
Abstract
Introduction:
Electromyography (EMG) assessments have been conducted virtually more frequently in recent years, leading researchers to explore the barriers to EMG assessments in a telehealth setting and how to overcome them.
Methods:
A scoping review was conducted according to the methodology described by Arksey and O'Malley. A comprehensive search using controlled vocabulary and keywords for two concepts, EMG and telehealth, was conducted using Medline and EMBASE on February 7, 2022. Two independent reviewers screened titles, abstracts, and full-text articles. Two reviewers also extracted the data and described the findings in a descriptive analysis.
Results:
A total of 248 articles were screened during the abstract and title review, of which 64 full texts were screened for eligibility. Of these, 15 publications met the inclusion criteria. Most articles were published in 2018 or later (66.7%). The most frequently mentioned barrier to conducting a virtual EMG assessment was poor data and signal transmission (53.3%). Another frequently mentioned barrier was poor patient usability (33.3%). Solutions most frequently reported related to patient usability (33.3%). These included interactive instructions and video chat to monitor and provide the patient with technical support.
Conclusion:
The last 4 years have seen an increase in articles published on EMGs' use in telehealth to monitor or diagnose patients. Further research is required to determine if the proposed solutions have improved clinical outcomes for the patient.
Introduction
Electromyography (EMG), which has been introduced into routine clinical practice since the 1950s, is a useful method of physiological monitoring of muscle activity. 1 It is an important diagnostic and monitoring tool in health care due to its crucial role in many biomedical and clinical applications. These applications include but are not limited to medical research, rehabilitation, and biomechanics. 2 There are several clinical assessments that utilize EMG. For example, EMG is useful in clinical practice as it is used to diagnose muscle and nerve disorders such as peripheral neuropathy and carpal tunnel syndrome. 3
EMG has traditionally been used for in-person clinical assessments. Recently, there has been an increased need and demand for virtual health care, in part, brought on by COVID-19 and also because of recognized inequities in access to care for patients in rural and remote settings. Telemedicine allows the delivery of care through internet-based services, and in the last few years, EMG assessments have begun to be conducted virtually. 4 When used appropriately, telehealth has the potential to save health care dollars while simultaneously saving travel time and out-of-pocket costs for patients. 5 While telehealth has provided many advantages in the health care field, the use of EMG in telemedicine is recent and has been shown to have some constraints and limited use in practice. 6
The barriers to using EMG virtually and recommendations for overcoming these have been reported in the literature; however, to the best of our knowledge, a scoping review is yet to be conducted to assess and summarize these barriers.
This scoping review aims to determine if there are any clinical or technical barriers to conducting EMG assessments virtually and how they are used in a virtual health context. In addition, this review summarizes solutions that have been recommended to address barriers to using EMG as part of a virtual care assessment.
The population of interest for this scoping review includes all patients who underwent virtual EMG assessments.
Methods
This scoping review used the methodology guided by Arksey and O'Malley. 6 However, in this case, only two databases were searched. This article adheres to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) for scoping reviews. 7
SEARCH STRATEGY
The search was conducted on February 7, 2022. Two electronic databases were used: Medline (1946-present through Ovid) and EMBASE (1946-present through Ovid). The search strategy used controlled vocabulary and free text terms to highlight the following concepts and objectives mentioned in the research question: (1) electromyography and (2) telehealth. Telehealth includes any general term for remote health (e.g., telerehab, telemedicine, m-health). Studies were limited to English, and news articles, editorials, and veterinary studies were removed from the results. The Medline search strategy can be found in the Supplementary Materials. All sources were checked to be peer-reviewed to maintain the accuracy of the results.
INCLUSION AND EXCLUSION CRITERIA
Articles were included if they discussed the use of EMG assessments in telehealth or conducted remotely. This included but was not limited to wearable EMG devices and EMG virtual health applications (i.e., migraine, dysphagia, stroke, spinal cord injuries, and pain monitoring). Articles were only included if authors or investigators discussed the limitations of EMG assessments and/or how to overcome the barriers of conducting EMG assessments virtually. This included but was not limited to the transmission of the data virtually, the quality of the signal, the usability of the device, data storage, safety and patient confidentiality, and user-friendliness. The included article types were scientific peer-reviewed articles obtained from the electronic database search.
