
Abstract
Introduction:
Clinical Pharmacist-led Comprehensive Medication Management (CMM) has the potential to mitigate medication errors during transitions in care, but current evidence is underdeveloped. The objective of this work was to assess the impact of optimized CMM services through a telehealth pharmacist clinic on hospital readmission and Emergency Department (ED) utilization rates.
Methods:
A quality improvement study with patients discharged home from an urban, nonacademic Hospital in Westchester County, New York, receiving telehealth CMM was used. Participants included adult patients discharged home from an internal medicine unit considered high risk for preventable adverse medication errors based on comorbidities and prescribed medications. Eligible patients were offered to enroll in telehealth CMM visits with a clinical pharmacist immediately, 30 days, and 60 days post-discharge versus the current standard of care.
Results:
Primary outcomes included the impact on 30- and 90-day readmission and ED visit rates. Secondary outcomes included quantifying the outcomes on patient engagement, enrollment, and volume resulting from the program's process improvements. In this study, 3,060 patients were discharged from June 14, 2021, to May 10, 2022; 1,547 were eligible and offered CMM visits, and 889 completed enrollment (Treated). There was a 2.1% absolute difference in 30-day readmission rates between untreated and attempted (p = 0.07), and a 2.9% difference between the untreated and treated group (p = 0.04). Thirty-day ED utilization decreased by 1.6% between untreated and attempted (p = 0.3), and 3.5% between the untreated and treated (p = 0.03). There were four Plan-Do-Study-Act cycles in this program, in which the process improvements resulted in an overall average increase in patient volume, enrollment rates, and patient engagement for this QI initiative.
Conclusions:
This study yielded significant reductions in readmission and ED utilization rates among treated patients, highlighting successful process improvements that improved patient engagement and the potential for enhancing care coordination in vulnerable populations.
Introduction
“Transition of care” encompasses a patient's movement between services, providers, or health care systems, representing potential weak points in the continuity of care. A notable transition of care is discharging a patient from the hospital, with studies reporting 20% of patients experiencing an adverse event resulting in injury from medical management, 1,2 66% of which are adverse drug events (ADE). 2 A systematic review determined 50% of patients experience a medical error at discharge. 3 A 2018 study used three different regression models to assess the cost expenditure of 196,600 ADEs, projecting a total cost between $871 million and $1.8 billion for treating preventable ADEs. 4 With the aging population of the United States, 5 and the rising use of pharmaceuticals and polypharmacy 6 resulting in an increased incidence of hospitalization, outpatient care visits, and health care costs, 7 it is imperative to continue to investigate practices improving outcomes for discharged patients.
Comprehensive medication management (CMM) integrates clinical pharmacists in a patient-facing role to assess the efficacy, safety, and feasibility of prescription and nonprescription medication regimens. 8 Currently, CMM models implemented in individual health care systems across the United States show improved medication outcomes, reduction of readmission, cost savings, and improved patient and provider satisfaction. 9 –11 Recently, CMM models integrated telehealth, 12,13 demonstrating initial success managing medications in rural and developing communities, and increased growth in accessible areas due to the COVID-19 pandemic. 14 Many clinical pharmacy publications to date were multifaceted interventions with results that confound the results of telehealth clinical pharmacist services with other telehealth services. 15 Previous studies that have the sole intervention of virtual pharmacist services describe this model, but do not quantify the impact post-implementation. 16 There is a need to assess structured telehealth clinical pharmacist CMM programs' impacts on accessible areas.
Before the initiation of this program, our hospital identified medication-related issues as a potential source of preventable hospital readmission and utilization of acute care services based on individual case reviews. However, given that this occurred after discharge, the true extent of this was not fully known. In 2020, we were either at goal or above goal in our readmission targets, primarily for all-cause readmissions, heart failure (HF), chronic obstructive pulmonary disease (COPD), and pneumonia (PNA) discharges.
In this quality improvement (QI) initiative at a single-site institution, the authors wanted to best optimize CMM in a high-risk population with a focus on decreasing hospital readmission rates and subsequent ED visits post-hospitalization. This article highlights the implementation steps and process measures put into place at this single center to optimize a CMM-based program. The smart aim for this project was to decrease all-cause readmissions through a CMM Program from 10.3% in 2020 to 9.5% by 2021.
