
Abstract
Purpose:
This systematic review aimed to identify the types and effectiveness of telenursing in home health care (HHC) compared to conventional HHC.
Methods:
This study followed the Preferred Reporting Items for Systematic Review and Meta-Analysis 2020 guidelines. A random-effects meta-analysis was performed. The risk of bias was assessed using the Risk of Bias 2.0 tool. The quality of bias was evaluated using the Grading of Recommendations Assessment, Development, and Evaluation system.
Results:
A total of 17 studies published between 2003 and 2022 were included in the review. The majority of the targeted health conditions of the patients were chronic obstructive pulmonary disease or congestive heart failure (70%). We categorized telenursing interventions according to different technology (N = 4) and nursing (N = 7) types. Among the identified types of nursing, fundamental nursing to monitor patients' symptoms was the most representative. Telemonitoring was found to be the most common technology type, followed by synchronous technology using video or telephone. The telenursing outcomes, including health care utilization, physiological/psychological outcomes, and quality of life, varied. In the meta-analysis, participants who received telenursing reported fewer hospital admissions (standardized mean difference [SMD]: −0.18; confidence interval [95% CI]: −0.43 to −0.02) and emergency department visits (SMD: −0.28; 95% CI: −0.45 to −0.10).
Conclusion:
Telenursing in HHC tends to improve the quality of life and could result in many benefits, including a reduction in health care utilization and facilitating the management of chronic diseases. These results ultimately represent the potential effectiveness of telenursing in community health care settings.
Introduction
Telenursing can be defined as “the use of telecommunication and information technology to provide nursing practice at a distance.” Hence, it can range from simple tasks, such as faxing medical records, to providing more complicated nursing care in patients' homes by utilizing cameras and computer technologies. 1 Telenursing is broadly classified into four main types: (1) synchronous, (2) asynchronous (store-and-forward), (3) remote monitoring, and (4) mobile health. Moreover, it can be performed by transmitting voice, data, images, and information instead of actual movement of patients or medical staff. 2 Recently, telenursing has been growing rapidly in various countries as a result of aging populations and chronic disease, especially in the era of the coronavirus disease 2019 (COVID-19). Moreover, along with the development of information technology, telenursing has become the nursing paradigm of the 21st century. 3
Home health care (HHC) is provided by various health care professionals at home, independent of hospital environments. The goal of HHC is to provide care for patients with illness or injuries and help them regain their independence as much as possible, with the ultimate goal being to enable them to achieve and maintain the highest standard quality of life and to learn to live with their own illness or disability while reducing medical expenses. 4 On account of aging populations and the increasing prevalence of chronic disease, there is a need for shifting the scope of health care from hospital-based care to a convenient, easily accessible method, such as HHC, for patients and their families. 5 We defined HHC as the care provided by health care professionals, including nurses, at the patients' homes. 6
Telenursing can be used as one of the effective methods of HHC. Health care professionals, including nurses, can deliver HHC services to patients in several ways. They can directly visit the patients' homes, known as conventional HHC (face-to-face care), or indirectly visit patients using information and communication technology, known as telehealth or telenursing. 7 Owing to the long-standing nature and need for frequent monitoring in chronic disease management, telenursing can be successfully applied to HHC patients with chronic diseases such as diabetes, congestive heart failure (CHF), and chronic obstructive pulmonary disease (COPD). 8,9 HHC can result in multitudinous benefits to both patients and health care providers. Previous studies have reported improved patient outcomes, including better quality of life, reduced readmission rates, and cost-effectiveness, associated with telenursing in HHC. 10 –12
To effectively utilize telenursing in HHC, it is imperative to identify the specific types of telenursing that have been performed so far and to systematically check the efficacy of telenursing according to the nursing type. However, to the best of our knowledge, very few systematic reviews identifying the effects of telenursing in HHC have been conducted. Moreover, there is currently no such review in the literature that summarizes the types of telenursing according to the technology and nursing type used. This study was performed to address this gap in knowledge by providing crucial evidence on the efficacy of telenursing and to further determine the differences among the types of telenursing utilized in HHC. Therefore, this study aimed to provide information on the characteristics of telenursing interventions and identify the effects of telenursing in HHC compared with conventional face-to-face HHC.
Methods
CORE QUESTIONS
This systematic review used the Participants, Intervention, Comparison, Outcomes criteria to formulate the research questions. Participants included patients who had received HHC services provided by health care professionals. Intervention was defined as telenursing in an HHC setting. A comparison was made with conventional home care, which refers to face-to-face HHC services. We focused on the types and effects of telenursing on the outcome in patients receiving HHC.
DESIGN
This review followed the recommendations of the Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines and was carried out according to the protocol of the International Prospective Register of Systematic Reviews, with the registration number CRD42022371634. This study is a literature review and has been exempted from review by the Seoul National University IRB committee.
