
Abstract
Background:
Telehealth is an emerging method which may overcome barriers to rehabilitation access for pediatric cancer survivors (aged ≤19 years). This systematic review aimed to examine telehealth-based rehabilitation interventions aimed at preventing, maintaining, or improving disability in pediatric cancer survivors.
Methods:
We performed systematic searches in Ovid MEDLINE, Ovid EMBASE, Cochrane Library, SCOPUS, Web of Science, and CINAHL Plus between 1994 and 2022. Eligible studies included telehealth-based interventions assessing disability outcomes in pediatric cancers.
Results:
Database searches identified 4,040 records. Nine unique interventions met the eligibility criteria. Telehealth delivery methods included telephone (n = 6), email (n = 3), mobile health applications (n = 3), social media (n = 3), videoconferencing (n = 2), text messaging (n = 2), active video gaming (n = 2), and websites (n = 2). Interventions focused on physical activity (n = 8) or self-management (n = 1). Outcomes assessing disability varied (n = 6). Three studies reported statistically and clinically significant results. Narrative synthesis of findings was constructed based on the Picker's principles for patient-centered care: (1) values, preferences, and needs; (2) involve family and friends; (3) coordination of care; (4) provide social support; (5) holistic well-being; and (6) information and communication.
Conclusions:
Telehealth-based rehabilitation interventions for pediatric cancer survivors is an emerging research area with potential to improve disability outcomes. Adequately powered trials with consistency in disability outcome measures are warranted. Additional research is needed to determine the effectiveness and best practices for telehealth-based pediatric cancer rehabilitation.
Introduction
Survival rates for pediatric cancers (diagnosed age ≤19 years) continue to increase related to advancements in treatment, 1 as do the adverse late-effects which often sustain into adulthood, positioning survivors at increased risk for disability later in life. 2,3 As defined by the International Classification of Functioning, Disability, and Health (ICF) framework, activity limitations and participation restrictions are two aspects that make up cancer-related disability. 4 Pediatric populations diagnosed with cancer commonly experience activity limitations (e.g., activities of daily living [ADLs], gross motor performance, and physical activity) and participation restrictions (e.g., poor school performance, difficult social relationships) resultant from cancer diagnosis and treatment. 5,6 Pediatrics with cancer may also present with participation restrictions in the ability to successfully engage in society, such as impaired academic performance in school, socialization, sports performance, and interpersonal relationships and interactions, further affecting quality of life. 7
Cancer rehabilitation services and interventions have the potential to mitigate activity limitations and participation restrictions in pediatric populations. 5 However, access to cancer rehabilitation services is limited. For example, 76% of sampled hospitals and clinics affiliated with the Children's Oncology Group do not have an established pediatric oncology rehabilitation program. 8 While specifically unknown for pediatrics with cancer, disparities in access to physical rehabilitation for pediatrics with other health conditions include having Medicaid insurance and rural residence. 9,10 In a pediatric sample with acute lymphoblastic leukemia across 330 hospitals, only 27% of patients overall and 59% of patients with identified neuromuscular conditions received rehabilitation services within a year following their first hospital admission. 11 Taken together, these data suggest that many pediatrics with rehabilitation needs after cancer treatment do not receive these important services.
Telehealth delivery of rehabilitation interventions is an evolving model that may optimize health care delivery and improve access to rehabilitation services. Telehealth defined by the World Health Organization (WHO) is “the delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies, for the exchange of valid information for…treatment, and prevention of disease and injuries, [and] research and evaluation… in all the interests of advancing the health of individuals and their communities.” 12 Therefore, telehealth provides patients the opportunity to take part in real-time virtual consultation with health care practitioners, including rehabilitation professionals (e.g., physical therapy, occupational therapy, exercise physiology). Telehealth utilization has increased in recent years and been further expanded during the COVID-19 pandemic. 13 –15 Currently, little is known about the application and effectiveness of rehabilitation services delivered through telehealth for pediatric cancer survivors.
The primary aim of this systematic review was to identify and examine current cancer rehabilitation interventions delivered through telehealth aimed at preventing, maintaining, or restoring disability in pediatric cancer survivors. Second, we describe the intervention content and telehealth delivery methods, explicate effect of interventions on disability outcomes, and provide a framework for culturally competent patient-centered telehealth-based cancer rehabilitation interventions for consideration in future pediatric cancer telehealth intervention development, testing, and implementation.
Materials and Methods
An original systematic review by Brick et al. 16 assessed the effectiveness of telehealth-based cancer rehabilitation interventions for adult oncology populations. We sought to conduct a complimentary systematic review, synthesizing the existing literature for pediatric oncology populations. This work is warranted as pediatric oncology populations are compounded with unique developmental needs compared to adults.