Methods
This was a single-center QI initiative at White Plains Hospital, a 292-bed community hospital in Westchester County, New York. The program was initiated through the White Plains Hospital Cares (“WPH Cares”) program, a department that originated in 2018 as a telehealth transition of care platform for all discharged patients. The WPH Cares team includes Registered Nurses (RNs), Social Workers (SWs), Physician Navigators (PNs), and Advanced Practice Providers (APPs) and is overseen by a Medical Director.
The clinical pharmacist's impact on this QI initiative was implemented through Cureatr Clinic (New York, NY), a national data-driven telehealth medication management clinic powered by Cureatr Clinical Pharmacists (CCP). The CCPs had 1–2 years of pharmacy residency training or equivalent direct patient care experience and performed all CMMs on patients. At the time of initiation of the study, the 2020 all-cause readmission rate for Medicare patients was 12%, 16.7% for HF, 15.9% for COPD, and 15% for PNA.
This report describes in detail the QI intervention and integration, abiding by the reporting guidelines suggested by the Standards for Quality Improvement Reporting Excellence (SQUIRE 2.0) guidelines and leveraged 17 the Model for Improvement by the Institute of Health care Improvement. This model highlights the Plan-Do-Study-Act (PDSA) cycle, one of the most well-known, experience-based learning models in health care for QI. 18 This report reveals the first five cycles of this initiative.
Intervention
Inclusion criteria were 18 years of age or older, admitted to an internal medicine unit, and considered high risk for preventable adverse medication errors based on specific discharge disease state diagnoses, elevated LACE+ scores, and being discharged on 1 high-risk medication or 5+ medications. Early PDSA cycles focused on patients with a discharge diagnosis of Acute Decompensated Congestive HF, COPD, and PNA.
In later PDSA cycles, the inclusion criteria expanded to patients with an elevated LACE+ index (Length of stay, Acuity, Comorbidities, and Emergency Room visit), five scheduled prescription medications, or discharged on at least one high-risk medication, classified as (1) anticoagulants, (2) antiplatelets, (3) hypoglycemic agents, (3) immunosuppressants, or (4) anti-infectives, following a prior telehealth pharmacist service study. 19 Enrollment occurred between June 14, 2021, and May 10, 2022. Exclusion criteria included the following: no personal phone number, palliative care or hospice, or discharge to a subacute rehabilitation facility, group home, long-term acute care, or skilled nursing facility.
Data collected by Cureatr included the patient's medication list at the time of discharge, reconciled medication list completed by Cureatr Clinic Support Staff (CCSS), pharmacist interventions, provider recommendations, and admission, discharge, and transfer (ADT) status records. The patient's date of birth, gender, race, and prior disease status were collected from the White Plains Hospital electronic medical record (EMR) data.
A summary of the PDSA cycles is listed in Table 1. In PDSA 1 (May– June 2021), the authors designed a protocol that would start with a smaller subset of the population limited to patients with discharge diagnoses of HF, COPD, and PNA. To measure the impact and changes necessary to strengthen the program, they reviewed process measures focused on outcomes including acute care visits after hospitalization, patient enrollment in the program, and measurable provider engagement as the program began to centralize and engage the ambulatory physicians. Key stakeholders included inpatient hospitalists, including the director who worked with the Cureatr Clinic leadership to build out escalation pathways for the treated population, hospital RNs in the outreach department, and clinical pharmacists involved in the planning and implementation. Throughout the program, the Cureatr messaging application was leveraged by ambulatory physicians.
Plan-Do-Study-Act Cycles with Correlating Improvements
HF, heart failure; COPD, chronic obstructive pulmonary disease.
Patients with multiple discharges during the study period were removed from eligibility into the program after their first discharge. The attempted group includes all patients the CCSS tried to contact, but not all were reached or treated. The results section includes statistics comparing the untreated versus attempted group, in addition to the untreated versus reached group.
For the implementation stage (PDSA 1), patients received a one-time telehealth outreach by an RN for follow-up care, discharge instructions review, and access to medication assessment. Furthermore, patients diagnosed with HF, COPD, or PNA receive additional services, such as weekly follow-ups with an APP for 4 weeks, with some patients receiving remote patient monitoring, community paramedicine, or visiting nurse services based on their clinical requirements.
