
Abstract
Background:
Telemedicine has proven successful in relieving the burden of chronic neurological disorders from the national health care systems by ensuring a highly customized and effective management plan. Although many studies focus on assessing telemedicine effectiveness, little is known about the economic implications of telemedicine applications in chronic neurological diseases (CNDs). This issue could account for a lack of widespread implementation.
Objective:
Our study attempted to fill this gap by systematically reviewing scientific literature on the economic evaluation of telemedicine compared with traditional care in the management of CNDs.
Methods:
We performed a literature search on PubMed, Google Scholar, Scopus, Embase, and Medline. The inclusion criteria were as follows: (1) studies with a full cost-analysis; (2) randomized controlled trials; (3) studies comparing telemedicine interventions with traditional care; (4) articles focusing only on CNDs. Conversely, the exclusion criteria were as follows: (1) studies focusing on acute neurological conditions or other diseases and (2) study protocols, case report, duplicate articles, abstract only, books, letters to editors, and review articles.
Results:
Ten articles met the inclusion criteria. Three different approaches of telemedicine intervention could be identified: digital cognitive-behavioral therapy (CBT), motor telerehabilitation, and home monitoring and assessment devices.
Conclusion:
Cost-analysis showed an overall benefit in terms of both cost and effectiveness from the application of telemedicine instead of in-presence management in CNDs. Among the identified interventions, digital CBT proved to be the most cost-saving. However, promising results were also found in monitoring and assessment devices and in telerehabilitation. Definitely, however, more thorough, comprehensive, and high-quality economic evaluation studies are needed.
Introduction
The burden of chronic neurological diseases (CNDs) has dramatically increased over the last 25 years. 1 Nowadays, CNDs are one of the leading causes of permanent disability worldwide, contributing in 2016 to 11.6% of global disabilities-adjusted life-years (DALYs), and with the progressive aging of the population, the prevalence of these disorders will keep increasing. 1 Providing constant care for people with CNDs is very challenging as patients often require a multidisciplinary approach necessitating a considerable increase in resources allocated for their management. Consequently, this has led to an additional strain on the national health care systems that are currently already bending over due to the COVID-19 pandemic. Telemedicine has proven to be effective in the management of chronic diseases and has the enormous potential to improve patient's and caregivers' quality of life as well as to ease the burden on the health care system. 2 –5
Despite such reported benefits, the adoption and implementation of telemedicine solutions require incurring a whole bunch of costs, including the cost of devices and equipment, the cost of supporting servers, and the cost of information technology technicians and other staff involved in the projects. Therefore, there is a need to investigate the real impact of the implementation of telemedicine in the health care system. To perform a proper comparative economic evaluation of the different possibilities of health care application of telemedicine, a thorough analysis of the differences in the cost and effect of these interventions is required. Five different methods are commonly used: cost–effectiveness analyses (CEAs), cost–utility analyses (CUAs), cost–consequence analysis (CCA), cost–minimization analyses (CMA), and cost–benefit analyses (CBAs). 6
Finally, it is essential to consider the point of view from which the analysis is conducted, which is better defined as the “perspective,” since it determines which costs are relevant and consequently influences the interpretation of the results. Perspectives typically used in cost analysis are those of the patient, hospital/clinic, health system, or society. 6 To this end, we performed a systematic review of the literature on the economic evaluations of telemedicine versus traditional approach in CNDs.
Methods and Materials
STUDY SELECTION
Our systematic review was drafted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). 7 A systematic search of the scientific literature on PubMed, Google Scholar, Scopus, Embase, and Medline was performed to identify studies published to date reporting the cost–effectiveness (“the degree to which something is effective or productive in relation to its cost”) 8 of telemedicine interventions applied to CNDs.
Only English-language articles were considered. To this aim, we used the following terms, and their possible combination: ([cost benefit analysis OR cost effectiveness analysis OR cost utility analysis OR cost minimization analysis OR incremental cost effectiveness ratio (ICER) OR quality of life year OR quality of life] AND [telemedicine OR telehealth OR telerehabilitation OR exergames OR virtual reality OR digital health OR mHealth OR mobile OR telephone OR telemonitoring OR remote monitoring OR video OR serious game OR artificial intelligence OR exergames] AND Neurology). Moreover, relevant articles were manually located individually to examine references and cited-by articles.
