
Abstract
Background:
Child and youth mental health problems represent a substantial burden of illness in Canada, with appropriate services only inconsistently available. Charitable organizations, such as Kids Help Phone (KHP), are, therefore, crucial to filling system gaps by offering 24/7 phone, chat, texting, and peer-to-peer services.
Methods:
We describe the services provided by KHP, the volume of use for each service, and compare usage across Canada's provinces and territories for a 5-year period from January 2018 to December 2022. Trends seen during the COVID-19 pandemic are highlighted.
Results:
More than 1.5 million total number of conversations were held across texting, chat, and phone services over 5 years. Considerable growth is demonstrated between 2018 and 2022, and many of the highest peaks in volume occurred in March or April of 2020, the onset of the COVID-19 pandemic. The highest proportional volumes were consistently from the northern territories.
Discussion:
KHP cannot provide specialized or repeat services, nor can it alone meet the scale of unmet youth mental health needs across the country. Nonetheless, KHP plays a pivotal role in the Canadian mental health system. Efforts to understand the role that KHP and other e-mental health services like it play within the national mental health landscape should be intensified to aid in understanding unmet needs, identify system gaps, and make needed enhancements.
Introduction
Youth mental health problems represent a substantial burden of illness, and are only now gaining commensurate recognition. In Canada, roughly 18.5% of adolescents aged 15–24 years are affected by mental health and/or substance use disorders, and 15.5% and 19.6% of males and females aged 15–30 years, respectively, report that they have seriously contemplated suicide in their lifetime. 1 In response to this, there has been considerable attention to transforming the youth mental health system; multiple initiatives have emerged across Canada to combat stigma and expand youth services. 2 –7
Despite these efforts, mental health support for youth is still not consistently available across Canada, and there remains a considerable amount of unmet need: 20% of young people in Ontario aged 4–17 years were classified as having a mental health need but only 3.5% were in contact with a children's mental health agency. 8
In an environment where traditional services are sparse and difficult to access, nonprofit and charitable organizations, which are not part of the formal care system, have become crucial to providing mental health support to children and youth across Canada. One such organization, Kids Help Phone (KHP), was established in 1989 as an independent telephone helpline. KHP originally focused on supporting young people experiencing abuse of any form. A priority of the organization was to provide young people with an avenue to accessing help on their own, anonymously, and without requiring involvement of a parent or guardian.
KHP's offerings have continued to evolve in response to needs and technological advancements with the goal of breaking down common barriers to help seeking, including fear, stigma, and lack of accessibility. 9 –11 Prioritizing the agency of children and youth in help seeking remains central to KHP's services; each encounter is designed to be confidential, child/youth friendly, and offers tools that young people can use in their day-to-day lives. KHP now supports roughly 4.8 million young people each year, making it Canada's largest professional counseling, support, and information service for youth.
Delineating the scope and scale of KHP, and the uptake of its services to date, provides an opportunity to better understand the mental health needs of young people in Canada and the role that KHP and similar e-health services play within Canada's mental health system. With this in mind, it is timely to describe the services provided by KHP, the volume of use for each service, and to compare their usage across Canada's provinces and territories. In Part 1 of this series, we focus on KHP's service volume data. Because data spanning the 5 years from 2018 to 2022 are presented, annual patterns and trends seen during the COVID-19 pandemic are also highlighted. A subsequent report (Part 2 13 ) will address issues most discussed over this same 5-year period.
Methods
SETTING AND SAMPLE
KHP has a national headquarters in Toronto, Ontario, with additional regional offices in Montréal, Quebec; Halifax, Nova Scotia; and Vancouver, British Columbia. All organizational data are stored in Canada. There is no exclusion criteria for accessing KHP's services, but they are designed and marketed for self-identified children and young people.
SERVICE PLATFORMS
KHP has four service platforms included in this analysis: texting, Live Chat, phone counseling, and a peer-to-peer platform. Live Chat has had fluctuating hours over the study period. In 2018, Live Chat was available during limited evening hours from 6 pm to 12 am; starting in March 2019, KHP expanded the service to 24 h. This continued until March 2020, when the organization temporarily closed the service for 1 year in response to increased service volumes due to the COVID-19 pandemic.