ELIGIBILITY CRITERIA
Eligible studies included those that implemented a randomized controlled trial (RCT) design and of which the full text was published in English. Studies were excluded when they did not focus on the effect of telenursing in HHC, when the providers of the intervention were not nursing professionals, or when the target of telenursing on other medical staff, rather than the patient, was the investigated outcome. In addition, studies in which the participants were aged <18 years were excluded. Studies published between 1997 and 2022 were eligible for selection. This time period was chosen due to the emergence of telenursing since 1997. Furthermore, the American Nurses Association first published an official definition of telenursing that year, 13 and the American Academy of Ambulatory Care Nursing also officially embraced telephone nursing as a subspecialty of ambulatory care nursing and published its standards. 14 The eligibility criteria are listed in Table 1.
Study Search Eligibility Criteria
HHC, home health care.
SEARCH AND STUDY SELECTION
Studies were identified by searching the following electronic databases: PubMed, Excerpta Medica Database, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Library, and ProQuest. A brief description of the keywords used in the search can be found in Table 2. The search terms were developed by the research team and reviewed by a medical librarian. The final search strategy for CINAHL is provided in the Supplementary Data S1.
A Brief Description of the Search Terms
RCT, randomized controlled trial.
Note: Combine A and B–G into “AND,” the results of No. 1, 2, and 3 were combined into “AND” to complete the final search queries.
Asterisks indicate search term truncation.
For screening studies, we used Covidence®, an internet-based software program. All three reviewers independently screened the titles and abstracts to select all relevant studies. These studies were subsequently reviewed by each reviewer based on the predetermined eligibility criteria (Table 1) by screening the full text. Discrepancies in the process were resolved through a group discussion involving all three reviewers.
QUALITY APPRAISAL
The Cochrane risk of bias tool (RoB) for randomized trials (version 2.0) was used to evaluate the quality of the included studies. The three reviewers independently assessed the quality of each selected study and provided appraisal scores for each. Studies were given a final rating of low risk, some concerns, and high risk using RoB 2.0. 15
DATA EXTRACTION
Data were manually extracted from the full text independently by the three reviewers. From each study, we extracted the following data: author and year of publication, country, target population, number of participants (number of intervention/control group participants, mean age, and standard deviation of age), characteristics of the intervention (duration, providers, and characteristics of control [conventional HHC]), types of technology used, types of nursing intervention, time point of data collection, outcome measurement tool, and results. The data extraction table can be found in the Supplementary Data S4.
QUANTITATIVE SYNTHESIS
Meta-analyses were conducted for quality of life, patient satisfaction, self-efficacy, depression, hospital admission, emergency department (ED) visits, length of hospital stay, and cost to Medicare using Review Manager® (version 5.4.1). To determine the effect size of each outcome, standardized mean differences (SMDs) were calculated with confidence intervals (95% CIs) for each respective variable.
Owing to the foreseeable complexities and multicomponent properties of the intervention and various target populations of the included studies, a random-effects model was used to pool the outcome measures across studies, which allowed the generalizability of the estimated effect. 16 To measure the heterogeneity of the intervention effects in the included studies, the Higgins I 2 test was performed. Subgroup analyses were conducted to explore the differences in the effect of telenursing between the data collection time points of each of the study outcomes (3-month follow-up and the full study period). Publication bias was assessed by visual inspection of the funnel plots.
QUALITY OF EVIDENCE ASSESSMENT
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system was applied to determine the quality of evidence from the primary outcome measures. The GRADE system classifies the quality of a body of evidence as high, moderate, low, and very low.
Results
SEARCH OUTCOMES
A total of 1,246 studies were identified following the initial search across all the databases, of which 380 were duplicate studies. The titles and abstracts of the remaining 866 studies were screened (Fig. 1). Upon thoroughly scanning the titles and abstracts, 786 studies were excluded from the review, and 79 studies, excluding one article without a full text, were further assessed. A list of 79 full text screened studies and the reasons for their exclusion can be found in the Supplementary Data S2. A final total of 17 studies were included in the systematic review.