The virtual clinic consisted of roughly 12 CCSS and 8 CCPs to complete the volume of this study. The CCSS completed pre-visits with study participants, which included the creation of medication lists and the identification of concerns to be addressed during the Cureatr Clinical Pharmacists (CCP) consultation. Urgent concerns were triaged to the CCP immediately. Both the CCSS and CCPs utilized Cureatr's proprietary, Meds360° platform, which allowed for real-time access to roughly 80–85% of payor data through real-time PBM claims, pharmacy point-of-sale data, and ADT feeds. In addition, the CCSS and CCPs had read-only access to WPH's EMR system to complete the pre-visit and CMM, respectively. The CCPs were compensated for providing CCM visits.
Participants who were successfully reached by telephone underwent an initial CMM visit and scheduled 30- and 60-day follow-up visits. The initial and follow-up visit interventions were all telephonic visits. The attrition rates for the study can be found in Supplementary Table S1. Each CMM visit consisted of discharge medication reconciliation and disease state counseling.
The CCP tailored the CMM to each patient, focusing on barriers to adherence and medication access, disease state counseling, medication cost, patient concerns, goals of therapy, medication administration, self-care, coordination of care, and social work issues. Furthermore, the CCP created a medication action plan (MAP) that was emailed or mailed to the patient and faxed to the primary care provider and specialists after the appointment. The MAP was faxed using a website that would detect failures, ensuring the CCSS would get notification of any send failures and prompt action to investigate the case until it is sent successfully.
The MAP included the reconciled medication list, along with detailed recommendations for both the patient and provider. Patient recommendations were presented in a summary format, highlighting key counseling points, instructions, and follow-up guidance. Provider recommendations were classified as medication optimization, consisting of dosage adjustments, unnecessary and suboptimal interventions, and access issues, or medication safety, consisting of adverse events, interactions, duplications, overutilization, and duration issues. Each patient had a MAP sent to their provider on their behalf explaining the different medication recommendations the CCP found; however, when medication safety issues arose, the CCP called the provider's office to report the recommendation verbally, in addition to the office receiving the recommendation by fax. The full CCP escalation pathway can be found in the Supplementary Table S1.
The second PDSA cycle took place over the course of July and August 2021. During this time, it became apparent that the program was experiencing low enrollment rates, which stood at 32%. In response, the program enlisted the support of Cureatr Clinic, which assumed responsibility for patient enrollment. This involved conducting phone calls, text messages, and email outreach to encourage patients to participate in the program. Moreover, the team identified inaccuracies in the reporting of patient data, specifically in the inclusion of patients with a history of HF, COPD, or PNA without a recent acute exacerbation. As a result, the team collaborated with departments outside of Internal Medicine, including Surgery, to address these inaccuracies and ensure the accurate reporting of patient data.
The third PDSA cycle took place from September through October 2021. To continuously support ambulatory physicians, the team set up focus groups to gather feedback and insights from these health care providers.
The insights gained from these focus groups were used to make several key adjustments to the program, including changing the MAPs based on physician preference. Specifically, medication recommendations were grouped by a physician, and provider recommendations were moved to the top of the documentation, as opposed to being placed at the end. These changes aimed to make the MAPs more accessible and user-friendly for physicians and improve the likelihood of adherence to treatment plans. In addition, during this cycle, the program scaled up from focusing solely on patients with HF, COPD, and PNA, to all discharges with an elevated LACE+ score and who were on five or more medications, based on the inclusion criteria previously discussed. These changes reflect the program's commitment to continuously evaluating and improving its services and providing the best possible care to all eligible patients.
The fourth PDSA focused on revisiting escalation pathways with the inpatient teams, driven by concerns about the frequency of escalations. As a result of this evaluation, the team added more structure to the boundary between inpatient and ambulatory physicians, clarifying the circumstances under which escalation to either team was appropriate.
In addition to this, the team developed a social work pathway in response to a high number of social escalations. This development aims to ensure that patients receive the most appropriate care and support, with social work specialists providing valuable insights and interventions for patients with complex social needs. These changes reflect the program's commitment to continuously improving the care and support provided to patients, by refining and strengthening the escalation pathways in response to feedback and evaluation. The development of a social work pathway reflects the program's dedication to holistic patient care, addressing the unique needs and challenges of each patient to support their overall well-being.