ELIGIBILITY CRITERIA
We included randomized controlled trials (RCTs) and intervention studies with or without a control group that evaluated telehealth with a goal of preventing, maintaining, or improving disability in pediatric cancer survivors. Participants could be enrolled in the study with or without a caregiver(s) and could be at any point along the cancer care continuum, from diagnosis to end-of-life. Studies were included if they met the following criteria: (1) participants were diagnosed with a pediatric cancer as a child (aged 0–14 years) or adolescent (aged 15–19 years) 1,17 ; (2) participants were aged 0–19 at time of study enrollment 1 ; (3) intervention delivered according to the WHO definition of telehealth 12 ; (4) inclusion of at least one synchronous interaction or tailoring by a health care professional (to reflect current models of reimbursement for rehabilitation services); and (5) at least one measure of disability as a primary or secondary outcome.
For the purposes of this review, disability was representative of activity limitations, participation restrictions, or health-related quality of life that captured functional well-being. Studies that included any measure considered a proxy for participation such as community mobility or recreation and leisure activities were eligible.
We excluded studies with nonhuman subjects (e.g., animal models, in vitro), studies conducted before 1994 (due to significant changes in treatment protocols which have since increased survival rates 17 ; and advances in telehealth technology 14 ), non-English language publications, unpublished research, conference abstracts with no corresponding full-text publication, participant samples with mixed chronic health conditions (e.g., non-co-occurring cardiac disease, diabetes, and cancer), and noninterventional studies (e.g., cohort, observational, case–control, qualitative). Studies which exclusively enrolled participants aged greater than 19 years or did not stratify results by age classification, purely pharmacological interventions, studies including only psychosocial outcomes, and studies with outcome measures only assessing symptom severity were excluded. We identified and linked multiple reports of the same intervention and included reports detailing distinct findings and excluded if duplicated or irrelevant.
INFORMATION SOURCES AND SEARCH STRATEGY
We performed a comprehensive systematic search in Ovid MEDLINE, Ovid EMBASE, Cochrane Library, SCOPUS, Web of Science, and CINAHL Plus from inception to April 13, 2022. The initial search occurred on January 21, 2021, and to ensure that research recently published was included, an updated search was completed on April 13, 2022. Search structures, subject headings, and keywords were tailored to each database by a medical research librarian (K.J.K.) specializing in systematic reviews in consultation with coauthors. Searches were restricted to English-only articles. Searches were not otherwise restricted, including by study design. The complete MEDLINE and EMBASE search strategies are provided (Supplementary Table S1). The protocol for this review was not registered. Findings are reported in accordance with the PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analyses. 18
STUDY SELECTION AND DATA COLLECTION PROCESSES
Two investigators (M.B.S., S.J.W.) independently screened each of the titles and abstracts of the articles to identify potentially relevant studies using web-based systematic review management software. 19 Three investigators (M.B.S., S.J.W., and K.R.) independently screened titles and abstracts. Two investigators (M.B.S., S.J.W.) were the primary reviewers and supervised research interns during the data screening process so that each citation underwent an independent two-stage screening process. Studies that passed the title/abstract review were retrieved for full-text review by S.J.W. Disagreements at any stage were resolved by consensus and by seeking the opinion of an additional reviewer (M.C.S., V.M., K.R., or L.T.).
DATA EXTRACTION AND SYNTHESIS
Two coauthors (M.B.S., S.J.W.) extracted data from eligible studies pertaining to study design (i.e., sample size, primary and secondary endpoints, format, duration, dose, control condition), location of intervention, sample characteristics (i.e., cancer diagnosis, treatment history, sex, age, race/ethnicity), disability outcome measures, description of intervention components, adverse events, interventionist discipline, and telehealth delivery methods. Descriptive statistics was used to summarize intervention characteristics and calculate proportions. Raw means and standard deviations of disability measures were extracted when available to calculate between-group standardized effect sizes (Cohen's d) to determine clinical significance. 20
After full-text review, a meta-analysis was determined as inappropriate for evaluating the results of this systematic review due to the limited sample size and heterogeneity in disability outcome measures, population, and study and intervention design. Therefore, we used a narrative synthesis approach to coalesce intervention outcomes and guide the future development of telehealth-based pediatric cancer rehabilitation interventions, utilizing a conceptual framework 21 informed by nursing theory and the Picker principles of patient-centered care. The conceptual framework enumerates health care that is organized around the patient with partnership between the patient and family to identify and fulfill the full range of patient needs and preferences. 22,23 This approach was agreed upon by all authors before data extraction.
REPORTING RISK OF BIAS ASSESSMENT
Potential bias was evaluated using the Cochrane Risk of Bias for randomized trials version 2 (RoB-2) 24 for RCT or Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) 25 assessment tools for nonrandomized trials by two independent reviewers (M.B.S., S.J.W.). Any incongruence was resolved by discussion between M.B.S., S.J.W., and M.C.S.