All articles published during or after 2006 were included due to the rapid advancement of technology and the limited knowledge of telehealth and EMG assessments before 2006. Article settings that were included had to consider a virtual or remote setting during EMG assessments. Article interventions had to consider an EMG application that was used to assess or monitor a patient remotely. Article outcomes had to consider barriers or how to overcome barriers of remote EMG. Finally, articles had to consider a population that needed to use EMG to measure any sort of muscle activity due to neuromuscular disorders.
Articles were excluded if they were not written in the English language due to feasibility. Articles were also excluded if they only included clinical EMG applications that did not consider their applications in a virtual setting. Books, newspaper articles, theses, dissertations, and conference abstracts were also excluded due to feasibility. Finally, articles were excluded if they only described applications of EMG use virtually without considering any barriers to these assessments and/or how to overcome certain barriers to the data collection method.
STUDY/SOURCE OF EVIDENCE SELECTION
All citations were uploaded into Covidence®, and duplicates were removed. 8 Title and abstracts were screened and assessed by two independent reviewers against the inclusion and exclusion criteria. Next, two independent reviewers ordered full-text publications of all relevant titles and abstracts and screened against the inclusion and exclusion criteria. Finally, the reasons for excluding specific sources during the full-text that did not meet the inclusion and exclusion criteria were recorded. If any disagreements occurred between the reviewers during any stage of the selection process, these disagreements were resolved through a discussion-based meeting.
DATA EXTRACTION
One reviewer determined which variables would be extracted and created a data extraction form before the literature review. The data extraction process was done using Covidence by two independent reviewers who used the same form. Any disagreements that occurred between reviewers were resolved through a discussion-based meeting. Extracted data included general article information and characteristics (year of publication, the country where the study was conducted, the purpose of the study, and the setting). It also included key findings related to the clinical and technical barriers of EMG used virtually and how these were overcome. The key findings also included restrictions to the scope of professional practice that could affect virtual EMG assessments.
Results were synthesized by grouping the articles according to the types of barriers they presented and the proposed solutions for these barriers (if any). These were then each summarized. Finally, details for the evidence obtained in this review were presented through tables and graphs and a narrative summary.
Results