Only the following studies were included: (1) studies with a full economic evaluation such as CEAs, CUAs, CCA, CMA, and CBAs; (2) randomized controlled trials (RCTs) 9 ; (3) studies comparing telemedicine interventions with traditional care; and (4) articles focusing only on CNDs. Whereas the following exclusion criteria were applied: (1) studies focusing on acute neurological conditions or other diseases and (2) study protocols, case report, duplicate articles, abstract only, books, letters to editors, and review articles.
In this review, we refer to telemedicine as “the use of electronic information and communication technology to provide and support healthcare when distance separates participants.” 10 ; This broad definition includes the use of several digital devices for monitoring, management, and rehabilitation and describes the main techniques involved, including gaming techniques, virtual reality, mobile and computer application, artificial intelligence, software, and home-based exercises.
DATA EXTRACTION AND QUALITY ASSESSMENT
After title screening, two expert investigators (E.M. and L.L.) independently examined abstracts to select articles that met the abovementioned inclusion and exclusion criteria for full-text screening. Data were extracted into a standardized excel template including the following information: author's name, country and year of publication, neurological disease, population size and mean age, type of telemedicine intervention, time horizon, currency and currency year reference, performed analysis, and, finally, the adopted perspective.
A 10-item checklist by Drummond et al. was used to appraise the methodological rigor of the economic evaluation of each article. 6 This checklist was selected as it is commonly recommended by international guidelines and considers the following: (1) research question; (2) description of the intervention; (3) study design; (4–6) identification, measurement, and valuation of relevant costs and consequences; (7) whether discounting was performed or not; (8) incremental analysis; (9) whether uncertainty and sensitivity analyses were carried out; and (10) discussion and generalization of results. 6
Whenever possible, we also adjusted the values with the 2022 inflation rate to reflect current cost. Moreover, we explored whether sensitivity analysis was performed in any of the included studies since it is critical for identifying variables that might change the study's conclusions.
Results