The Live Chat service reopened with reduced hours (6 pm–12 am) in April, 2021. Other than this, the phone and texting services operated on a 24-h basis throughout the 2018–2022 period, whereas the peer-to-peer service launched in June 2021. All services operate in English and French (with phone counseling in additional languages not included in these analyses) and data in this analysis are summarized from combined operations in both languages (i.e., not analyzed separately for each language).
DATA AND ANALYSES
The data used in the present analysis were independently collected as part of the organization's ongoing service monitoring efforts. In each of these services, KHP collects monitoring data on service volumes over time of day and day of week for each Canadian province or territory, as well as the issues identified during each service interaction and the age of the service user if volunteered during the conversation.
The volume of interactions is reported based on the total number of text conversations, Live Chat sessions, and phone conversations from January 2018 to December 2022, with the exception of August 2018. Owing to a technological data loss issue, data from August 2018 are incomplete for all of texting, Live Chat, and phone. This month was, therefore, omitted from analyses. The unit of analysis for each service is one completed session from start to finish with a service user (i.e., not individual text or Live Chat message received).
We additionally analyzed information on the total volume of page views and posts that occurred on the peer-to-peer platform between July 2021 and December 2022. Volumes are described both at the national and provincial levels over time. Summary descriptive statistics are provided for all four KHP service platforms (texting, calls, Live Chat sessions, and page views), per month from January 2018 to December 2022. Given that province and territory population sizes vary widely, standardized volumes (per 100 000 people) are reported for each platform.
ETHICS
Data were anonymized and aggregated into dashboards for the research team in KHP's centralized internal database ecosystem: Microsoft PowerBI. Only KHP staff members have access to this whole data set and no raw individual user data, clinical records, service user conversations, or KHP survey responses were provided or reported on. The research ethics board of the Douglas Research Centre reviewed the study protocol and deemed that no full review was required for this service evaluation project.
Results
CURRENT/CONTEMPORARY SERVICES
As of December 2022, anonymous and confidential single-session counseling and referrals are provided in English and French over the phone at any time and through online web-chat during evening hours. Phone counseling is also supported in Ukrainian, Russian, Pashto, Dari, Mandarin, Arabic, Plains Cree, and Ojibwe through an on-demand third-party translation service (note only data from English and French conversations are included in these analyses). Counseling sessions are provided through KHP's 135 professional counselors across Canada.
KHP runs a 24-h text messaging-based crisis response helpline through short messaging service. KHP offers this service in English and French with 1,440 active volunteers who are remotely trained and monitored by professional clinical staff through an independent centralized service delivery platform. Unlike phone-based counseling service, this text line is confidential but not anonymous because users access the service through their personal cell phones.
In 2021, KHP launched its Peer-to-Peer Community, the organization's first peer-to-peer service. This service was developed through a nation-wide codesign process with 237 young people in both English and French, with youth assisting in the development of the platform design, moderation procedures, conversation formats, and overall style of the service. This Peer-to-Peer Community takes the form of digital message boards moderated by youth peer workers on staff. Like the texting service, posting on the Peer-to-Peer Community is confidential but not anonymous given that young people need to provide e-mail addresses to create an account and post in forums. However, access to viewing message board content is openly available to anyone at any time without the need to create an account.
NATIONAL VOLUMES
Overall
From January 2018 to December 2022, the total number of discrete conversations, or “interactions,” across the three one-on-one service platforms (texting, Live Chat, and phone counseling) was 1,524,528 (Fig. 1). Monthly total volumes from 2022 are much higher than those recorded in 2018, demonstrating considerable growth across all services over this 5-year period. The largest growth across all platforms occurred over 2018–2019 when the texting service was first launched, amounting to a 264.66% increase in total service volume for 2019 compared with that for 2018 (Supplementary Table S1).