A total of 249 articles were imported into Covidence for screening in the initial search, with 1 duplicate removed. A total of 248 articles were screened for the title and abstract review. After the title and abstract screening, 184 articles were excluded, and 64 articles were obtained for a full-text review screening. Then, 49 articles were excluded based on the full-text screening because the study design (9 publications), setting (4 publications), population (1 publication), interventions (16 publications), or outcomes (18 publications) were not relevant to the scoping review. One publication was excluded because it had not been peer-reviewed. A total of 15 articles were deemed relevant and included in the scoping review (Fig. 1). 7

Number of published articles per year in the included texts.
ARTICLE CHARACTERISTICS
A total of 15 articles were identified. The number of articles published concerning EMG and its virtual application and assessment has significantly increased over time, with a significant upward trend starting between the years 2018 and 2022 (Fig. 2).
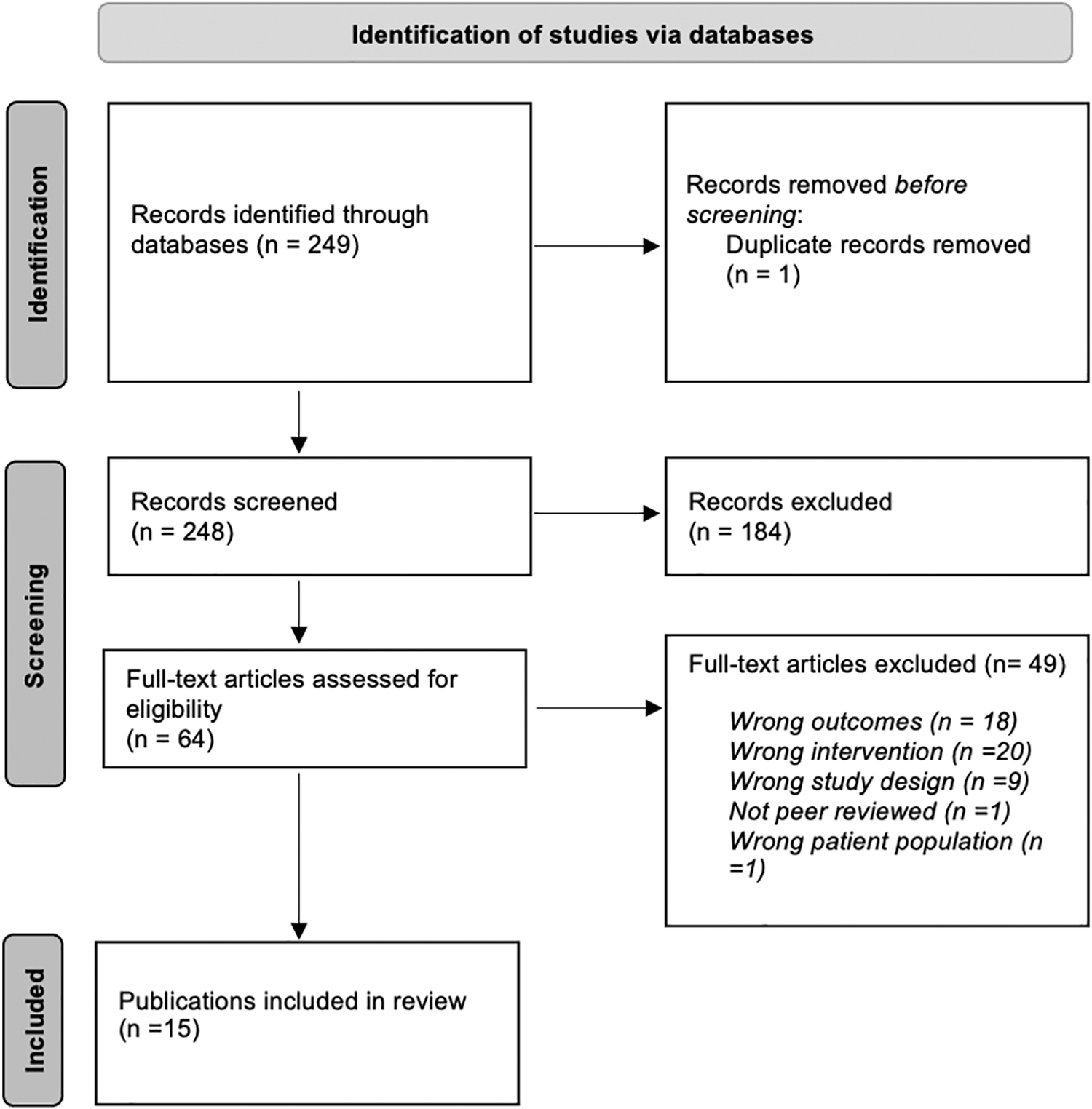
Preferred Reporting System for Systematic Reviews and Meta-Analyses diagram of the screening process.
The articles in the included texts were conducted in 11 different countries, most in the United States and Italy (20.0% each). The countries in which the articles were conducted are found in Table 1.
Country in Which the Study Was Conducted in the Included Texts
Most articles investigated the use of a wearable EMG sensor for EMG data monitoring and assessments (33.3%). 9 –13 Some articles looked at algorithms for the compression of EMG signals to improve remote data transmission (20.0%). 14 –16 Some articles also compared the wireless portable EMGs to those typically used clinically to evaluate their strengths and weaknesses (20.0%) 17 –19 A few articles focused on studying the remote-based EMG sensor placement for the highest signal accuracy and comparing it to a research-grade (or clinically used) sensor (13.3%). 20,21 Finally, a few articles focused on cloud-based systems for remote real-time information and data, unreliable real-time data (13.3%). 22,23
Most of the articles were conducted in a laboratory setting (60.0%). Laboratory setting studies were done to design a specific device (i.e., wearable) for ease of use in a virtual setting. Two studies were done in a remote clinical setting (13.3%). Clinical setting encompassed both clinic-to-clinic and clinic-to-home models. The clinic-to-clinic model is when the patient is at a remote clinic with a clinical assistant and the specialist is located in a virtual setting. The clinic-to-home model is when the patient is at home and the specialist is located in a virtual setting. The articles did not mention which model was used. Finally, one study was conducted in a laboratory and then described a case study in a remote clinical setting (6.7%). In addition, two articles were reviews (13.3%), and one described a system (6.7%). Most studies were conducted with healthy participants (7 of 12 articles, 58.3%). The settings and the types of participants are presented in Tables 2 and 3, respectively.