The search on the different databases and manual screening retrieved 1,519 results; after removing 250 duplicates, a meticulous title and abstract screening was performed. We then selected 42 articles for full-text assessment, but only 10 articles were eligible according to the inclusion criteria and were therefore included in the review. 11 –20 The PRISMA flowchart, illustrated in Figure 1, shows each phase of study selection.
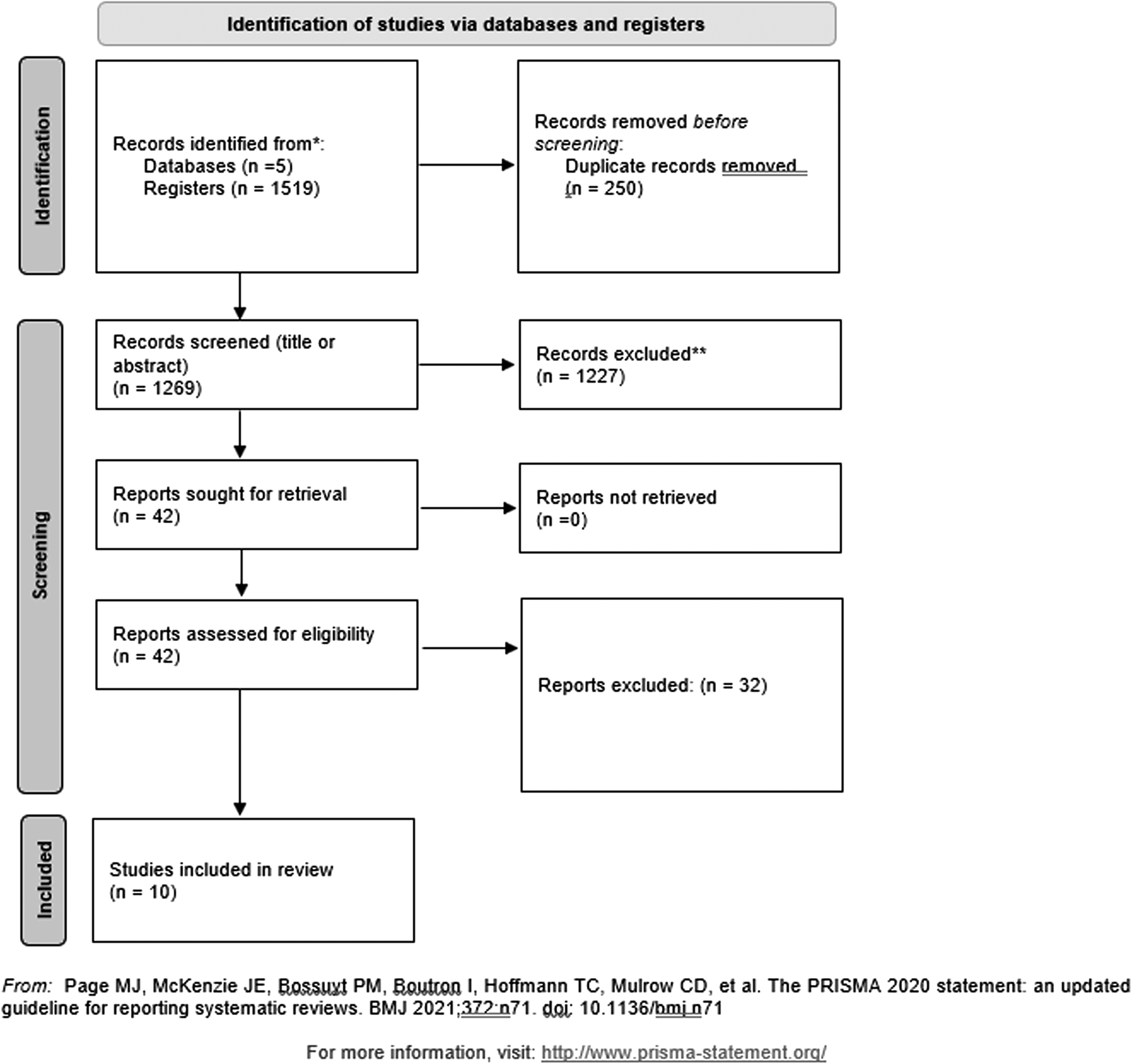
PRISMA flowchart showing each phase of the selection process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Out of these studies, four focused on sleep disorders, 12,13,16,17 one on multiple sclerosis (MS), 18 one on cognitive impairment, 19 one on Parkinson's disease (PD), 15 one on cerebral palsy, 14 and two on stroke. 11,20 Notably, since our review concentrates on CNDs, we had to exclude several studies centered on stroke acute management, while we still included studies dealing with long-term management of complications.
Three different approaches of telemedicine intervention could be identified: the four studies on sleep disorders used remotely delivered cognitive behavioral therapy 12,13,16,17 ; an additional four studies compared motor telerehabilitation with conventional care 11,14,18,20 ; finally, the last two studies used home monitoring and assessment devices. 16,19
All of the studies were conducted between 2012 and 2020, in high-income countries, including Spain (n = 2), 15,20 The Netherlands (n = 2), 12,17 the United Kingdom (n = 2), 11,18 Germany (n = 1), 13 the United States (n = 1), 16 Sweden (n = 1), 19 and Australia (n = 1). 14 Economic analyses of each study were reported using the local currency between 2013 and 2019.
The time horizon ranged from 12 weeks to 1 year, 6 months being the most common period to perform the intervention protocol. Three of the studies reported a societal perspective (30%), 12,16,17 a further three a health care perspective (30%), 14,15,19 and three included both societal and health care perspectives (30%) 11,13,18 ; conversely, only one reported no relevant viewpoint (10%). 20
Concerning the different economic evaluation modalities, six studies reported exclusively CEA (60%), 11,14,15,17 –19 three performed both CEA and CUA (30%), 12,13,16 and lastly, only one used the CBA methodology (10%). 20
To better understand and interpret the results, we grouped the studies included in the review according to the adopted telemedicine approach and therefore discuss the main findings below. In Table 1 and in Table 2, we provide a summary of the main characteristics of the studies.