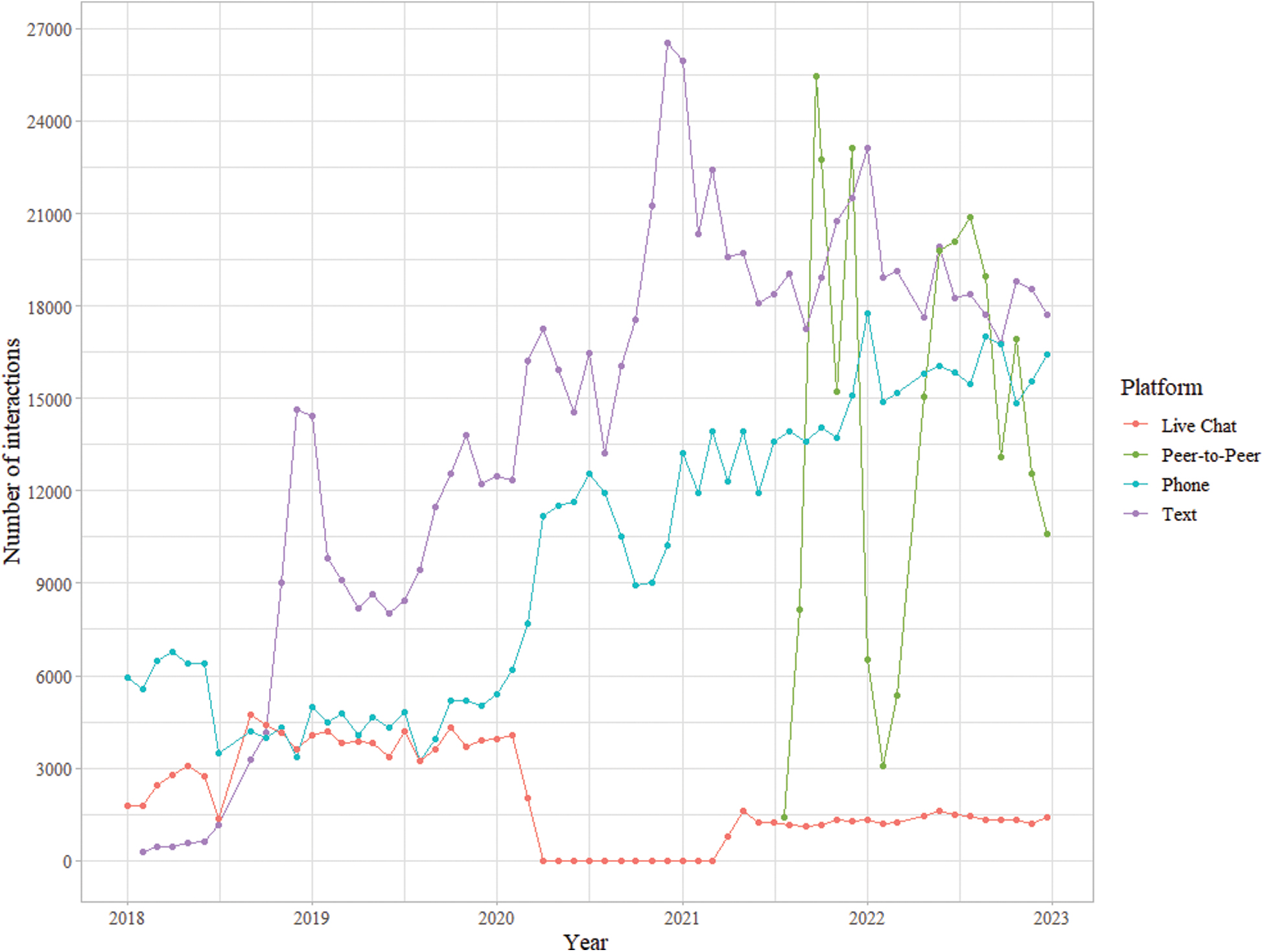
National-level volume of interactions by KHP platform. KHP, Kids Help Phone. Color images are available online.