Description of the Study Setting
Types of Participants
From 12 articles; 2 articles were reviews, and 1 article was a simulation exercise.
BARRIERS TO CONDUCTING EMG ASSESSMENTS VIRTUALLY
Several barriers to conducting EMG assessments virtually were identified in the included articles. The most common barrier was related to the delayed or unreliable real-time data of EMG signals in telemedicine due to high bandwidth consumption (of up to 500 Hz) and the large amounts of data to be processed (80%). 10,12,14,16,17,20 –23 Some articles also mentioned that wireless EMG systems have high power consumption and low energy efficiency (13.3%). 17,23 Cybersecurity issues to ensure data confidentiality were also raised as a concern (13.3%). 17,23
The second most common barrier mentioned in the articles was poor patient usability or user-friendliness in the clinic-to-home model (40.0%). 9,11,17,19,21,23 In this model of virtual EMG use, the patient is expected to apply the electrodes on their own. Because of the bulky equipment, the patients found it difficult to attach the electrodes to themselves without the clinician's intervention. One article described that the surface EMG electrodes they used were too rigid and lacked flexibility, preventing their use as a wearable technology. One article mentioned that EMG electrodes required the electrodes to be at the exact anatomical location to obtain accurate recordings. Another article mentioned that there was variability in the sensor location across sessions. It was also difficult for the patient to pair the EMG sensor system to the application on the computer due to technological difficulties. One article mentioned that the system required a minimum level of computer knowledge to set up and utilize. Barriers to virtual EMG assessments are summarized in Table 4.
Barriers to Virtual Electromyography Assessments
OVERCOMING BARRIERS TO CONDUCTING EMG ASSESSMENTS VIRTUALLY
The articles described various solutions by which the identified barriers could be managed to address the issues related to conducting EMG assessments virtually.
Patient usability and user-friendliness
All articles that identified issues related to poor patient usability or user-friendliness proposed a solution for this barrier (33.3%). 9,11,12,18,21 Improvements in patient usability were recommended through more interactive instructions on how to operate the EMG independently. For example, two articles suggested adding tips and techniques progressively throughout the sessions. 9,21 Another article included an options menu for the software, which contained additional options for user support. 18 In some articles, a regular video chat between the clinician and patient would occur to monitor the patient and provide technical support. This ensured that the electrodes were placed correctly and that the EMG data were obtained accurately. 18,21 Another solution proposed regarding the bulkiness and rigidity of the system was to use an ultrathin wearable EMG electrode (20.0%). 10,12,18 One article described one such system made of a polyimide film in a honeycomb layout to allow for better flexibility and breathability over extended periods of time.
It is important to note that usability will vary depending on the location. For example, in a clinic-to-clinic model where the EMG data are collected from a remote clinic and sent to a specialist in another location, usability may not be as large of an issue due to available help from a clinician on site. However, if the patient is being tested from home or a clinic-to-home model, it may be more challenging for a clinician to assist the patient in using the software or where to place electrodes, for example.
Real-time data
To address the reliability of real-time data, several articles described various EMG systems being developed and validated to address this (20%). 17,21,23 It is important to consider that the EMG system does not contain any significant data above 200 Hz when it is used clinically. These data are used for sequencing of the muscle or power spectrums to identify fast or slow fibers.
Data transfer latency could be managed through Fog computing architecture (6.7%). 22 Fog computing architecture is when a series of nodes will process the data in real-time when they receive it from the Internet of Things (IoT) device. The nodes will then send information to the cloud periodically. 24 Consequently, this will allow to distill the results, allowing less data to be transferred, reducing transmission delay. Cloud-based systems have been reported to have data transfer delays (latency). Delays increase with an increase in the number of sensors used since the cloud server must deal with the data from all the sensors at once. 22 Fog-computing architecture has been proposed as an option to minimize the delay and improve efficiency. It uses fog devices (nodes) as an extra data processing step that groups sensor data and then transfers it to the cloud server. This decreases the amount of individual sensor data transferred to the cloud server. 22
Signal transmission could be improved with new methods of signal compression techniques (13.3%). 14,16 For example, using discrete wavelet transform or deep convolutional autoencoders could reduce the size of the data without losing important information. These methods would be useful for minimizing data storage or removing irrelevant information within the data for better and faster data processing. 14,16 However, it is important to note that signal transmission speed will depend on the clinician's goal and what they are trying to assess. Raw data transmission that is postprocessed transfers much larger amounts of data than if edge or fog computing is used (i.e., where the amount of data that is transmitted is much lower as it has already been processed). Edge or fog computing would allow to reduce the latency of the data being transmitted.