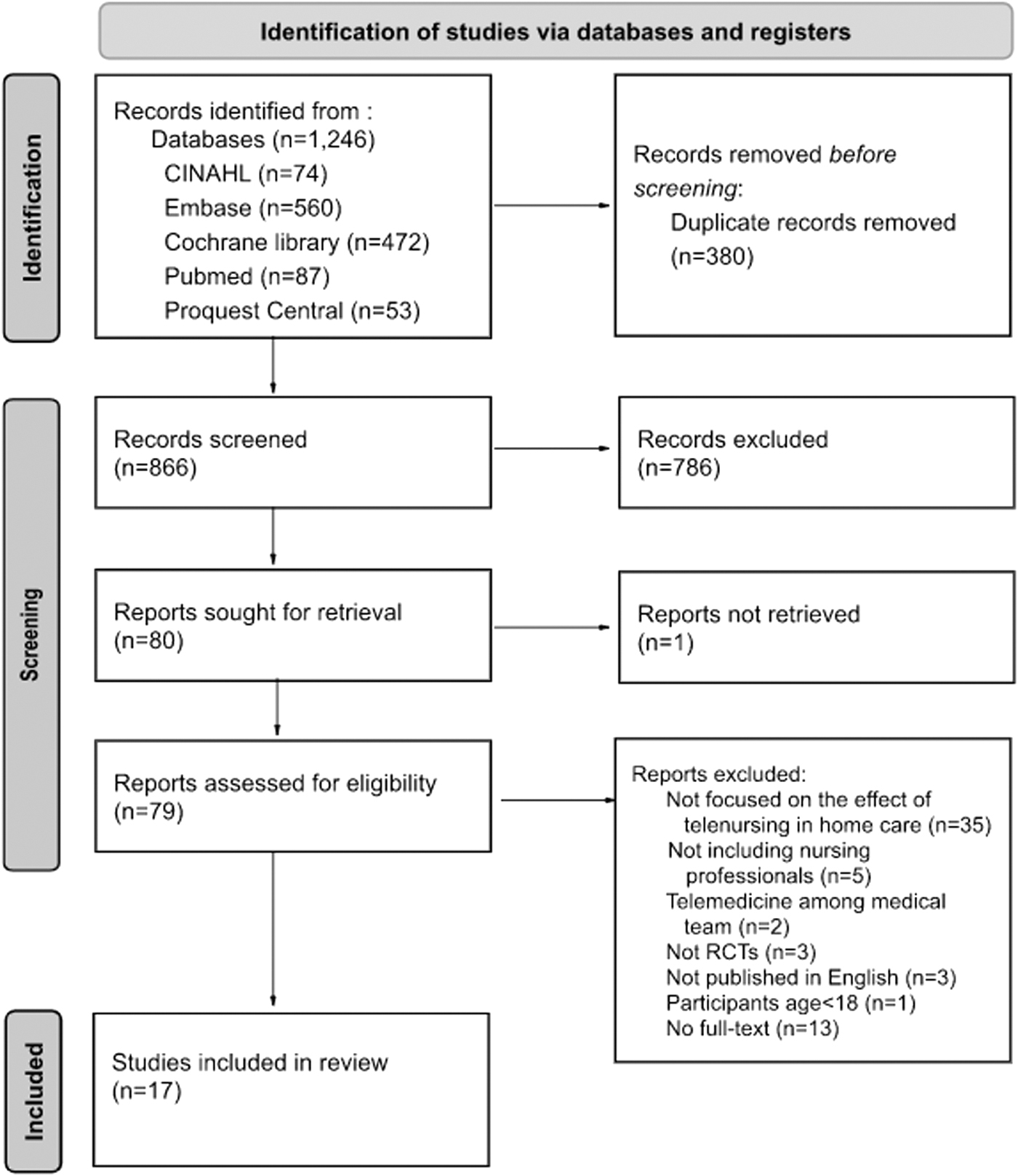
Flow diagram of study selection. CINAHL, Cumulative Index to Nursing and Allied Health Literature; RCT, randomized controlled trial.
QUALITY ASSESSMENT OF THE SELECTED STUDIES
The information included for the quality assessment of the selected literature using RoB 2.0 is shown in Figure 2 and the Supplementary Data S3.