Results
STUDY SELECTION
A total of 6,238 records were identified from databases of which 2,198 were duplicates; 4,040 were screened and 3,994 records were excluded by title and abstract screening. Bibliographies of relevant articles and systematic reviews were reviewed but yielded no additional records. One study was excluded due to insufficient reporting of outcome data, and the study authors were unable to provide these data upon request. 26 Interrater agreement averaged 98% (Cohen's kappa: 0.42). Following full text review (Fig. 1), 9 interventions with 10 published reports were included. 27 –36
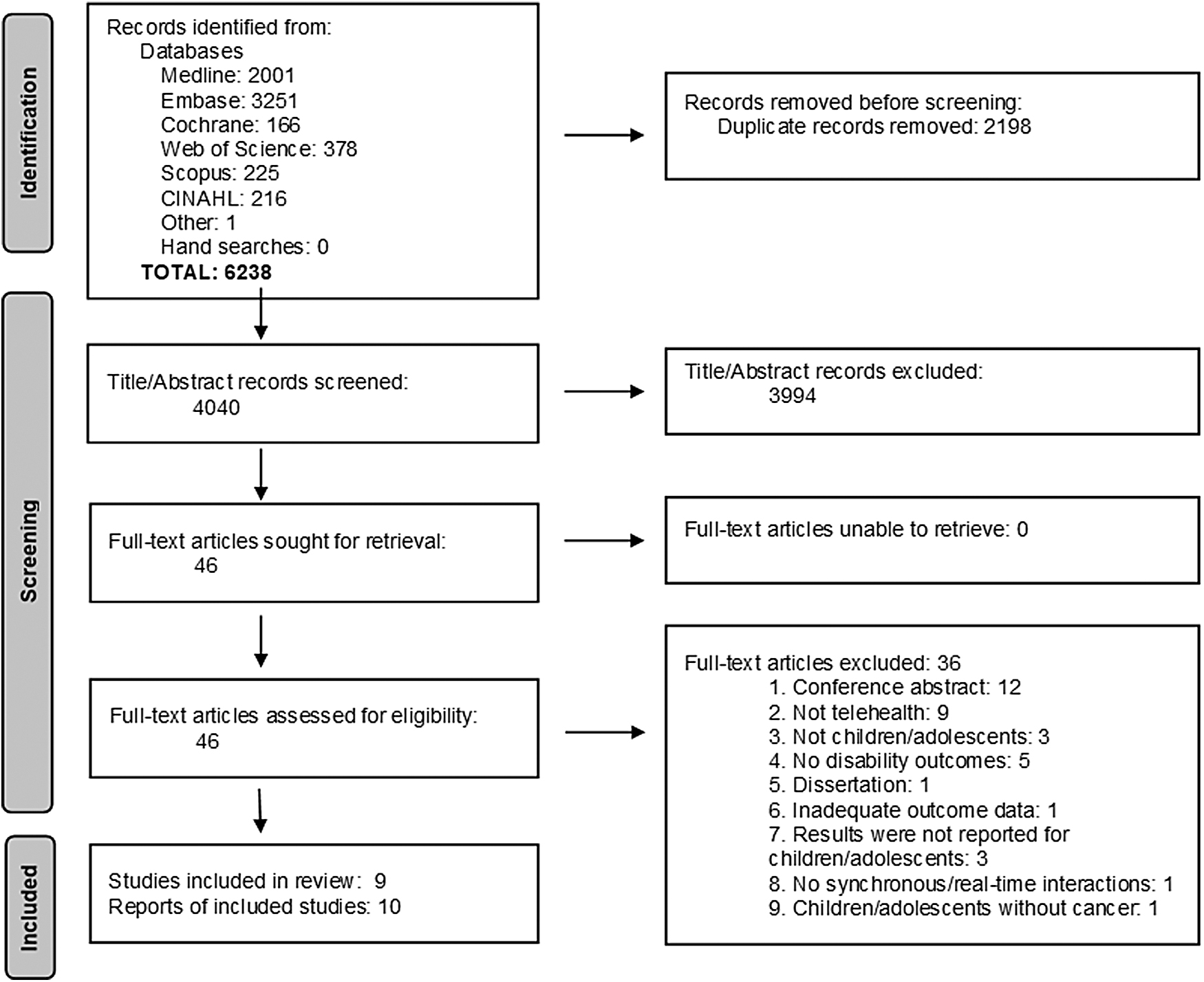
PRISMA 2020 Flow Diagram.
