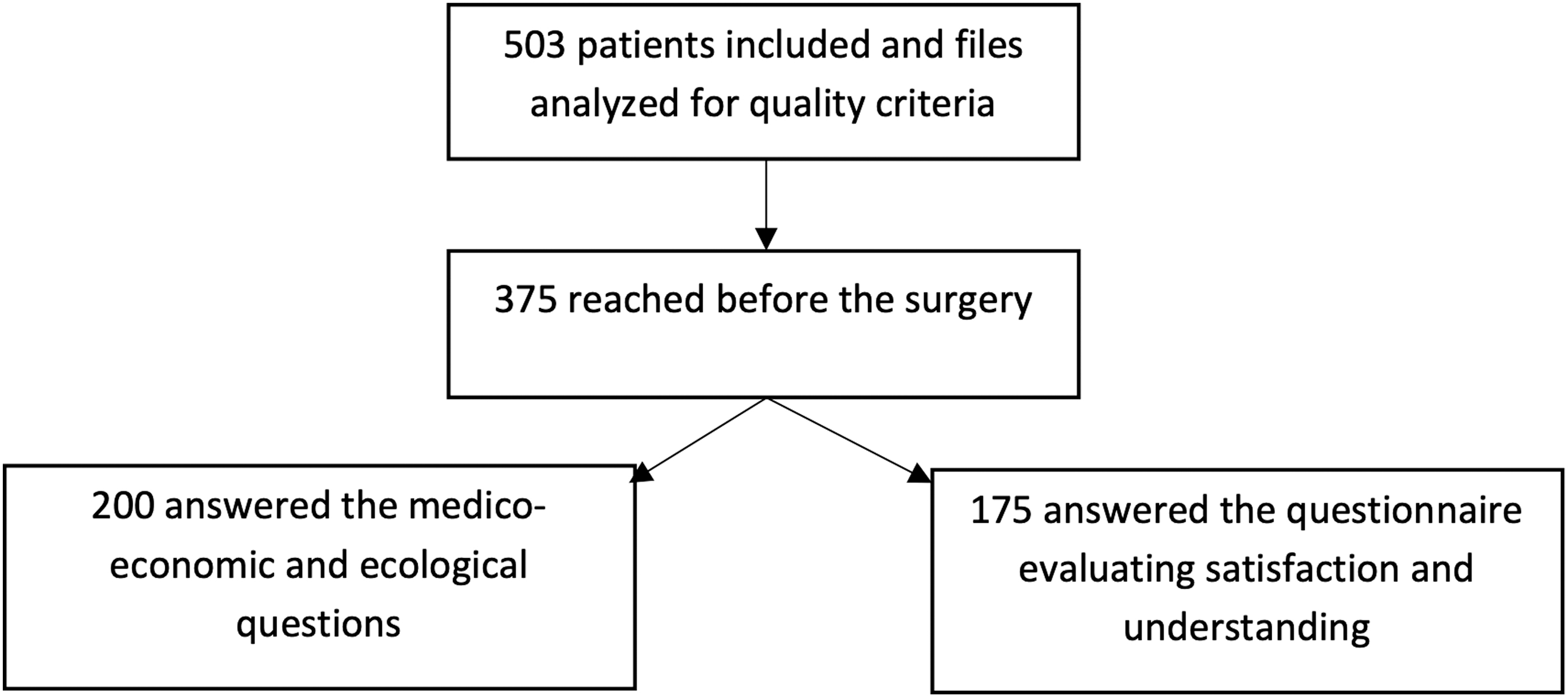
Flow chart included patients and reachable patients.
The characteristics of the patients are reported in Table 1. The median age of the patients was 43 years (IQR 31–54), 271(54%) were male gender, mostly ASA status 1 305 (61%), attending an orthopedic surgery 453 (90%). Most of the preanesthesia evaluation was computerized (E-file) but 49 of 503 (9.8%) were not.
Baseline Characteristics of the Patients
ASA, American Society of Anesthesiologists Classification.
A majority of the files reviewed, 478 of 503 (95%), have met all of the French high authority of health (HAS) quality criteria for preanesthetic evaluation. In terms of items found, 2,989 quality items were present out of a maximum of 3,018 possible (99%). Higher age, higher ASA status, and electronic rather than paper anesthesia records were associated with a higher rate of completion (Table 2). After adjusting, the electronic format of records was still associated with higher completion rate 6.49 (2.56–15.7) p < 0.001 (Table 2).
Factors Associated with Completion of Preanesthetic Evaluation
Bold text represents statistically significant p values (p < 0.05).