Texting
Texting interactions totaled 827,474 from January 2018 to December 2022 and this was the most frequently used platform during this period. Use of the texting service peaked in December 2020 with 26,546 total interactions. Of all four services, texting also experienced the largest growth during this time period. After the initial growth during its first year of operation (i.e., throughout 2018), March 2020 (the onset of the COVID-19 pandemic) had the single highest one-month proportional increase in conversations, with a 31.19% increase from February to March 2020 (Supplementary Table S1).
Live Chat
Between January 2018 and December 2022, Live Chat sessions totaled 115,990, with a peak in usage in 2019 (45,988 sessions), when the service was offered 24 h per day. A substantial decrease in Live Chat usage was observed between March 2020 and March 2022 as a result of its closure and subsequent reduction in service hours once reopened in April 2021.
Phone counseling
A total of 581,064 phone counseling sessions occurred between January 2018 and December 2022. Peak usage of this service occurred in January 2022 with 17,762 total interactions during this month. The phone service demonstrated an increase in usage over time with the largest annual increase occurring from 2019 to 2020 (113.54%). The largest single-month increases in interactions were in January 2019, April 2020 (after the onset of the COVID-19 pandemic), and October 2019 with 48.30%, 44.89%, and 30.95%, respectively.
Peer-to-peer
The peer-to-peer service was publicly launched in July 2021 and was thus not included in the 2018–2022 overall growth summaries above. Total interactions for this service were substantially higher than other services, with 258,936 total page views in 18 months of operation. As of December 2022, there were 1,841 members on the platform, and an average of 101.55 posts created each month since July 2021 (Supplementary Table S2).
PROVINCIAL VOLUMES
Texting
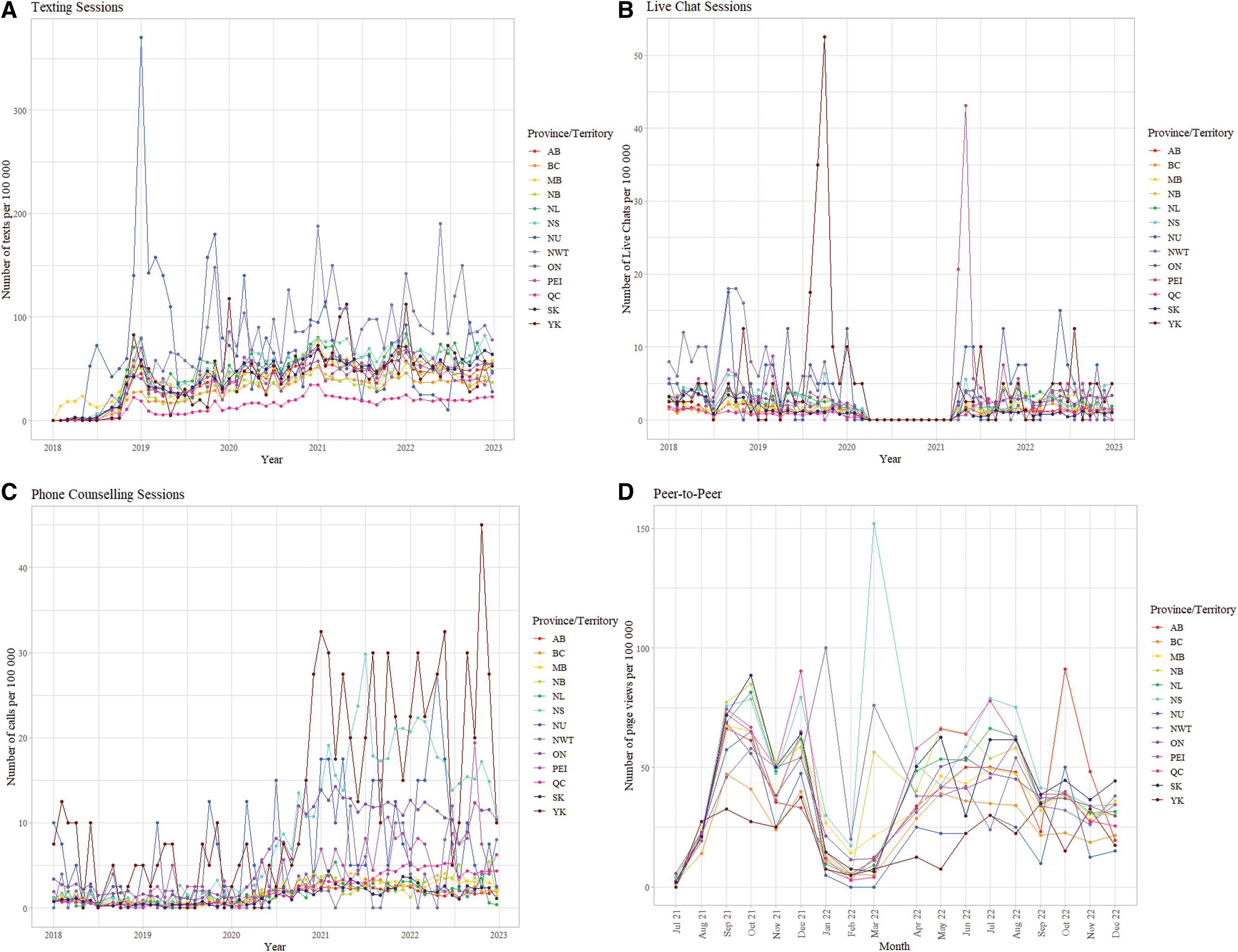
All provinces and territories demonstrated an upward trend in text service usage between January 2018 and December 2022 (Fig. 2a). The three northern territories in particular showed usage peaks in January of each year, with volumes ranging from 52.5 to 370 interactions per 100,000 people. The largest volume of texts per 100,000 people consistently came from the northern territories, with the highest peak from Nunavut in January 2019. The lowest proportional volume of text interactions came consistently from Quebec, ranging from 0.07 to 34.66 interactions per 100,000 people (Supplementary Table S3).
Live Chat