STUDY CHARACTERISTICS
Study sample and design
All eligible interventions were designed with the primary objective of assessing feasibility or change in disability (Table 1). Included studies were heterogenous in design, dose, duration, population, and outcome measures. Five studies used an RCT design, 27,29,31,34 –36 whereas four studies were single-arm observational pre- and post-test design. 28,30,32,33 Studies that included a control group used wait-list, 27,35,36 usual care, 29,34 and active 31 control interventions. Of note, Lambert et al., 33 reported using a single-arm quasi-intervention study utilizing a retrospective case–control design of healthy age- and sex-matched participants drawn from a database who had outcome measurements available at a single timepoint but were not enrolled in the intervention to demonstrate causality of intervention effect.
Characteristics of Eligible Telehealth-Based Pediatric Cancer Rehabilitation (n = 9): Intervention Design, Population, Outcomes, Relevant Findings, and Summary
Only reported for study completers.
RCT, randomized controlled trial; NR, not reported; SD, standard deviation; HRQOL, health-related quality of life; ADLs, activities of daily living; BMI, body mass index; BOT-2, Bruininks-Oseretsky Test of Motor Proficiency Version 2; IPAQ-SF, International Physical Activity Questionnaire Short Form; MABC-2, Movement Assessment Battery for Children Second Edition; PedsQL 4.0, Pediatric Quality of Life Inventory Generic Core; AMPS, Assessment of Motor and Process Skills; 6MWT, six-minute walk test; MVPA, moderate to vigorous physical activity; MET, metabolic equivalent; SMS, short messaging service; AVG, active video gaming.
Sample sizes ranged from 12 to 59 participants. Across all studies, participants (n = 281) average age was 13 years (SD: 0.9), and approximately half were male (51%). Blood cancers (i.e., leukemias and lymphomas) were the most prominent diagnosis. Eight studies tested rehabilitation interventions that emphasized physical activity promotion. 27 –31,33 –36 One study used principles of pain self-management to influence health related quality of life (HRQOL). 32
The interventions utilized a variety of telehealth delivery methods, including telephone (n = 6), 26,28 –32,34 email (n = 3), 30,32,33 mobile health applications (mHealth app; n = 3), 27,32,34 social media (n = 3), 27,31,34 videoconferencing (n = 2), 33,35,36 short messaging service (SMS) text messaging (n = 2), 31,34 active video gaming (AVG; n = 2), 29,35,36 and websites (n = 2). Interventions were delivered by registered nurses (n = 4), 28,30,32,35,36 physical therapists (n = 2), 28,29 an exercise physiologist or kinesiologist (n = 2), 28,33 certified trainers (n = 1), 27 health coach (n = 1), 31 or a research staff member with unspecified expertise (n = 1). 34 One intervention was implemented by multiple practitioners, including an exercise physiologist, physical therapist, and nurse, 28 while another stated that the intervention was implemented by either a physical therapist or nurse. 30
Intervention duration ranged from 22 days to 6 months. The average retention rate for the nine unique studies was 86%; studies with the greatest attrition included in-person supervised group exercise. 27,28 No adverse or serious events were reported. Two studies reported nonserious adverse events. For example, Esbenshade et al. 28 reported three nonserious adverse events possibly related to the intervention (i.e., minor cut, muscle strain, and dizziness). Similarly, Mendoza et al., 34 disclosed four mild adverse events related to falls or missteps occurring during exercise.
Disability outcome measures
Outcome measures that met our definition of disability included motor performance, ADLs, HRQOL, functional capacity, and community mobility (Table 2). Activity limitations in motor performance were objectively measured using the Bruininks-Oseretsky Test of Motor Proficiency™ Second Edition 37 (BOT™-2; n = 2) 28,36 and the Movement Assessment Battery for Children Second Edition 38 (MABC-2; n = 1). 29 Self-report and performance-based measures of activity limitations included the Pediatric Quality of Life Inventory™ Generic Core 39 (PedsQL 4.0™; n = 3) 27,32,34 to assess self-reported HRQOL and the Assessment of Motor and Process Skills 40 (AMPS; n = 1) 35 to objectively assess ADLs. Participation restriction was measured using the 6-min walk test 41 (6MWT; n = 1) 33 to objectively assess functional capacity in terms of community mobility. Step counts and moderate-to-vigorous physical activity minutes 42 (MVPA; n = 4) 27,30,31,34 were captured by self-report questionnaires or objectively by accelerometers to capture additional aspects of community mobility.
Summary of Disability Outcome Measures and Effect Sizes in Eligible Interventions
Defined by International Classification of Functioning, Disability and Health (ICF) Framework.
ADLs, activities of daily living; N/A, not applicable.