The median satisfaction was 10.0 (IQR 8.25–10.0). Greater satisfaction was associated with a nonworking status (p = 0.043) (Supplementary Material Appendix SA2), but neither distance (p = 0.23) nor age (p = 0.86) was associated with patient satisfaction (Supplementary Material Appendix SA3).
A small number of patients, 30 of 175 (17%), reported not being informed of the risks associated with anesthesia. With the exception of one patient, all patients understood the type of anesthesia they would receive (general or locoregional). The rules of fasting were understood by 98% of patients. There was a statistical association between understanding of the preoperative instructions and satisfaction with the TCs (p < 0.001).
Regarding the medicoeconomic and ecological impacts of TC, the average cost of a TC in anesthesia was significantly lower than that in a face-to-face surgical consultation (Fig. 2): with a median cost of 1.49€ (IQR 0.8–1.99) versus 34.81€ (IQR 14.01–91.7) p < 0.001.
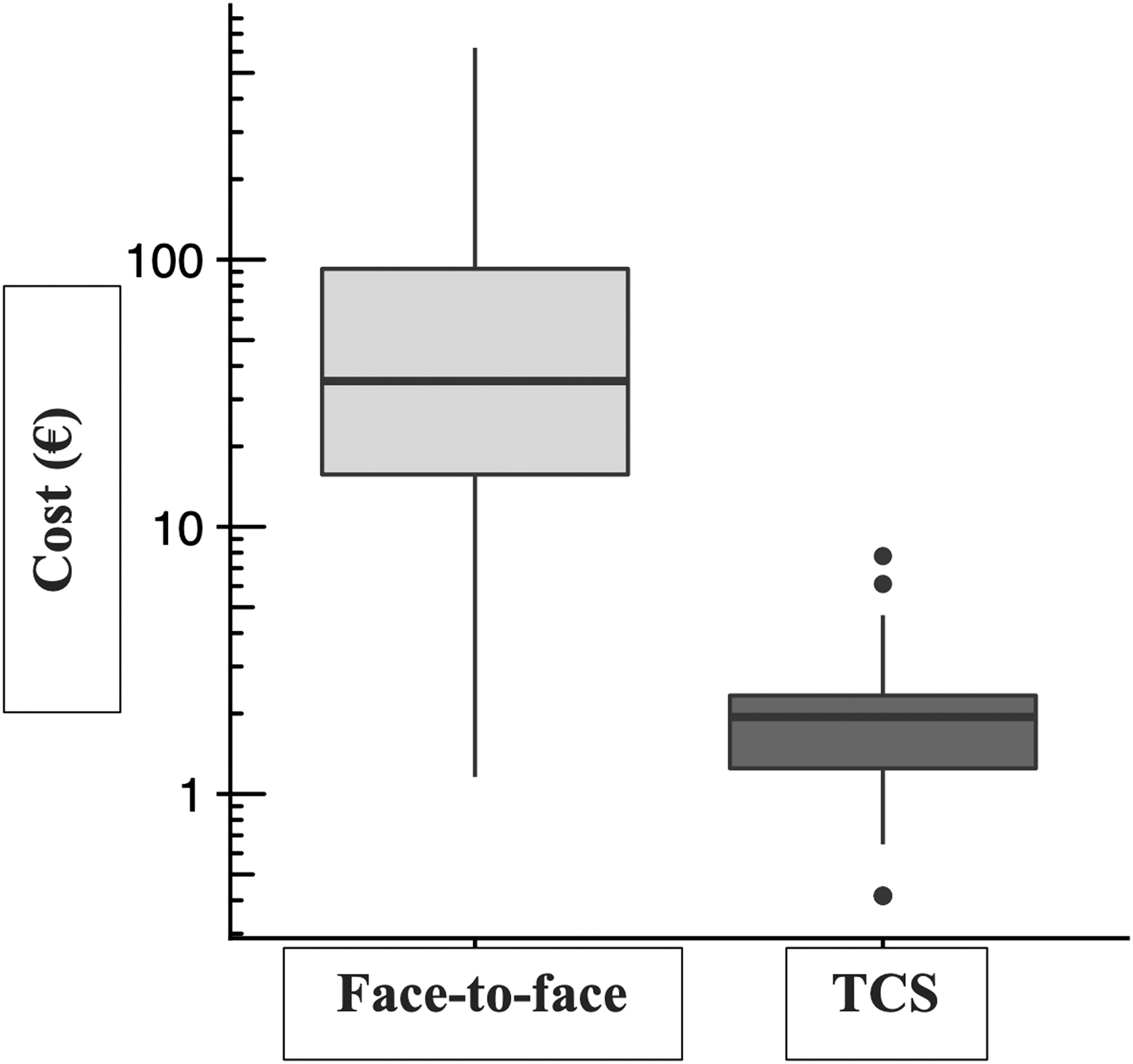
Box plot (logarithmic scale) comparing the cost (€) of consultations according to the type of consultation performed (TC: teleconsultation).