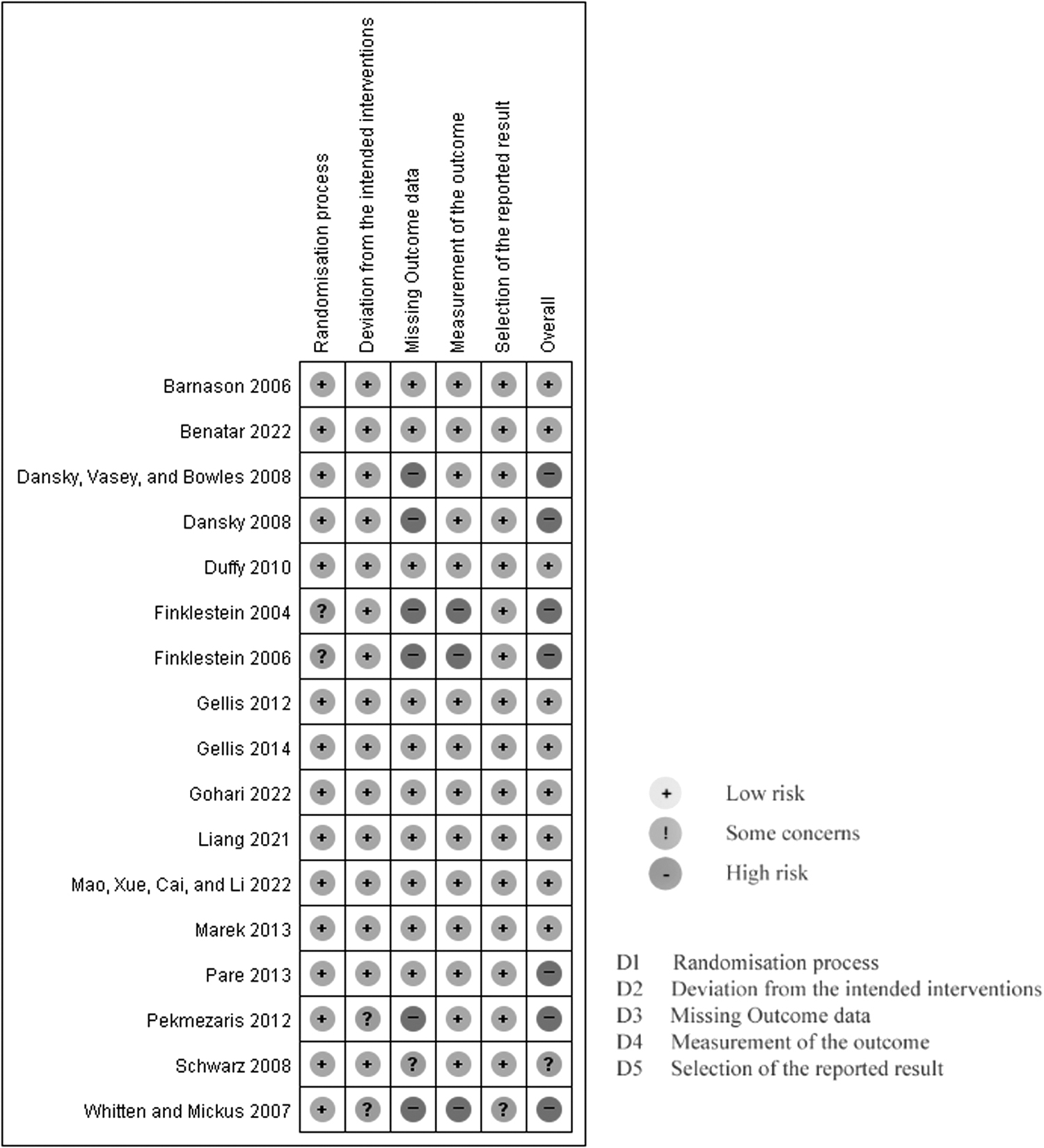
Quality appraisal results for individual studies.
With the exception of two domains, “missing outcome data” and “measurement of the outcome,” the overall quality of the included studies was high across the remaining domains. No studies were judged as having a high RoB in the “randomization process,” “deviations from intended interventions,” and “selection of the reported result” domains. Upon integrating the biased results of the aforementioned domains, seven, one, and nine studies were evaluated as having a “high” RoB, “some concerns,” and a “low” RoB, respectively. Studies were not excluded based on their quality appraisal results to consolidate all the available evidence and enhance the rigor of the synthesis.
CHARACTERISTICS OF THE SELECTED STUDIES
The general characteristics of the included studies and information concerning the intervention according to the nursing and technology types can be found in the Supplementary Data S5.
General characteristics
The selected studies were published between 2003 and 2022. The majority of the selected studies (76%) were conducted in the United States (study 1, 2, 3, 6, 7, 8, 10, 12, 13, 14, 15, 16, and 17). The total sample size of the selected studies ranged from 32 to 414 participants, and the mean age of the participants ranged from 60 to 83 years (mean age: intervention group, 77.03 years; control group, 81.90 years). The targeted health conditions of the patients in each study varied. However, the majority of studies (70%) targeted patients with COPD or CHF (study 1, 2, 3, 5, 6, 7, 10, 13, 14, 15, 16, and 17). The target population of the included studies included patients with COPD (64.7%), CHF (35.3%), coronary artery bypass graft surgery (CABG) (11.8%), chronic wound care (11.8%), carotid artery stenosis (5.9%), and multiple chronic illnesses (5.9%). The intervention providers were composed of a wide range of health care workers; however, a nurse always played the key role in the administration of telenursing interventions. Further details can be found in the Supplementary Data S4.
Interventions according to the nursing type
The categories of nursing applicable to telenursing can be classified into (1) fundamental nursing, (2) education and training, (3) consultation, (4) medication and injection, (5) therapeutic nursing, (6) testing, and (7) referrals. 17
In the selected studies, fundamental nursing was administered in most studies (88.2%), followed by education and training (70.6%) and consultation (70.6%) (Fig. 3).