RESULTS OF INDIVIDUAL STUDIES AND SYNTHESIS
Disability outcome measure analysis
Jibb et al. 32 reported statistically significant improvements for HRQOL and clinically significant improvements in pain intensity (a proxy for pain interference associated with functional well-being); Sabel et al. 35,36 reported statistically and clinically significant improvement in motor performance postintervention. Of note, the improvement in these measures was generalized to age-expected values for independent living. Lambert et al., 33 reported within group statistical and clinical significance in median improvement of functional capacity among participants postintervention. However, the authors did not find between-group statistical or clinically meaningful differences. No statistically significant improvements in disability were reported for six studies. 27 –31,34
Effect size
Two studies reporting clinical significance favoring the intervention also reported within-group effect sizes for three disability outcomes. Sabel et al. 36 reported an effect size of 0.74 for change in AMPS Motor Score and 1.42 for AMPS Process Score, while Jibb et al. 32 reported an effect size of 0.42 for HRQOL based on the PedsQL 4.0. The reported effect sizes demonstrated small-medium magnitudes of effect. 20 Data were available to calculate between-group effect sizes from five studies for four measures (BOT-2, PedsQL, 6MWT, and MVPA) (Table 2). Calculated effect sizes ranged from 0.18 (small) for fine manual control to 0.95 (large) for manual coordination, both measured by BOT-2. 35
Risk of bias
Two studies indicated low risk of bias, 34 –36 three had moderate risk of bias, 27,31,32 and four had high risk of bias ( Fig. 2). 28 –30,33

Risk of Bias Assessment of Included Interventions using ROB-2 or ROBINS-I Criteria (n = 9). aRoB-2; bROBINS-1. RoB-2, Risk of Bias for randomized trials version 2; ROBINS-I, Risk of Bias in Nonrandomized Studies of Interventions; N/A, not applicable.
NARRATIVE SYNTHESIS: CONSIDERATIONS FOR CULTURALLY COMPETENT PATIENT-CENTERED TELEHEALTH INTERVENTIONS
Figure 3 presents a conceptual framework for culturally competent, patient-centered telehealth-based cancer rehabilitation interventions influencing cancer-related disability in pediatric oncology populations informed by nursing theory and the Picker principles of patient-centered care. 22,23 The resultant conceptual framework comprises six components: (1) values, preferences, and needs; (2) involvement of family and friends; (3) coordination of care; (4) provision of social support; (5) holistic well-being; and (6) information and communication. Due to the heterogeneity of the included studies, this conceptual framework was used to systematically evaluate and extract data from the interventions included in this review.

Considerations for Culturally Competent Patient-Centered Telehealth-Based Rehabilitation Interventions. Six identified components to prevent, maintain, or improve disability outcomes for pediatric cancer survivors. Determined by narrative synthesis and informed by the Picker Principles of Patient-Centered Care.
Values, preferences, and needs
Patient-centered care is defined as “providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions.” 43 Factors unique to individuals are associated with and may influence patient values, preferences, and needs which are instrumental for patient autonomy. 22,23 These patient level factors detailed in the eligible studies include cancer diagnosis, age, and culture which may be consequential to clinical trial participation, adherence, and retention. Included studies had a heterogeneous sample of pediatric patients ranging in clinical and sociodemographic characteristics. Known reasons for declining study participation included parents' overloaded schedules, current perceived activity level, and lack of interest. 28,30,32,33
While age was not associated with completion, 27 it is unknown how cancer type or age influenced enrollment rates. Age of the patient reflects the individual stage of development in cognitive, social, and emotional, speech and language, fine motor skill and gross motor skill development 44 which potentially impacts the patient's ability to fully participate in intervention components. One intervention used progressive resistance exercises, and intervention delivery was adapted and tailored for safety purposes. 33 Age was considered in two studies where physical activities were recommended based on age groups, 29,35,36 while other studies stratified randomization by age. 27,31 Participant's sex was considered as a potential confounder in one study, and analyses were adjusted accordingly. 34
Intervention materials were provided in languages other than English for four studies and included French, 33 Spanish, 31 Finnish, 29 and Swedish, 29,35,36 but it was unclear if interventions available in multiple languages were also culturally relevant. Supplies to fully participate in the intervention were provided by seven of the nine interventions and included exercise equipment, 28,33 Nintendo® Wii Fit™ AVG systems, 29,35,36 device with mHealth app installed, 32,34 software installation, 33 or a cellphone with data plan 31 ; however, associated costs remain undefined. Values, preferences, and needs of participants were not explicitly measured in any study. Future studies should consider formal assessment of values, preferences, and needs beyond demographics and clinical history.