Bandpass filtering, a technique that allows frequencies within a specific range and rejects frequencies outside that range, was proposed in three articles (20.0%). 10,13,21 The bandpass filter in one article had a bandwidth of 20–500 Hz and a notch filter of 60 Hz. However, while the two other articles used bandpass filtering, the type of bandpass filter used was not mentioned.
One article mentioned a dynamic bit allocation scheme which is a process for better utilization of the system's memory space so that the data adjust itself to the available memory capacity (6.7%). 14
POWER CONSUMPTION
A wearable system's most significant power demand is its wireless transmission. One study presented a novel EMG system that provided more power using a dual 9-V battery. One review article also suggested the use of dual 9-V batteries, passive electrodes with a battery for power supply on the sensor, or rechargeable Li-ion batteries to provide more power than the normal amount that needs to be consumed (13.3%). 17,23
SECURITY
While two articles mentioned that cybersecurity was an important consideration in telehealth, only one provided ways to ensure data privacy. Enhanced security was proposed through monitoring data in real-time, firewalls, anti-distributed denial of service (DDoS), Security Enhanced Linux (SELinux), and Virtual Private Network (VPN) (6.6%). 18 Anti-DDoS is used to prevent malicious attempts to make the system unavailable to users. SELinux is an access control program that enforces security on a system. It has mechanisms that separate system integrity and data confidentiality (multilevel security). VPN can also be used for increased security as it provides privacy and anonymity for online users through encryption. 18 Solutions to overcoming barriers to virtual EMG assessments are summarized in Table 5.
Ways to Overcome Barriers in Virtual Electromyography Assessments
DDoS, distributed denial of service; EMG, electromyography; SELinux, Security Enhanced Linux; VPN, Virtual Private Network.
Discussion
This scoping review identified 15 published articles relevant to the research questions. While the scoping review considered articles published since 2006, most were published in the last 4 years. Technological advancements in society, in general, may explain this increase in articles. Alternatively, it may be due to the pursuit of technology development in more recent years to make telehealth a more frequent and feasible application to use. The COVID-19 pandemic has required physicians and other health care providers to adapt their means to deliver health care quickly through the use of online tools and digital and virtual applications. Statistics have shown that in April 2020, almost half of the physicians in the United States started to use telehealth, up from 18% in 2018. One could assume that similar data could be seen globally. 25
The two countries with the most publications were Italy and the United States. Most of the remainder of the publications included in the scoping review was also from developed countries (Canada, Norway, and Japan), for a total of 60% of the articles published in developed countries. 26 This is consistent with studies that have shown that more programs have been attributed to telehealth in more developed countries. In 2019, it was estimated that the market for telehealth in the United States reached 43.4 billion dollars, with an annual growth rate of 17.7%. However, less effort has been put into telehealth in developing countries due to a smaller return on investment, a limited health care budget, and challenges due to limited technological infrastructure. 27 Future research should explore the differences in barriers between developed and developing countries and how the availability of the technology, research funding, and socioeconomic factors influence the differences between the two.
BARRIERS TO VIRTUAL EMG ASSESSMENT
The review revealed that the most common barrier to virtual EMG assessment reported in the literature was related to information technological infrastructure. The review characterized this as poor reliability of real-time data to remote locations and explained by the substantial amount of data collected. This barrier was reported in more than 50% of the studies. A significant concern was that poor reliability of real-time data could lead to wrong or delayed diagnosis due to the inaccessibility of the data. When high volumes of data are being processed, transmitting data to a remote cloud server can cause high latency and network utilization. Consequently, this may mean improper care for the patient and needless patient suffering.
Most commercial EMG systems use 1000 Hz sample rate. However, clinical data are typically in the range of 10 to 200 Hz range. Higher sampling rates provide an advantage to represent the amplitude of the EMG signal accurately. Nyquist theorem requires a minimum sampling rate that is twice the signal maximum frequency but also suggests that higher sampling rates give a better representation of the amplitude of the signal being sampled. A higher sampling rate will avoid missing essential data and better represent the amplitude envelope of your data. However, as mentioned, this creates high volumes of data processed and may cause this delay. It is also important to consider that there are two approaches you can use to transmit data. You can transmit data synchronously or asynchronously. Delay in asynchronous data is dependent on the duration of the measurement being made.