The majority of the cost difference can be explained by the cost of transfer. We, therefore, analyzed in detail the cost of transport in face-to-face consultations. We found a median cost of 22.4€ (IQR 5.56–77.15).
Salary loss was also compared between the two groups. We found a significantly lower loss of salary in the TC group with a median loss of 1.04€ (IQR 0.35–1.3) against 16.67€ (IQR 13.54–29.17) for the face-to-face consultation group.
The time spent was significantly lower for the anesthesia TC. We, therefore, calculated the difference in time spent between the two types of consultation and found a median time saved of 122.5 min for the patient (IQR 78.75–226.25).
The carbon impact of the two types of consultation was calculated and showed a clear advantage for TC with a median total mass emitted of 0.02 kg of CO2 (IQR 0.02–0.02) in the TC group against 3.86 kg of CO2 (IQR 0.03–19.3) in the face-to-face consultation group.
One hundred seven patients were asked about their willingness to have the same type of consultation with their surgeon, 70 (65%) patients agreed to this but 37 patients (35%) did not wish to have their surgical appointment through TC.
Discussion
In this study, TCs in anesthesia appear to be a good quality solution for preanesthesia evaluation by maintaining the respect of the quality criteria according to the French HAS while bringing satisfaction to the patients, providing the necessary information, and making savings both on the economic and ecological levels.
According to our information, this study is the first to evaluate anesthesia TC in its entirety and attempt a comparison with a consultation. However, our study is subject to numerous biases.
First of all, the evaluation of quality according to the HAS criteria is an evaluation based on criteria that are mainly medicolegal and does not take into consideration the quality of physical examination/clinical scenario of the patients. It would have been more interesting to know whether the Mallampati score evaluated by videoconference was correlated with the Mallampati score evaluated before entering the operating room rather than only assessing the Mallampati score by itself.
We could have also taken as a quality criterion the rate of surgery cancellations due to incorrect preoperative management for patients seen in TC and compared it with face-to-face consultations. However, this double study had already been carried out in part by Applegate et al. in the United States and did not find any difference in the rate of cancellations or postponement or in the prediction of a possible difficult intubation. 10
Another weakness of our study is that we only considered the medicoeconomic gain centered on the patient and not on the structure. We have not considered the benefits for the health care facility: personnel, cost of equipment for the center, etc. This could be the subject of a second study. It should be noted that we did not have anesthesia consultations organized on the same day as the in-person surgical consultations; this could have reduced the differences in cost, but it requires additional organization at the institution.
Finally, the main limitation regarding the median time spent in the center is the modified cross-over design, in which the patient is his or her own control, with the surgical consultation as a control. By nature, the surgical consultation and the anesthetic consultation are not comparable. We did not compare, for example, the time spent in consultation with the surgeon with the time spent in TC with the anesthesiologist, but rather the total time spent in the hospital for the face-to-face consultation versus the total connection time for the remote consultation.
Nevertheless, many positive points can be drawn from this study. The quality of TC was achieved first of all through the presence of medicolegal criteria set up by the health authorities to ensure patient safety. Moreover, the global evaluation of anesthesia TC, from quality criteria to carbon impact and patient satisfaction, had never before been so exhaustively illustrated in the literature.
Our results could also be interesting for health systems where the preoperative assessment by an anesthesiologist is not an obligation. Because many day surgery cancellations are due to a lack of a medical preoperative evaluation, 11 –14 a simple and safe consultation as performed in telemedicine could be an answer to reduce disorganization. Telemedicine, representing a low cost for patients, a low carbon impact for the environment, and a decrease in time spent from home, that is, hospital journeys, seems to be an affordable alternative to optimize the preoperative pathway.
Conclusion
TC in anesthesia seems to be a good alternative in terms of file completion, patient satisfaction, and medicoeconomic gain for our patients. Through studies like this one, the development of TC in anesthesia, but more broadly the development of preoperative evaluation in anesthesia, can be enhanced. By facilitating access to preoperative evaluation for all, it could be adopted worldwide and thus reduce surgery-related morbidity and mortality in our patients.
However, further studies are needed to explore more extensively the clinical quality and the overall medicoeconomic gain for the health system.
Footnotes
Acknowledgments
The authors thank Dr. Griscenco and Susan Barke, native English speakers, for proofreading the article. We thank Drs. Raft, Classaux, Destruhaut, and N'Guyen for their assistance with the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Material Appendix SA1
Supplementary Material Appendix SA2
Supplementary Material Appendix SA3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.