Involve family and friends
The dimensions of involving family and friends include involvement in decision making, providing accommodations, providing support as caregivers, and recognizing the needs of the family and friends of the patient. 22,23 Pediatric patient experience can be influenced by the role of family and friends. 23,45 Family and friends were indirectly involved in the included studies. Parental informed consent and participant informed assent were required for all studies as participants included minors <18 years of age. Parents completed an activity diary and questionnaires as a proxy for children aged <10 years in one study. 29 Beyond this, involvement of family and friends was a common design element of four interventions, in which family and friends were not actual study participants but were tangent or delivered the intervention. 28 –31
The nature of a telehealth intervention requires parental supervision or permission. Parents were taught to use the FitBit® platform. 30 Often family members participated in the at-home exercises and engaging their parents and siblings encouraged participants, increased intervention adherence, and required less coaching follow-up. 28 Adherence was promoted in one study where families received an email to connect before every virtual exercise training session, and parents were encouraged to attend. 33 Some participants continued to engage with family and friends in the intervention activities after completion, 29 while some family members expressed aspirations to purchase their own FitBit. 30 Future telehealth interventions should be designed with consideration of the family and friends of the patient as a caregiver and additionally address their needs. 46
Coordination of care
Coordination of care includes integrating clinical care, frontline patient care, and ancillary and support services to increase self-determinism for the patient. 22,23 We were only able to extract limited information from the studies on how the telehealth rehabilitation interventions were implemented in the cancer treatment centers to suggest coordination of care. We found that the phase of the cancer continuum ranged from recently diagnosed 28 –30,32 through early post-treatment. 27,31,33 –36 Time since diagnosis and completion of treatment was not consistently reported, ranging from 1.5 to 9.5 years. 27,31 –33,35 Study participants were convenience samples recruited from affiliated cancer centers, and most studies had at least one intervention component delivered by a clinician. Health care professionals, rather than research staff, were often the interventionists. Only one study included a nutrition aspect where content was delivered by a health coach, not a Registered Dietitian. 31
All studies were multimodal, combining two or more delivery modes. Hybrid delivery, including both telehealth and in-person components, were provided by three interventions during inpatient hospitalization 29 or outpatient. 27,28 Telehealth interventions were supplemental to the standard of care being received; any external therapeutic modalities received by participants were not reported in any study. As a result, it is unclear how the telehealth interventions were integrated into the clinical workflow. It is possible that patients in the studies may have been receiving supportive care such as medical nutrition therapy, occupational therapy, or physical therapy during intervention participation. In future studies, it is important to state whether the telehealth interventions were integrated into the clinical workflow and how they were implemented. Furthermore, integrating health care providers and utilizing hybrid delivery models may enhance the delivery of telehealth rehabilitation delivery during pediatric survivorship care.
Provision of social support
Social support is a broad concept that refers to interpersonal relationships established with others and can be categorized as emotional, informational, instrumental, and appraisal types. 22,47 Social support was integrated into five trials primarily through health behavior theoretical framework or assessment. 27,31 –34
The FitSurvivor study utilized a variety of behavior change techniques from Social Cognitive Theory, including goal setting, self-monitoring, reinforcement, and behavioral substitution. 27 The Fit4Life study also drew from Social Cognitive Theory in the design of their weight management intervention, using techniques such as social support through health coaches and self-monitoring. 31 Mendoza et al., 34 used Social Determination Theory, aiming to increase autonomy and competence through participants setting their own step goals and tracking their progress. Gamification, the use of game design elements in nongame contexts to increase motivation and engagement, 48 was present in mHealth apps and included unlocking achievements and badges 27,34 and points and reward systems. 27,32 Additional social support was provided through optional moderated online peer support groups to increase connection and establish a sense of community; however, engagement was limited and study findings favored the control group. 27,34
Most studies included informational and instrumental social support with little emotional and appraisal social support provided. All studies lacked comprehensive reporting on how the social support construct was changed because of the intervention. Moreover, none of the studies analyzed the impact of social support as a mediator of intervention effectiveness. Providing elements comprising the four types of social support in intervention design and delivery and formal assessment should be regarded in forthcoming interventions to provide meaningful patient-centered telehealth rehabilitation for pediatric cancer survivors. 45
Holistic well-being
Holistic well-being encompasses body, mind, social, and spiritual elements of humanity. 49 Included studies were considered holistic in various forms of supportive cancer care, including psychosocial, synergistic health behaviors and symptom management. Interventions often included additional education on issues unique to survivorship 27,31,32 because they have major impact on activity and participation 4 especially among pediatrics. 50 Huang et al. 31 measured change in depressive symptoms in participants in Fit4Life and indicated that the intervention had a significant effect on improving depressive symptoms of negative mood. Sabel et al. 36 measured the effect of AVG on cognition, but there was no statistically significant change in cognition after the intervention period, with improving trends observed for sustained and selective attention. Fatigue was measured in three studies, but fatigue did not significantly change because of participation. 27,29,30 Pain was measured by Jibb et al. 32 where postintervention, significant improvement in pain intensity and nonsignificant reduction in pain interference were observed. While pain was not an outcome in the study by Lambert et al. 33 pain was assessed on a Likert scale at the beginning and end of each supervised exercise session with adaptations personalized according to location and intensity of the pain.