Summary of Study Characteristics
AMPS, Assessment of Motor and Process Skills; COPM, Canadian Occupational Performance Measure; ISI, Insomnia Severity Index; M, mean; MS, multiple sclerosis; PD, Parkinson's disease; SD, standard deviation; UPDRS, Unified Parkinson's Disease Rating Scale.
Characteristics of the Studies Included in the Review
AUD, Australian dollar; CBA, cost–benefit analysis; CBT, cognitive–behavioral therapy; CEA, cost–effectiveness analysis; CUA, cost–utility analysis; EUR, Euros; GBP, British pound sterling; NS, not stated; SEK, Swedish krona; USD, U.S. dollar.
We used the 10-item Drummond checklist 6 on the selected studies for quality assessment: all studies scored “Good” except one that ranked “Average; see Table 3, at the end of the section, for the results.
Quality Assessment of Economic Evaluations Using the Drummond Checklist (Poor: 1–3 Points; Average: 4–7 Points; Good: 8–10 Points)
TELEREHABILITATION
Four studies evaluated the economic impact of motor telerehabilitation in the context of different CNDs such as MS, cerebral palsy, and long-term consequences of stroke. 11,14,18,20
A study conducted on children with cerebral palsy used “Move It To Improve It (Mitii)” training, an effective, individualized web-based exercise program for upper limb motor rehabilitation. 14 One hundred two children with mild-to-moderate congenital hemiplegia were randomized into two groups, and each participant performed the exercise program for 20 consecutive weeks. The intervention group recorded a significantly higher number of responders in the two outcome measures used, which were the Assessment of Motor and Process Skills (AMPS) (p < 0.001) and the Canadian Occupational Performance Measure (COPM) (p = 0.002).
Furthermore, most of the responders in the intervention group (about 70%) had shown an improvement in both scales. Health costs were $476 for the control group and $1,861 for the intervention; in the latter the largest burden was Mitii license as well as training and staff costs. The ICER ranged from $3,078 to $4,191, according to the effectiveness measures applied, respectively, AMPS or COPM. To achieve a clinically meaningful improvement in the AMPS and COPM scales per patient would cost $2,800 and $4,000, respectively.
For people with severe progressive MS (with an Expanded Disability Status Scale—EDSS—between 6.5 and 8), a RCT attempted to compare a home-based telerehabilitation approach with conventional rehabilitation treatment. 18 One hundred forty participants were randomly assigned to the intervention or the control group, and the study lasted for a total of 36 weeks. Despite the slightly higher cost of the intervention group (£3,667.30 vs. £3,491.91), there was an improvement in EUROQOL-5D-5L values from baseline to 36 weeks of 0.042 for the intervention group and 0.01 for the usual care group. Nevertheless, the difference with the control group did not reach the minimum significant difference established by Marra et al. 21 Overall Quality-Adjusted Life Year (QALY)-ICER was ∼£14,700. Moreover, telerehabilitation intervention resulted more effective to improve motor function, measured with the Amended Motor Club Assessment score, compared with standard care (p = 0.0014).
Also, statistically significant differences were observed, at the end of the study at 36 weeks, in hip and ankle goniometry (respectively p = 0.012 and p = 0.015).
Concerning motor complications poststroke, the study conducted by Lloréns et al. evaluated the administration of a virtual reality-based telerehabilitation program for balance recovery. 20 The virtual reality system relied on a “serious game,” defined as games that “have an explicit and carefully thought-out educational purpose and are not intended to be played primarily for amusement.” 22 The aim was to step on some lifting objects with the closest foot, while keeping the other foot within the boundaries of a circle drawn on the floor. In CBA, significantly lower costs were reported for the virtual reality intervention group compared with traditional in-clinic rehabilitation ($835.61 vs. $1,490.23). However, no significant differences in clinical outcomes were found; improvements in gait and balance were registered in both scenarios.