Interventions according to the nursing type.
When administering fundamental nursing, 15 of the 17 selected studies reported that the patient's signs and symptoms were monitored using telenursing. Thus, for telenursing, fundamental nursing was the representative nursing category used for monitoring patients.
Across all categories of nursing utilized in telenursing, education and training and consultation accounted for 25.5% of the nursing administered. Education and training nursing included various programs for diet, exercise therapy, methods of medication, and treatment methods. Medication and injection nursing included the management, monitoring, alarm related to medication, and drug titration according to the patient's daily symptoms, status, and side effects. Furthermore, nursing of the medication and injection type accounted for 29.4% in 17 studies, mainly consisting of medication management that allowed appropriate doses to be administered at a specified time and management of the side effects.
Therapeutic nursing was observed in two of the selected studies. In a study by Gellis et al. (Study 3), problem-solving therapy, a type of cognitive behavioral therapy, was conducted every week according to a five-step procedure. In the study by Barnason et al. (Study 8), postoperative nursing, such as patient recovery symptom management and surgical wound care through telenursing, was provided to patients who had undergone CABG. In one study, self-administered O2 saturation testing was performed by patients and guided during videoconferencing with an HHC nurse (Study 6).
Interventions according to the technology type
Telenursing interventions use a variety of technologies. Studies were categorized based on the technology utilized in the telenursing intervention. As shown in Figure 4, we classified these telenursing interventions into four categories based on the technology type: (1) real time or synchronous, (2) store and forward or asynchronous, (3) telemonitoring or remote monitoring, and (4) mobile health. Real time or synchronous means that the information or data are transmitted in real time. 1 In 12 studies (70.5%) that used real-time or synchronous technologies, interventions were conducted by videoconferencing or virtual visits (Study 6, 7, 10, 15, 16, and 17) or telephone calls in real time (Study 1, 2, 4, 5, 9, and 14). As for telenursing through telephone, this method of communication enabled the nurse to remotely exchange data with patients, assess their health-related problems, support them, and intervene (such as urgent home visits) as necessary (Study 2, 5, and 14).

Interventions according to the technology type.
Asynchronous means that the information was transmitted after recording. 1 Five studies (29.4%) used store and forward or asynchronous technologies (Study 8, 12, 15, 16, and 17) for performing various functions for both nurses and patients. One of the functions of this technology in telenursing is to enable patients to independently record their own measurements through peripheral devices and transmit the readings to the nurse using a one-way monitoring system (Study 15). In telemonitoring or remote monitoring, medical devices record and process information and transmit it to the medical team in real time (synchronous) or in summary form (asynchronous). 1 The majority of the selected studies (76.4%) used telemonitoring and remote monitoring technologies. In these studies, basic vital signs (heart rate, blood pressure, pulse, oxygen saturation, and temperature), weight, and patient symptoms were monitored daily. Thereafter, the nurse could remotely monitor the patients' health status and adherence to ongoing treatment.
Mobile health means using mobile and wireless devices to improve health outcomes, health care services, and health research. 1 Only one study used this type of technology, thereby accounting for the smallest percentage (5.9%) of utilized technologies (Study 11).
RESULTS OF THE OUTCOMES
The outcome measures of the included studies were categorized into six groups: quality of life and perception, physiological outcomes, psychological outcomes, health care utilization, self-management, and caregiver aspects (Table 3).
Outcomes Measured in Individual Studies
ED, emergency department.
Four RCTs compared the effects of telenursing in HHC with conventional care based on the quality of life (Study 1, 11, 13, and 14). A significant improvement in quality of life was only reported in two studies (Study 11 and 14). Regarding the physiological outcomes, the mortality rate declined in two studies that measured the rate of mortality. Considering the psychological outcomes of telenursing, five studies measured depression but reported contradictory results. Two studies (Study 2 and 3) indicated that the application of telenursing in home care reduces the prevalence of depression, whereas a further study (Study 14) reported that depressive symptoms tended to decrease in the intervention group. However, the observed differences were not significant.
In the health care utilization category, four and five studies measured the rate of readmission to hospital and ED visits, respectively. Both outcomes demonstrated mixed results related to the efficacy of each study. First, in the case of readmission, two studies (Study 5 and 14) reported that the application of telenursing significantly lowered readmission. However, one study (Study 15) reported that HHC was only partially effective, and the readmission rate was only reduced for the 60-day follow-up and not for the full study period. Among the studies measuring the ED visits, three studies (Study 2, 3, and 5) reported that telenursing significantly reduced the number of ED visits, whereas one study (Study 15) additionally reported that ED visits were only reduced for the 60-day follow-up.