Fit4Life promoted healthy weight among survivors of cancer by combining physical activity (i.e., daily step goal) with nutrition (i.e., calorie reduction, portion control) which are synergistic health behaviors for energy balance; however, there was no significant intervention effect on daily calorie intake. 31 No other intervention included additional health behaviors. Body mass index (BMI) was assessed in three studies 28,30,31 where two interventions had nonsignificant reductions in BMI z-scores. 28,31 Amalgamating rehabilitation with supportive cancer care that addresses patient basic needs can promote holistic well-being and self-care for pediatric populations in future telehealth interventions. 22
Information and communication
Patient education, including information and communication, that is understandable and detailed on clinical status, progress, processes of care, and prognosis, can facilitate independence and promote health. 22,23 The type of information shared and the communication format varied across interventions, including traditional and digital channels.
Web-based information (i.e., website or email) and supplementary printed materials were used for primary information sharing. 27 –36 One study promoted families selecting their preferred technology to interact with the interventionists (i.e., tablet, desktop computer, or smartphone) providing participants access to the intervention outside their home. 33 Health coaches and clinicians provided verbal information either face-to-face or virtually (with or without video). An activity tracker (i.e., FitBit) or other wearables (i.e., accelerometer) providing information on activity were included as part of the intervention 30,33,34 or as an assessment method. 27,29,31,34 –36 Many participants found their individual physical activity data helpful. Reported adherence to activity tracker wear criteria established by studies ranged from 71% to 94%. 30,33,34 While wearables were well accepted and useful for sharing motivational and goal setting messages among participants, nonwear reasons included leaving it at home, technical issues, and battery life. 30,33,34 SMS text messaging was tailored for interventions 31,34 ; however, SMS use was more prevalent among older children. 31
Use of a mHealth app provided encouragement, motivation, education, and social enjoyment for participants yet technical aspects and functional features of the mHealth app had room for improvement. 27 Social media acted as a facilitator and barrier for communication between providers, participants, and peers. 27 Social media was considered a good forum for participants to check-in with one another, but participants reported a desire to have more frequent interactions on social media (e.g., Facebook, Snapchat, or Instagram). 34 Younger participants may not actively participate in social media, have parental permission, or meet the minimum age requirement for platforms; a reason for nonparticipation. 27 Information and communication through various medium in telehealth rehabilitation interventions can improve the pediatric patient transition through the cancer continuum and enable self-management. 51
Discussion
This systematic review provides an overview of the current science of telehealth-based rehabilitation interventions to prevent, manage, or improve disability among pediatric cancer survivors. The nine unique interventions included design components of promoting physical activity or self-management and were hybrid or multimodal while having at least one synchronous interaction between participants and health care providers. Our narrative synthesis of interventions points to six considerations for future interventions to deliver culturally competent and patient-centered cancer rehabilitation to pediatrics. Overall, our systematic review identified trends toward improved disability in pediatrics with cancer that utilized telehealth for rehabilitation, despite variance in measures and significance. Our results suggest that telehealth rehabilitation has potential to improve disability outcomes in the dimensions of impairment and activity limitation for pediatric cancer survivors, while effects on participation are less clear.
Our findings are similar to those of Brick et al. 16 who concluded that telehealth-based rehabilitation interventions for adults were primarily delivered post-treatment, one-on-one, and through telephone with heterogeneity in disability outcome measures among adult survivors of cancer. Another systematic review of 362 interventions by Sleight et al. 52 supported rehabilitation interventions as efficacious on nine domains of functioning for individuals with cancer; however, intervention designs varied, and telehealth was not specifically addressed. Both systematic reviews excluded studies with participants <18 years of age, a common exclusion criterion as interventions designed for adult survivors of cancer do not necessarily translate well into pediatric populations.
Most studies included in our review promoted physical activity, while only one study had an integrated nutrition component. A recent systematic review of eight exercise RCTs found improvement in function among pediatrics with cancer 53 ; however, other rehabilitation modalities, delivery methods, or disability outcomes of activity limitation and participation restriction were not measured. Nutritional status, meal engagement, or feeding was not captured in any study included in this review yet feeding and eating are essential occupations for pediatric populations. 54,55 Our separate review highlights the paucity of medical nutrition therapy interventions as part of the telehealth-based cancer rehabilitation interventions.
Our conceptual framework and narrative synthesis provides considerations for culturally competent patient-centered care in telehealth rehabilitation intervention design. This framework can inform the development of future telehealth rehabilitation interventions for pediatric cancer populations. Consistent with the ICF framework, external contextual factors and environment should also be considered. Such factors include social determinants of health, 56 which have been associated with pediatric cancer survival and health outcomes. 57,58 Access to adequate cancer care, including rehabilitation, may be resultant of health disparities related to these determinants. 59 Complementary frameworks exist to better understand the complexities of health disparities 60 while behavioral theories can assist in identifying which intervention strategies may be effective. 61 Therefore, integration of multiple theories and frameworks and applying multilevel intervention design principles may expand reach of telehealth rehabilitation to pediatrics in various phases of the cancer continuum.