A second study, also focusing on poststroke complications, investigated the possible use of the Nintendo Wii console for upper limb motor function rehabilitation in stroke patients. 11 Here instead, the study used an exergame, portmanteau word between “ exercise” and “game,” denoting the combination of motor and cognitive training through commercial video games. 23 A total of 235 participants, presenting with ischemic or hemorrhagic stroke within the last 6 months, were enrolled in the trial and subsequently randomized. Results showed no differences in either primary outcomes or QALYs at 6 months between the intervention and the control groups (interquartile range: 0.212–0.320 vs. 0.238–0.313), against, however, higher costs of telerehabilitation (£1,106 vs. £730).
MONITORING AND ASSESSING DEVICES
Two articles compared digital tools for remote assessment and management of neurological symptoms with traditional in-clinic visit. 15,19
The study by Cubo et al. compared the cost-effectiveness of a home-based motor monitoring (HBMM) with traditional clinical assessment (OBM) over the course of 1 year in patients with advanced idiopathic PD, defined by the Unified Parkinson's Disease Rating Scale (UPDRS) score >4. 15 Forty patients were randomized into the control group or the intervention group that used a home-device called “Kinesia system” comprising a tablet app, a wireless motion sensor worn on the finger, and a symptom reporting device. Total medical and nonmedical costs were relatively higher in the HBMM group compared with the OBM group (€14,567.3 vs. €12,069.8), although not significantly (p = 0.24).
The HBMM group was found to be cost-effective in terms of functional status, motor impairment, and motor complications (UPDRS II/III/IV-ICERs) but not in terms of QALYs and mental status (QALY-ICERs and UPDRS I-ICERs). Overall, in HBMM group, the UPDRS-ICERs ranged from €126.72 to €701.31 (the required cost to decrease one unit in the UPDRS parts II, III, IV, and total UPDRS).
SMART4MD application was specifically developed for remote monitoring and cognitive telerehabilitation in patients with mild-to-moderate dementia. 19 Some major functions involved reminding patients of health information such as medication intake or doctor's appointments, stimulating cognitive functions through games or practical exercises, or being able to share those data with the caregiver as well. There were no significant differences in total costs between the two groups (€8,188 vs. €8,175); however, a greater loss in terms of QALYs was observed in the intervention group (−0.03 vs. −0.01; p = 0.1759), whereas measures of Quality of Life in Alzheimer's Disease (QoL-AD) (−0.76 vs. −1.27; p = 0.2027) and Mini-Mental State Examination (MMSE) (1.06 vs. 0.60; p = 0.0331) were found to be improved in comparison with the control group.
An additional strength of the study was the inclusion of caregivers, who share the burden of disease with their loved ones, for whom the SMART4MD application proved to be less costly and more effective in terms of gaining QALYs.
DIGITAL COGNITIVE-BEHAVIORAL THERAPY
Within the area of CNDs, a considerable amount of attention has been directed toward sleep disorders and their remote management. Indeed, insomnia has a significant correlation with an extensive economic burden, as affected individuals have major functional impairments. Costs arise primarily from lost productivity as well as higher rates of absenteeism, while also resulting from increased utilization of health care services. Accordingly, four studies 12,13,16,17 investigated the economic feasibility of remote cognitive-behavioral therapy (iCBT) compared with traditional face-to-face therapy in moderate-severe insomnia, as meta-analytic evidence has largely demonstrated its effectiveness. 24
An RCT conducted on subjects with severe insomnia, defined by an Insomnia Severity Index (ISI) >14, sought to perform an economic evaluation of iCBT both from a societal perspective and a public health care perspective. 13 The results revealed that, from a societal perspective, iCBT intervention appeared to be more effective than conventional therapy (27/64 subjects in the intervention group achieved a symptom-free status, vs. only 4/64 in the control group) and that such improvements were achieved at a lower cost (€4,030 vs. €5,021). Moreover, CUA performed by computing QALYs through the Short-Form Six-Dimension scale yielded a similar result. From a public health care perspective, benefits were attained at a higher cost; ICERs amounted to €650 and €11,285, respectively, for one symptom-free patient and QALY earned.