Phones, laptops, and tablets were used to measure EMG remotely in the study, all of which use different transmission paths. Most mobile and computing systems have the processing power necessary to transmit EMG data. Two approaches are widely used for wireless communication and were reported in the articles used in the scoping review. One approach is to use Bluetooth operating at 2.4 GHz and the other is ZigBee protocol operating at 902 MHz. Everyday microcontrollers are capable of communicating with both Bluetooth and ZigBee protocols. It is important to note that these different transmission paths may cause variations in the reliability of the real-time data being received remotely.
Some publications included wearable EMG devices as a rehabilitative intervention for neurological conditions (i.e., stroke). Wearable devices specifically are said to generate substantial amounts of data. Unfortunately, health care systems may have inefficient databases to store or analyze a large capacity of information. Therefore, further technological advancements are required to address data collection and storage before these devices can efficiently be adopted. 28
The second most reported barrier was poor patient usability or user-friendliness, reported in 40% of the articles, and unreliable real-time data, reported in 20% of the studies. The review reported that patients had difficulty attaching the EMG sensor to themselves or connecting the sensor to an application to self-monitor. Patient independence during the collection of EMG data remotely was challenging to achieve. This was primarily due to a lack of training before using the equipment. There is the risk that EMG data collection application without the direct involvement of the health care practitioner can lead to incorrect or incomplete data collection. These findings are consistent with what has previously been found in the literature regarding data collection obtained remotely with any medical devices in that usability is also a barrier, specifically for patients with any cognitive disability or low dexterity. 28
Elderly patients may also have difficulty reading the instructions to understand how to use the EMG device. 28 It is important to note that these barriers would only occur when data are being collected remotely or from the home to the clinic. In a clinic-to-clinic setting, the bandwidth of the clinic to acquire faster real-time data could easily be changed, and direct access to a clinician for assistance would improve user-friendliness.
OVERCOMING THE BARRIERS TO VIRTUAL EMG ASSESSMENTS
Various solutions to overcome the barriers were proposed in the published articles. Patient usability was one of the most frequently mentioned barriers in the studies and, not surprisingly, was the barrier in which most studies suggested ways to overcome this problem. This demonstrated that most studies focused on improving EMG virtual assessments centered around the patient's skill requirements. One solution to this barrier was increasing patient confidence and independence through prior training before use and technical support through regular videoconferencing. Another solution was implementing specific tips and techniques to collect EMG data independently, which was added progressively in certain applications for the specific concerns that participants brought forward. Some articles even proposed increasing patient engagement with their clinician by suggesting that clinicians remotely intervene directly with the software collecting EMG data using remote desktop features of the videoconferencing system.
User-friendliness was also mentioned in the articles, further highlighting that patient needs seem to be a priority in ensuring the success of virtual EMG assessments. This finding was expected because in telehealth providing exceptional patient usability and user-friendliness are essential to effective patient engagement and ensuring a positive patient experience. This aligns with the International Organization for Standardization definition of usability as “the extent a specific user can use a particular product or device to achieve goals of efficiency and satisfaction.” 29
Telehealth will only be made possible if patients are willing to participate. Most individuals will choose the most convenient option when choosing between in-person or virtual health care. Therefore, to improve telehealth and its popularity, most articles tended to focus on improving the ease of use for the patient. One option is to design how EMG data are collected (i.e., user-friendly software and hardware) tailored to individual users' needs. As such, this could significantly improve patient participation and adherence. 30
Poor reliability of real-time data was the most common barrier identified in the articles, yet very few articles proposed solutions to overcome this. This demonstrates a knowledge gap in the current literature. While studies raised this as a significant barrier that needs to be overcome to allow data to be transmitted efficiently without consuming a large amount of bandwidth, solutions have not yet been applied successfully.
Access to real-time data is important in certain clinical situations, such as obtaining a rapid result for immediate treatment or trying to synchronize a real-time assessment by video. Several articles described various EMG systems being developed and validated to address data reliability or to ensure that there is no delay in transmission in real-time. However, none suggested a hybrid approach where the preprocessed data would be sent in real-time and raw data asynchronously.