All provinces except Prince Edward Island showed consistent use of Live Chat between 2018 and 2022, ranging from 0.00 to 6.16 interactions per 100,000 people (Fig. 2b). PEI had a spike in usage with 43.13 interactions per 100,000 people in May 2021. The peaks were again in the northern territories, with the highest from the Yukon in October 2019 (52.50 per 100,000 people) (Supplementary Table S4).
Phone counseling
Phone counseling demonstrated the most within-province variability over time compared with other services, particularly in Yukon and Nova Scotia (Supplementary Table S5) (Fig. 2c). Nova Scotia initially had a low volume of interactions before 2019, with a lowest volume of 0.30 interactions per 100,000 people in July 2018, but showed a steady increase such that the province had the second highest volume in the country with 22.32 interactions per 100,000 people in February 2022.
Peer-to-peer
The highest proportional use was from Nova Scotia in March 2022 with 152.02 page views per 100,000 people (Fig. 2d). The second highest use was from the northwest territories showing 100-page views per 100,000 people in January 2022. Unlike the other platforms, Yukon was less engaged with the peer-to-peer service in comparison with other provinces and territories (Supplementary Table S6).
Discussion
Here we described the origin, evolution, and current KHP service platforms. Overall, most services saw a growth in interactions nationally between January 2018 and December 2022, with many of the largest increases occurring in January of each year. January volume increases are likely due to the presence of “Bell Lets Talk Day,” a national awareness campaign that promotes mental health help seeking. 2
It should be noted that during “Bell Lets Talk Day,” and for all other KHP promotions, the various KHP services were promoted together (i.e., with messaging stating that kids can call, text, chat, or connect through any of KHP's four platforms). An exception to this is the launch of new services: for example, in the year after the launch of the peer-to-peer service (2021), KHP ran additional peer-to-peer marketing efforts to promote this new service.
There were notable variations in trends between services at the national level. Both the text and phone service increased in usage over time, whereas the Live Chat and peer-to-peer services did not. For Live Chat, this was likely due to the service closure in 2020 and the reduced service hours after its reopening in 2021. Notably, before its closure, Live Chat received a higher volume of interactions than the phone service, suggesting that a 24/7, web-based service is desirable for Canadian children and youth.