META-ANALYSIS
Quality of life and perception
Among the 17 included studies, 4 studies (Study 1, 11, 13, and 14) explored the effects of telenursing in HHC on the quality of life using different instruments. The pooled SMD of the quality of life between the telenursing and conventional home care groups was not significant for either the 3-month follow-up period (SMD: 0.29; 95% CI: −0.18 to 0.77) or the full study period (SMD: 0.56; 95% CI: −3.06 to 4.18) (Fig. 5). The results indicated high heterogeneity of studies which included a 3-month follow-up and the full study period (I 2 = 84%). Two of the selected studies (Study 1 and 3) assessed the effects of telenursing on participant satisfaction during HHC. The results of the random-effects estimate on participant satisfaction were not significant (SMD: 0.20; 95% CI: −0.45 to 0.86; I 2 = 62%).

Forest plots demonstrating the effects of telenursing in home health care on different outcomes. CI, confidence interval; SD, standard deviation.

Psychological outcomes
Four studies (Study 2, 3, 13, and 14) explored the effects of telenursing in HHC on depression using different instruments. As shown in Figure 5, the results of random-effects pooled estimates of depression were significant (SMD: −0.74; 95% CI: −1.42 to −0.06). However, the current results indicated high heterogeneity in four studies (I 2 = 91%). Two studies (Study 4 and 14) examined the effects on self-efficacy. The pooled SMD for self-efficacy was not significant (SMD: 0.59; 95% CI: −0.25 to 1.43; I 2 = 90%).
Health care utilization
Five studies (Study 2, 3, 5, 13, and 15) assessed the ED visits of the participants. The random-effects pooled estimates of ED visits were revealed to have a significant effect on telenursing in HHC (SMD: −0.28; 95% CI: −0.45 to −0.10). The current results indicated low heterogeneity in five studies (I 2 = 25%). Hospital admissions were reported as an outcome in four of the studies (Study 5, 13, 14, and 15). The results from the random-effects pooled estimates of admissions were significant (SMD: −0.18; 95% CI: −0.43 to −0.02; I 2 = 20%). The length of hospital stay was reported as an outcome in four studies. The results of the random-effects pooled estimates on the length of hospital stay were not significant (SMD: −0.24; 95% CI: −0.58 to 0.09; I 2 = 67%). Two studies assessed the effect of telenursing on the cost to Medicare. The pooled SMD effects were not significant (SMD: 0.05; 95% CI: −0.22 to 0.33; I 2 = 12%).
Publication bias
Funnel plots were generated for each outcome to assess publication bias in this systematic review. As shown in the Supplementary Data S6, visual inspection revealed that the funnel plots on depression, ED visits, and length of hospital stay were symmetrical. Although the shapes of the funnel plots were asymmetrical for the other outcomes, confirming whether publication bias exists is challenging due to the number of included studies being lower than 10. 18
THE QUALITY OF EVIDENCE OF THE MEASURED OUTCOME
The quality of evidence for this review was evaluated using the GRADE system. There were one, four, and three studies with moderate-quality, low-quality, and very low-quality evidence, respectively. The quality of evidence for the outcome measures was downgraded owing to an elevated RoB, lack of precision, and inconsistent results. Further details are provided in the Supplementary Data S7.
Discussion
GENERAL INTERPRETATION OF THE RESULTS
In this systematic review and meta-analysis, we attempted to summarize the published evidence in the literature to ascertain the effects of telenursing intervention in HHC in terms of quality of life and perception, physiological outcomes, psychological outcomes, health care utilization, self-management, and caregiver aspects. Overall, the findings of this review suggest that telenursing intervention in HHC may result in reduced depression and lower hospital admission rates and ED visits compared with conventional face-to-face care. However, no significant differences across groups were observed in quality of life, participant satisfaction, and self-efficacy. Although there are some limitations to this analysis due to the heterogeneity of the included studies, the findings of this review strengthen the evidence of the potential efficacy of telenursing interventions in HHC.
Based on the findings of this review, telenursing interventions in HHC can vary according to general characteristics, especially according to the nursing and technology types. Moreover, telenursing interventions had various effects on HHC patients, as well as their caregivers. Depending on the nursing and technology types, various nursing services could be provided to patients using a variety of technologies, either independently or in combination, in HHC. Therefore, nurses play an essential role in the course of treatment using technology when providing nursing care in HHC. These findings provide valuable insight into the scope and value of nursing, the technological aspects of nursing, and ultimately the potential effectiveness of telenursing in community health care settings such as HHC.
Considering the targeted health conditions of the patients, the majority of diseases (70%) included COPD and CHF. These results could be attributed to the country in which the study was conducted. Several of the studies (76%) were conducted in the United States, where the major health burdens include COPD and CHF, especially in the aging population. 19,20 Patients with COPD and CHF need continuity of care. Thus, individualized case management and telenursing can ensure that patient needs are met.