Strengths and Limitations
This scoping review identified articles of interest using two researchers who followed appropriate literature screening and study selection techniques. Data were extracted upon identifying relevant articles using a data extraction form designed a priori. The findings were grouped into similar themes. Disagreements between the reviewers were resolved by discussing and reaching a consensus.
Some limitations of the scoping review are worth noting. To start, the scoping review did not appraise the quality of the articles. Even if the goal of this scoping review was to identify the barriers and solutions of virtual EMG reported in the literature, and assessing the quality is usually not a component of a scoping review, quality assessments should be strongly considered before these findings are applied to improving future virtual EMG assessments for patient diagnosis and monitoring. In terms of limitations regarding the quality of the scoping review, the search was limited to two databases and only articles published in English were included. This may have led to missed studies, causing biased results as it narrowed down the search and the variety of articles obtained.
Furthermore, 40% of the articles were from the United States or Italy, with only one publication (6.7%) in Canada. This may limit the generalizability of the findings to the countries of origin. A study done by Man et al. indicated a publication bias where articles were most likely to be published in high-ranking journals according to their English proficiency and the amount of funds available for research. This may directly impact the number of articles published by developing countries. 31
Third, a broad search was conducted for any application involving virtual EMG assessments. Barriers to conducting EMG assessments may vary according to the condition being diagnosed or monitored. In addition, different conditions may have different needs and impairments, which would reflect specific barriers. For example, patients suffering from low dexterity due to stroke may have a more specific set of barriers, such as difficulty placing the electrodes. 28 However, a broader inclusion was used to get a bigger picture of general barriers to virtual EMG assessments as there is still not much research on the subject and, therefore, limited search results.
Furthermore, another limitation involves the increasing popularity of the telehealth field, which means that, as technology advances, other barriers may emerge according to such advances. It is important to acknowledge that the scoping review may only be relevant for a few years as the technology becomes more sophisticated, the identified barriers are removed or mitigated, and others are created.
In addition, the EMG electrode was not placed in the same area for each study reviewed. Multiple layers of muscle affect its ability to detect deeper muscle activity. Using EMG is significantly compromised as there is cross talk between different muscles. There can also be two or three different muscles that are all firing and contributing to the signal. Therefore, muscle bundles can be tricky. Consequently, the quality of the signal does vary according to where it is located.
Finally, it is safe to assume that the time or length of the EMG data collected varied per article, although this was not specific. This may have created a considerable difference in bandwidth consumption and real-time data per study. Bandwidth consumption may also vary dependent on the number of EMG channels used in the articles. Most articles used one EMG channel, but some used up to four. This may create a larger bandwidth consumption for those that use more channels, creating a large barrier to virtual EMG use.
Conclusion
In conclusion, as technology progresses, more and more health care practitioners are using telehealth as a means to monitor and diagnose patients.
According to the published articles, the most commonly identified barriers to using virtual EMGs were poor patient usability of the device and signal and data transmission issues. This was followed by barriers which included high power consumption of battery-based systems and issues with cybersecurity.
Most articles solved the barrier of patient usability by adding very precise and interactive instructions that would make it easier to follow remotely. To have more accurate real-time data, many articles proposed to include fog computing architecture to allow the periodic transmission of information. Signal compression techniques and bandpass filtering were also proposed. Furthermore, the high-power consumption of battery-based systems was overcome by changing the battery to dual 9-V or Li-ion batteries. Finally, articles suggested using firewalls, anti-DDoS, SELinux, and VPN for better cybersecurity.
Various solutions were proposed; however, further research is required to determine if these solutions have resulted in enhanced use of virtual EMGs and improved clinical outcomes for the patient. Future studies should also consider how to overcome data security in EMG virtual assessments, as there was limited information found during the review.
The results of the scoping review may be helpful to clinicians wishing to offer virtual EMG assessments. It may be used to improve clinical practice by developing best practices for using EMG virtually. It may lead to engineering research to improve virtual EMG. With constant advances in the technology used for telehealth, it is a question of time before many of the barriers to using EMG virtually become issues of the past.
Footnotes
Authors' Contributions
V.N. contributed to writing—original draft, review and editing; methodology; validation; formal analysis; investigation. E.O. contributed to methodology; validation; investigation. M.F.-P. contributed to writing—review and editing; conceptualization; and supervision. L.D. contributed to writing—review and editing; methodology; resources.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.