STRENGTHS AND LIMITATIONS
This study represents current telehealth-based cancer rehabilitation interventions aimed at improving disability outcomes for pediatric cancer survivors. However, there are limitations to our findings. Participants in all studies had the ability to ambulate independently and maintain balance control, potentially biasing intervention effects in a more robust sample. Such inclusion criteria may limit generalizability to pediatric oncology populations with physical limitations resultant of cancer-related treatment. The measures of disability included both self-report, performance-based, and objective measures leading to additional variation. The variety in measurement points to the need for consensus in clinical and research measures to detect efficacy of interventions in this population. 16,52
Studies reported limited recruitment and inclusion of minority populations, limiting generalizability to underserved or historically marginalized population who often have limited accessibility to cancer rehabilitation interventions. 10 To deliver equitable care, cancer rehabilitation interventions must focus recruitment efforts to broader population groups. The published data did not allow for us to identify how time since diagnoses may be related to telehealth use. Future work may consider the context of time since diagnosis in the access and delivery of telehealth-based services.
We conducted the review using rigorous methods, but publication bias is always possible. Included studies were limited to articles published in peer-reviewed journals in the English language, potentially creating an upward publication bias and limiting the generalizability of the findings.
Study quality was not an eligibility criterion; therefore, some interventions presented with high risk of bias. To ensure a comprehensive overview of the state of the science in telehealth-based cancer rehabilitation interventions in pediatric oncology populations, we wanted to include those with high risk to demonstrate the breadth of intervention research. Our updated search did not yield any studies that took place during or referenced the COVID-19 pandemic. In response to COVID-19, pediatric rehabilitation interventions may have been adapted to telehealth 15 and were not captured in this systematic review due to latency of publishing full reports. Special attention to pre-, during-, and post- COVID-19 telehealth-based rehabilitation interventions is warranted, as interventions adapted to telehealth in response to COVID-19 compared to those inherently intended as telehealth by virtue of design may differ in terms of reach, disability outcome measures, and technology utilization. Such information will have lasting influence on policy related to telehealth reimbursement and access.
Conclusions
Pediatric cancer survivors are a growing population with unique needs who experience increased burden from cancer-related disability 62 hastening the prerequisite of increasing access to rehabilitation as part of cancer care through telehealth, which currently is still emerging. Future research is needed to evaluate telehealth rehabilitation interventions to also consider cost effectiveness and integration of a multidisciplinary clinical care team to improve disability outcomes. We recommend future telehealth-based rehabilitation interventions for pediatric cancer survivors to consider six factors: (1) values, preferences, and needs; (2) involve family and friends; (3) coordination of care; (4) provide social support; (5) holistic well-being; and (6) information and communication. High quality multimodal studies, including RCTs powered for activity and participation outcomes, are warranted. Future research on telehealth-based cancer rehabilitation interventions in this population should examine most effective combinations of components which will ultimately impact implementation, reimbursement, and sustainability of this supportive care service for pediatric cancer survivors.
Footnotes
Acknowledgments
This work was supported by members of the Outcomes and Research task Force of the Cancer Rehabilitation Networking Group of the American Congress of Rehabilitation Medicine. The authors acknowledge Kathleen D. Lyons, ScD, OTR/L for her consultation on study design and search strategy development. Access to electronic databases was made available by the University of Texas MD Anderson Cancer Center Library and the University of Arizona Health Sciences Library. The authors thank the student research interns who assisted M.B.S. and S.J.W. with supervised title and abstract screening: Alana Miller, Jiamin Yan, Sofia Malvaez, and Reina Sandoval. Portions of these data will be presented in symposia at the 2022 American Congress of Rehabilitation Medicine Conference. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Institutes of Health.
Authors' Contribution
Conceptualization, M.B.S., S.J.W., R.S.B., L.T., K.R., V.M., N.K., D.R., K.T., K.J.K., M.C.S.; literature searches, K.J.K. and M.C.S.; validation, M.B.S., S.J.W., R.S.B., L.T., K.R., V.M., N.K., D.R., K.T.; data screening, M.B.S., S.J.W., K.R., V.M., L.T., M.C.S.; data extraction, M.B.S. and S.J.W.; data analysis and interpretation, M.B.S., S.J.W., and M.C.S.; writing—original draft preparation, M.B.S., S.J.W., and M.C.S.; writing—review and editing, R.S.B., L.T., K.R., V.M., N.K., D.R., K.T., and K.J.K.; supervision, M.C.S.; project administration, M.B.S. and S.J.W. All authors have read and agreed to the published version of the article.
Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This research received no external funding. Additional salary support was provided by MD Anderson's Cancer Center Support Grant (CA016672).
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.