Study of interventions
In the “Study” phase of the PDSA cycle, the WPH Cares and Cureatr Clinic leadership team convened monthly to review process measures and determine the need for adjustments based on (1) outcome measures and the expansion of services to other high-risk populations, (2) patient engagement and enrollment in services, and (3) provider feedback on the program's recommendations.
To comprehensively evaluate the intervention's impact, patients were randomly selected for enrollment based on their initial diagnosis of HF, COPD, or PNA. In subsequent PDSA cycles, the program was scaled up to include patients with an elevated readmission score (LACE+), discharged on 5+ medications, or discharged on 1+ high-risk medication(s). Due to similar disease states being present in each unit, patients could not be divided based on unit, prompting WPH Cares to enroll even-numbered patients into the CMM program, in addition to their current transitional care work, while odd-numbered patients continued to receive the WPH transitional care outreach by hospital RNs. This design allowed the use of run charts to assess the intervention's impact and to compare the population that received the intervention with the population that did not, thereby further illuminating the intervention's effectiveness.
Key process measures monitored included (1) 30- and 90-day readmission rates, (2) 30- and 90-day ED utilization rates, (3) enrollment rates, and (4) volume of cases per month rate. The first two measures were compared between the untreated and both the attempted and treated groups, including analyzing any difference between baseline demographics and clinical factors. Also, subgroup analyses were performed for patients with a diagnosis history of HF, COPD, or PNA, in addition to any patient discharged on 7+ medications or 3+ high-risk medications.
Measures
The primary endpoint of interest in this study was the effect of the program on 30-day hospital readmissions and acute care visits. This was assessed by examining a run chart of all-payer readmissions monthly. In addition, to stratify the population based on participation in the intervention, we conducted a regression analysis comparing those who received the program to those who were eligible, but did not enroll, as well as those who were screened out of the program.
The secondary outcomes measured included (1) patient enrollment to assess the rates of participation based on the patients who were reached through phone, (2) patient satisfaction with the services they received through a survey, and (3) development of a provider engagement platform to assess their willingness to accept recommendations for mutual patients.
Analysis
Before the development of the program, the authors developed a Directed Acyclic Graph (DAG) relevant to potential confounders for 30-day readmission. Key categories included socioeconomic factors (Insurance, Zip Code, Race, and Ethnicity) and baseline health indicators (gender, age, chronic medical conditions, and Charlson comorbidity index) with the severity of disease (length of stay and ICU admission). After demographic information was collected, patient groups were tested across age, gender, race, and ethnicity, as well as DAG baseline health indicators. Each variable in the DAG, excluding zip code and CCI, was tested across the untreated, attempted, and treated groups using a chi-square test of independence to evaluate differences among populations shown in Table 2.
Directed Acyclic Graph Variable Tests
LOS, length of stay; PNA, pneumonia; AMI, acute myocardial infarction.
Patients were assigned a binary indicator of readmission based on the presence or absence of one or more acute inpatient readmission events during the 30- or 90-day period following the initial discharge. All future admissions were assigned to that patient and the patient status (attempted/untreated) was unchanged based on any following admission. Similarly, a binary indicator was used to flag the presence or absence of one or more ED visit events during the 30- or 90-day period following the initial discharge. This study also applied a Poisson regression model for readmission counts per patient to determine the impact of multiple readmissions.
Ethical considerations
This study has been reviewed and determined as exempt by the Institutional Review Board (IRB) of White Plains Hospital.
Results
From June 2021 to May 2022, our program ran four PDSA cycles. Results include 3,060 patients with a mean age of 68.4 years, 50.7% female, and 60.7% white. Of these, 1,513 are included in the untreated group, 1,547 in the attempted group, and 889 in the treated group, shown in Figure 1. The full demographics and characteristics of the study population are listed in Table 3.