Similarly, in a separate study, iCBT was delivered by the “i-Sleep” intervention, consisting of five modules with several different topics concerning sleep hygiene, psychoeducation, restriction of time in bed, relaxation exercises, and handling dysfunctional cognitive beliefs about sleep. ISI score was significantly improved compared with the control group with a mean difference of 3.9 points. 12 However, the mean difference in QALYs calculated with EUROQOL-5D-5L questionnaire at 26 weeks was statistically nonsignificant (0.40 vs. 0.38). Total health care and societal costs between the two groups were not statistically different, but average societal costs in the iCBT group were lower than in ordinary care. ICER for ISI score at the end of the study was −81, implying that 1 point of improvement equaled a cost saving of €81 for iCBT over conventional treatment. Finally, for QALYs, the ICER was −28,056.
The study conducted by DeBruin et al. also compared iCBT with face-to-face traditional group therapy in 62 adolescents with insomnia. iCBT at 1-year follow-up had considerably lower societal and health care cost than the usual care (societal cost: €1,046.53 vs. €1,452.08, p = 0.006; health care cost: €689.23 vs. €836.06, p < 0.001) and thereby had a high probability of being cost-effective. 17 CEA showed that with a willingness to pay €0, the probability of iCBT to be cost effective is 95% for both sleep efficiency ≥85% and QALYs.
Lastly, a further study applied a Markov simulation model to compare five groups for the treatment of severe insomnia, such as computer-assisted cognitive behavioral therapy, individual or group conventional cognitive behavioral therapy, pharmacotherapy, and no insomnia treatment. 16 A Markov model is a widely used analytical framework for economic evaluations that depicts the progression of a system over time through various states, in which precise transition rules apply. From this simulation, iCBT has proven to be the preferred intervention economically compared with control groups followed by group CBT, pharmacotherapy, and individual CBT (respectively, $2,998.8 for iCBT; $3,035.93 for group CBT; $3,102.17 for pharmacotherapy; and $3,756.79 for individual CBT). Moreover, iCBT had the smallest ICER and is therefore the most cost-effective treatment compared with no treatment (−3,124.73).
Discussion
Telemedicine and its declinations are becoming increasingly popular worldwide. In several diseases, remote management has proven to be efficient in ensuring a high and personalized standard of care. 2 –5 Meanwhile, however, very few studies highlighting the financial implications of telemedicine are currently available within the chronic management of neurological diseases. Only a recent systematic review has attempted to collect all studies focusing exclusively on telerehabilitation in neurological diseases, but the authors retrieved only three eligible articles on stroke. 25 Two of the articles 20,26 revealed actual cost savings from the telemedicine approach, 27 while the last one found no significant differences between telerehabilitation and traditional care. Furthermore, only one of the studies was an RCT, 20 one had a retrospective design, 27 while the last was a single-group intervention. 26
As the burden of CNDs has significantly increased in recent years, with greater incidence and disability, 1 we have steered our review toward the remote management of all the aspects of telemedicine approaches (monitoring, management, rehabilitation gamification, virtual reality, mobile and computer application, artificial intelligence, software, and home-based exercises) in CNDs. In addition, to provide more reliable results, we exclusively reviewed RCTs comparing telemedicine with standard in-clinic care. 9
Among the different interventions, the one that proved most cost-effective was remote CBT. 12,13,16,17 The four studies assessing iCBT reported lower costs combined with a greater improvement in outcomes such as ISI, subjective sleep efficiency, and quality of life. On top of that, Darden et al. 16 not only compared iCBT with care-as-usual—individual or group face-to-face therapy—but also with pharmacological interventions and with no treatment, affirming the superiority of remote CBT over all the other approaches.