Finally, the range of the measured outcomes in the study was very wide and included health care utilization, physiological/psychological outcomes, quality of life and perception, self-management, and caregiver aspects. Although the measured outcome was not effective in all the areas and inconsistent among studies, telenursing in HHC could affect a wide range of aspects of patients, not just limited to physical health, and has the potential to bring about a variety of outcomes. Therefore, more telenursing studies are warranted to assess the inconsistent results and to confirm the efficacy of telenursing in HHC.
STATUS OF TELENURSING IN HHC
The studies included in our systematic review were published between 2003 and 2022. Studies have been categorized into three groups: (1) studies published from 2003 to 2009, (2) studies published from 2010 to 2019, and (3) studies published from 2020 to 2022. The time classification for the second group reflects a period characterized by a significant global increase in smartphone penetration rates, particularly in 2010. 21 For the third group, the time classification reflects the impact of the COVID-19 pandemic, which greatly influenced the widespread adoption of telehealth, particularly after 2020. 22
Among the identified trends in telenursing, the application of telemonitoring according to the types of technology did not change over time and was consistent across all of the publication time periods. Hence, the highest utilization of telenursing was for nurses to receive and monitor various vital signs and bio-signals of home care patients without spatiotemporal restrictions (Table 4). Interestingly, the use of real-time video intervention has decreased over time, and telenursing using telephones has become more prominent (Fig. 6). This could be explained by the general tendency toward telemonitoring. Telephones are utilized by nurses as a means to analyze data transmitted through telenursing for providing counseling or education to patients and adjusting medications. They also have the added benefit of being widely accessible to patients and have significantly reduced installation and running costs compared with real-time video technology.
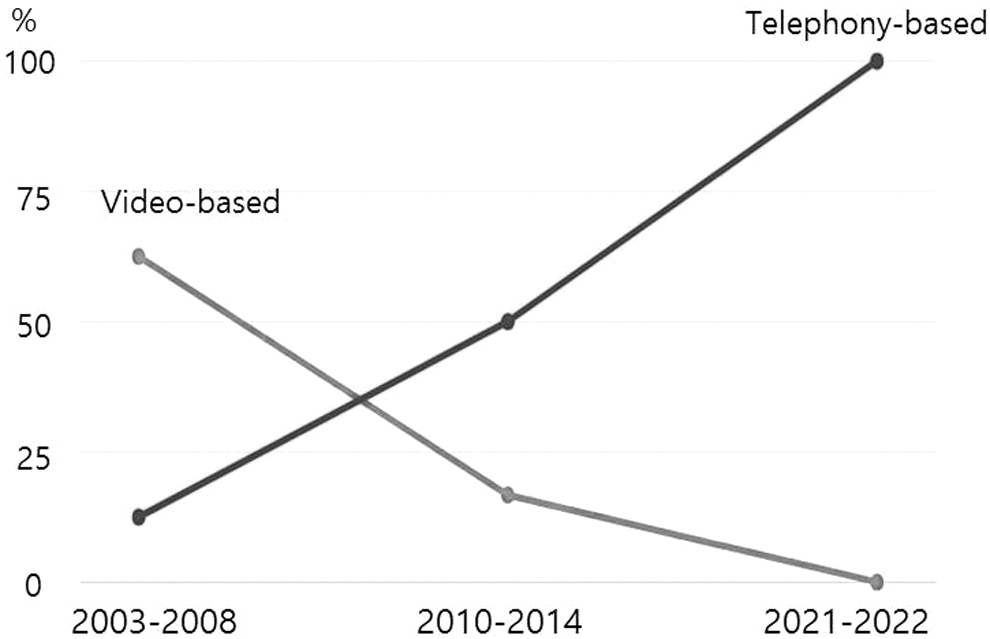
Status of the technology types according to the trend over time.
Status of Technology Types According to the Trend Over Time
Telenursing through smartphones belonging to the mobile health category was observed in only one study published in 2021 (Study 11). Two reasons were considered for this unexpected outcome.
First, owing to the characteristics of home care, the older adult population accounts for the majority of the home care patients. 23 Using this brand-new technology could have been challenging for older adults because smartphones are not user-friendly compared with other technologies, such as phones and videos. Although some previous surveys reported that mobile and tablet internet usage among older adults was higher than internet usage on computers, 24,25 the number of older adults who use smartphones is still very low. Therefore, we should identify the barriers to older adults' acceptance of technology in future studies and take these into consideration when implementing new technology, such as smartphones, to be utilized by older adults in HHC. These barriers could include the small size of the device, complexity of the device interface, cost, physical and cognitive impairments, and usage difficulty. 26 Second, due to the topic of our review, which focused on telenursing and not telehealth, since 2015, only three RCTs exploring the effect of telenursing in home care were suitable for inclusion. This may not reflect the recent trend of smartphone usage in telemedicine.