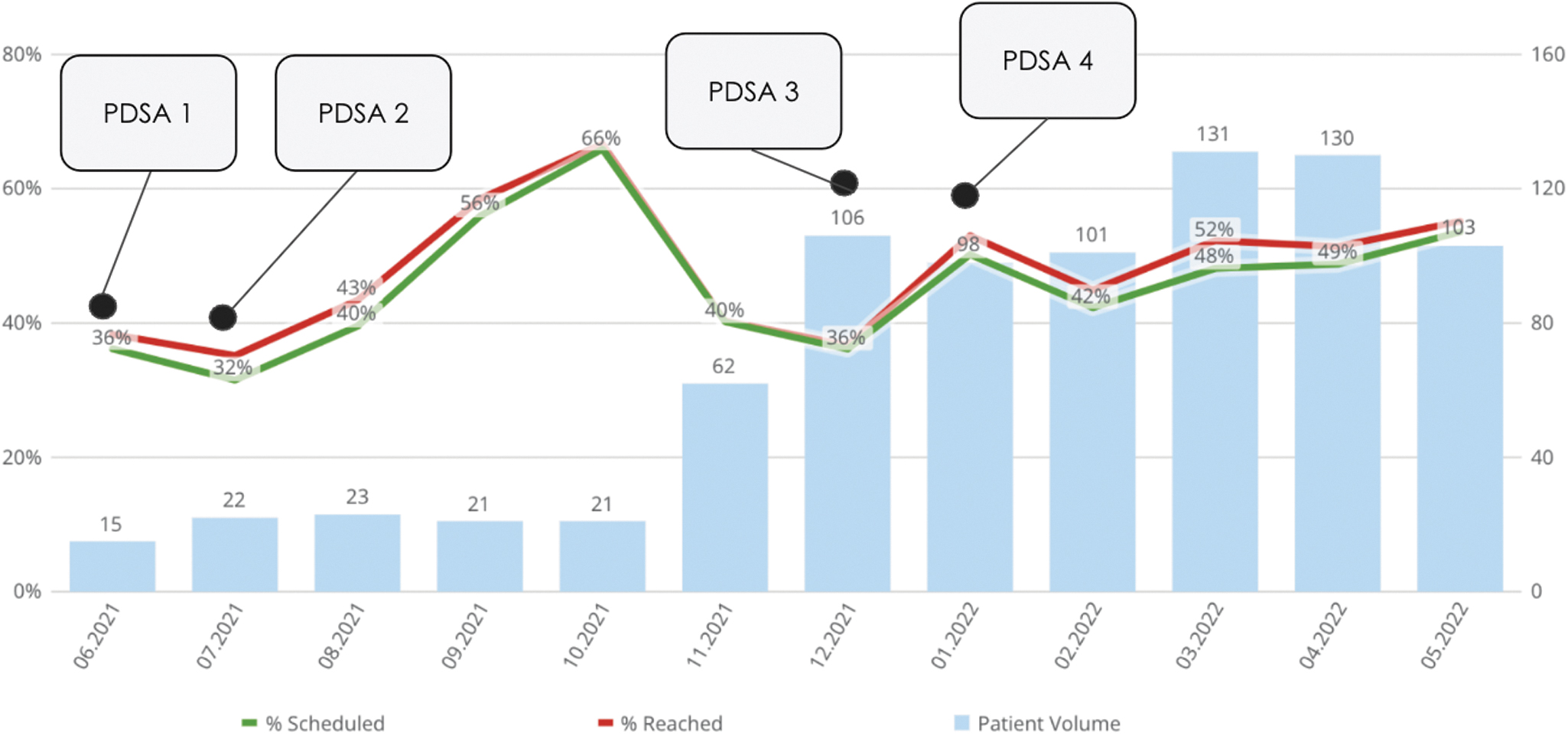
Run Chart.
Study Population Demographics
In order of frequency, the most common causes of initial admissions were (untreated and attempted) sepsis (13.1% and 12.7%), HF (5.2% and 5.1%), and acute myocardial infarction (AMI) (4.3% and 5.8%). The most frequent causes of readmissions (untreated and attempted) included sepsis (14.7% and 19.6%), PNA (5.1% and 2.4%), and diabetes (2.5% and 4.8%). There were 197 untreated patients, 13% of the untreated cohort, readmitted within 30 days with 34 (17.3%) having 2 or more readmissions, compared to 168 attempted patients, 11% of the attempted cohort, readmitted within 30 days with 18 (10.7%) having 2 or more readmissions. Poisson regression results testing readmission count did not produce significant variance (p = 0.6).