For the peer-to-peer platform, we noted large fluctuations in the number of interactions in the 18 months that the service has been active. The highest volume of interactions for the service occurred in September 2021 and May–July 2022, all of which coincided with large marketing campaigns for this service. This suggests the effectiveness of such campaigns, and that with time and ongoing outreach, usage of the service may continue to grow. A further observation is that during its highest peaks, the volume of interactions in the peer-to-peer service was higher than any other service.
This high level of engagement may be because this platform is freely accessible to anyone without the need to personally share one's own experiences directly; for example, one can use the forums to view content that others with similar experiences may have previously shared. This suggests value in a service that maintains access to asynchronous support and validation in moments when individuals may not be interested nor ready to talk to a counselor or crisis responder directly.
In addition, variations in service use across provinces were observed. The northern territories represented the highest proportional volumes across each of the phone, Live Chat, and text services. This could be explained by a combination of factors including low availability of, or trust in, local formal services within northern territories, as well as higher than average substance use and suicidality in these regions. 14 In addition, other trends could be explained by outreach campaigns and/or KHP partnerships. For example, Nova Scotia had higher volumes than any other province in the Maritimes, particularly for phone and text services.
One potential reason for this is “Good2Talk,” a partnership between KHP and provincial organizations in Ontario and Nova Scotia, which markets the phone and text service to postsecondary students in those provinces specifically. 15 Conversely, we noted a consistently low uptake of both the texting and phone services in Quebec, despite providing French coverage in all KHP services. The low volume of texts and phone interactions in Quebec may be due to the presence and awareness of other French-specific youth mental health phone services available in the province. 16 –18
Finally, time trends related to the COVID-19 pandemic were observed. Many of the highest volumes occurred in March or April of 2020 when the pandemic began. Based on historical trends in KHP service provision, crisis-based spikes are common in KHP's services, but they do not often create “new normal” volumes for months and years into the future. It is, therefore, surprising that 2020 saw a high and sustained period of growth for some of KHP's platforms compared with previous years; notably, the phone service received a two- to threefold jump in volume during 2020, and this new volume was sustained through to December 2022.
Altogether, the persistently increased volume may signal a sustained need for longer term mental health supports as a result of the pandemic. This is likely due to the fact that the pandemic was not an isolated incident (e.g., a school shooting), but was instead a prolonged period of uncertainty and distress. Thus, there is potential for long-term negative impacts on the mental health and well-being of young people, particularly those who faced additional adversity and disadvantage. 19 This persistence in volume merits further consideration, as it may signal an ongoing increase in youth mental health problems that may emerge in other settings.
STRENGTHS AND LIMITATIONS
For the first time, we described historical variation in the utilization of KHP services, as well as variation in use of different technologies across Canada. Although we describe usage trends across provinces, we acknowledge that we are only capturing trends related to KHP service use (i.e., not necessarily representative of all youth distress across Canada). Furthermore, although we report proportional variations in interactions, some crude volumes represent relatively small absolute numbers (in some instances fewer than 10 interactions per month) compared with other Canadian provinces. Finally, although we can hypothesize that an increase in KHP services between 2020 and 2022 is associated with the COVID-19 pandemic, we cannot assume a causal relationship.
Conclusion
Given the individual and system level barriers that can limit help seeking and thus result in unmet mental health needs, many youth rely on e-mental health and crisis services for support. KHP plays a pivotal role in the Canadian mental health landscape: its ease of access from any point in the country, through any technological means, facilitates wide engagement across most provinces and territories. Nonetheless, as these services are often time limited and offered through single session, they do not have the capacity to provide more intensive care to young people when required—especially for those who have complex or severe needs.
Thus, more services to complement e-mental health solutions and support the ongoing recovery of the young people who contact them are crucial. Efforts to understand the role that KHP and other services like it play within the national mental health landscape (e.g., as part of stepped care models) should be intensified to enable other service providers and system leaders to understand needs, identify gaps, and build functional access points between e-mental health services and the full breadth of needed supports.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.