SUMMARY OF THE META-ANALYSIS
Overall, the results from the meta-analysis demonstrated that telenursing in HHC could have an impact on depression (SMD: −0.74; 95% CI: −1.42 to −0.06) and health care utilization compared with conventional face-to-face home care. In particular, participants who received telenursing in HHC reported fewer hospital admissions (SMD: −0.18; 95% CI: −0.43 to −0.02) and ED visits (SMD: −0.28, 95% CI: −0.45 to −0.10). The results of this meta-analysis demonstrate that telenursing during HHC resulted in significant reductions in total health care utilization. These results indicate that reductions in health care use may result in the potential reduction of the cost of Medicare. A previous systematic review on the effect of telehealth services compared with conventional home care also demonstrated that the potential benefits of telenursing include its cost-effectiveness owing to a reduction in the rate of hospitalization, ED visits, and mortality and improved quality of life. 27
In conclusion, a significant reduction in health care utilization, such as ED visits and hospitalization, indicates the potential benefits of telenursing in HHC. This result demonstrates that telenursing in HHC can prevent the progression of chronic diseases, resulting in the reduction of complications by providing the participants with continuous monitoring and an immediate response. The findings of this meta-analysis offer insights into the potential effectiveness of the technological applications for HHC.
STRENGTHS AND LIMITATIONS
This review had some limitations. Language and national biases could exist since the search was limited to literature written in English. Owing to the restricted criteria in this review, only three studies published since 2015 were included in the review, which may not reflect the recent trends in telehealth technology, especially concerning mobile health. Therefore, various types of technology that have been widely used in telenursing or telemedicine in recent years, such as mobile applications, smart watches, and artificial intelligence, have not been mentioned in these studies. The results of the meta-analysis of this review are limited owing to the heterogeneity of the included studies; therefore, caution should be exercised when interpreting the results. Nevertheless, this study reports some meaningful results which significantly help in understanding telenursing in HHC. Considering previous studies on telemedicine applications in HHC, very few have focused on telenursing. Therefore, our study represents the benefits of telehealth applications with a special emphasis on nursing.
Our review describes the technical and nursing aspects of telenursing, as well as the current status and benefits of telenursing in HHC. Furthermore, our research findings demonstrate the potential of telenursing to be applied in nursing beyond HHC. The various advantages of telenursing demonstrated in our study suggest that it can be an innovative solution to nursing challenges, such as geographical barriers, workforce shortages, and the increasing prevalence of chronic diseases. By leveraging technology and remote care delivery, telenursing can contribute to improving access to health care, enhancing chronic disease management, optimizing health care utilization and costs, and addressing nursing workforce issues.
Conclusions
This study clearly demonstrates that telenursing in HHC has many benefits, especially in reducing health care utilization and facilitating the management of chronic diseases. These results demonstrate the potential of telenursing in HHC. This review further emphasizes the value of nursing practice, technological aspects of telenursing, and ultimately the potential efficacy of telenursing in community health care settings. Moreover, considering the tendency of home nursing, which is expanding not only to patients but also to caregivers, the growing trend of remote care preferences attributable to the COVID-19 pandemic, coupled with the advancement in information and communication technology, the potential benefits and efficacy of telenursing in HHC are clearly highlighted in this review.
Footnotes
Authors' Contributions
Conceptualization and study design: M.M., Y.P., J.H., and K.W.; literature search and data collection: M.M., Y.P., and J.H.; study selection and methodologic quality assessment: M.M., Y.P., and J.H.; data analysis and interpretation: M.M., Y.P., and J.H.; drafting article: M.M., Y.P., and J.H.; supervision: K.W.; and critical revision: M.M. and K.W.
Availability of data,code,and other materials
Supplementary Data: (1) Search History (CINAHL), (2) List of Studies, (3) Quality Appraisal for Each Domain, (4) General Characteristics of Included Studies, (5) Technology Type and Nursing Type, (6) Funnel Plots of the Outcomes of the Meta-analysis, (7) Results of Evidence of Quality Evaluation, (8) List of the 17 selected studies.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the BK21 Four Project (Center for Human-Caring Nurse Leaders for the Future) funded by the Ministry of Education (MOE, Korea) and National Research Foundation of Korea (NRF). The grant numbers for funding is 4120200413721. This research received support from the Ministry of Education (MOE, Korea) and the National Research Foundation of Korea (NRF).
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4
Supplementary Data S5
Supplementary Data S6
Supplementary Data S7
Supplementary Data S8
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.