Remarkable findings have also occurred in the use of mobile phone apps for assessment and management of CNDs. 16,19 Results showed nonsignificantly higher costs of telemedicine, but a significant improvement in outcomes such as UPDRS II/III/IV, QoL-AD, and MMSE. However, similar results were not reported in terms of QALYs. A peculiarity of the study by Ghani et al. is that it additionally included caregivers, showing that SMART4D app brought more benefits, both in terms of burden relief and QALY, to the latter than to their loved ones with dementia. 19
Conversely, within the scope of telerehabilitation, uncertain results were observed. 11,14,18,20 Three articles reported higher costs for the intervention groups, 11,14,18 while in two articles, although there were great improvements in outcomes, no significant differences were shown between the two groups. 11,20 The most important costs to be addressed are mainly related to the purchase and installation of the instruments and for the staff needed to train patients on their use. However, according to the authors, these costs should be considered minimal compared with the improvements achieved, leading to more autonomy in everyday life activities. 14 Noteworthy is the brief duration of these intervention, perhaps too short for significant differences to be recorded. Besides, Freeman et al. conclude that a bias may have occurred due to the enrollment of mainly young patients with high residual function, who therefore experienced less marked improvements than the more impaired patients. 18
The results summarized in the section above showed an overall cost-effectiveness from the application of telemedicine instead of traditional and in-presence management. This saving involves especially those interventions that do not require any special digital and technical instrumentation to be purchased and installed.
However, to demonstrate how actually the application of telemedicine approaches will economize in the long run, we believe that there is a need for more studies with a broader time horizon, specifically designed to ascertain and evaluate the economic implications of telemedicine. Indeed, although telemedicine requires significant start-up costs, these interventions could potentially provide significant cost savings over the long run. In rural populations and low- or middle-income countries, this cost-effectiveness could be particularly valuable in terms of gains in quality of life and DALYs. 28
Thus, the results of our review lead us to support the idea that cost savings through telemedicine must be considered from multiple perspectives. 29 It is essential to weigh not only the expenses sustained by the health care system that supports disease management, but also the well-being of the patients, how much more protected they feel by a constant and noninvasive monitoring, how much it improves the overall quality of life and their performance at a relational and work level, and much more.
This review has several limitations. First, the low amount of available studies with both a comprehensive economic evaluation and a comparison of telemedicine with traditional care. This has led to a medium heterogeneity in the characteristics of the studies included in this review, which has nevertheless allowed us to broaden our research to multiple fields. Furthermore, all of the studies were conducted in high-income countries, and therefore, it is not possible to generalize the current results to low- and middle-income countries. This has major implications as it becomes more difficult to convince stakeholders to invest in telemedicine to support low-, middle-income, and rural populations. In addition, it is possible that we excluded studies from such countries, published in the original language, as we considered only articles written in English.
Another limitation is the short duration of the interventions, ranging from 12 weeks to 1 year, which therefore may complicate the demonstration that the benefits of telemedicine can offset its costs. Finally, a different issue concerns the absence of true standardized guidelines involving the duration and intensity of training and the types of exergames to be used in telerehabilitation or the frequency at which subjects should be monitored at home.
Regardless, telemedicine could be the answer to many of the unmet needs of patients with CNDs and their caregivers, who are bearing a heavy burden. Although plenty of trials now attest to their efficacy in terms of outcomes, and new techniques are being developed, 30 nevertheless, whether telemedicine can be cost-effective or not is still unclear, and this is definitely holding back its widespread adoption. Although we are aware that more studies are needed, especially from low- or middle-income countries, we hope to have highlighted the economic potential of telemedicine and all its declinations.
Conclusion
As telemedicine is becoming an emerging and increasingly prominent tool, more and more studies are focusing on the possibility of using this approach as an alternative to traditional care. Such methods are globally well accepted as they focus on the patient, ensuring constant care and a highly personalized treatment program. Our study identified that evidence to date suggests that telemedicine could be cost-effective in the support for traditional care in several CNDs. Still, more in-depth, wide-ranging, and high-quality economic evaluation studies need to be promoted urgently to prove cost-effectiveness and health-related quality of life of telemedicine.
Author's Contributions
Conception and design of the review: E.M. Material preparation: E.M. The first draft of the article was written by E.M., L.L., and S.B. and all authors commented on previous versions of the article. All authors read and approved the final version to be published. All authors agree to be accountable for all aspects of the work. L.L. is the guarantor.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.