No statistically significant difference was found in mean length of stay, mean days in the ICU, mean health literacy score, count of prescription medications at discharge, or count of high-risk medications at discharge between the untreated vs attempted or untreated vs. treated groups. Finally, the condition profile of untreated and attempted samples was examined. The randomization resulted in an even balance between untreated and attempted for patients identified with HF, COPD, PNA, and AMI. To evaluate the impact of Cureatr Clinic services, additional analysis was performed on the highest-risk population, HF patients. Using a chi-square, the randomization of untreated, attempted, and treated groups across age, gender, race, ethnicity, average health literacy score, number of prescription medications at discharge, and diagnosis variances was tested and was found to be due to randomness and is not statistically significant.
When observing the primary outcomes of the study, there was a 2.1% absolute difference between the percent readmitted within 30 days post-discharge from the untreated group (13%) and the attempted group (10.9%) (p = 0.07), with a 2.9% absolute difference between the untreated group (13%) and treatment group (10.1%) (p = 0.04). In addition, 90-day readmission rates decreased by 3.1% between the untreated group (24.6%) and the attempted group (21.5%) (p = 0.04) and by 3% between the untreated group (24.6%) and the treatment group (21.6%) (p = 0.1).
Thirty-day ED utilization had an absolute reduction of 1.6% between the untreated group (18.7%) and attempted group (17.1%) (p = 0.3), and 3.5% between the untreated (18.7%) and treated group (15.2%) (p = 0.03). Ninety-day ED utilization has an absolute reduction of 1.5% between the untreated group (32.5%) and the attempted group (31%) (p = 0.4), and a 2.7% decrease between the untreated group (32.5%) and the treated group (29.8%) (p = 0.2).
Participants with 7+ prescription medications saw a decrease of 3.6% in 30-day readmission rates between the untreated (15.4%) and attempted group (11.8%) (p = 0.03) and a decrease of 3.8% when comparing the untreated (15.4%) to the treated group (11.6%) (p = 0.05). In addition, a decrease of 5.1% was shown in 90-day readmission rates between the untreated (29.2%) and attempted group (24.1%) (p = 0.02) and a decrease of 3.8% when the untreated (29.2%) was compared to the treated group (25.4%) (p = 0.1).
The largest subgroup of patients was active HF diagnosis (n = 647). In this subgroup, there was an absolute decrease in 30-day readmission of 6.2% between the untreated and attempted (p = 0.04) and between the untreated and treated groups of 6.6% (p = 0.08). Ninety-day readmission for HF patients was decreased by 9.7% when comparing untreated and treated groups (p = 0.04) and 9.9% between untreated and attempted groups (p = 0.01).
Thirty-day ED utilization was reduced by an absolute difference of 4.9% between untreated (p = 0.2) and 7.1% between untreated and treatment (p = 0.09), and 90-day ED utilization was reduced by an absolute difference of 4.6% between untreated (p = 0.3) and 5.3% between untreated and treatment (p = 0.3). Subgroups of PNA (n = 72) and COPD (n = 420) were also analyzed and both populations observed a 30-day readmission rate decrease between the untreated and attempted groups, with a decrease of 8.1% in PNA patients (p = 0.5) and 2.9% in COPD patients (p = 0.5) Statistical testing for 90-day readmission rates and both 30- and 90-day ED visit rates can be found in Table 4.
Total Population and Subgroups: Readmission Rate and Emergency Department Visit Rate Results
Three tested subgroups (HF, PNA, and COPD) averaged more prescription medications (11.5, 11.5, and 13.7) compared to the total population, averaging 9.4 (p < 0.001, p = 0.1, and p < 0.001, respectively). In addition, all three subgroups (HF, PNA, and COPD) averaged more high-risk medications upon discharge (2.5, 3.2, and 2.9) compared to the total population (1.9), with differences all statistically significant (p < 0.001, p < 0.001, and p < 0.001, respectively).
Patient enrollment was a key secondary outcome the authors wanted to investigate. Of the treated patients who had a successful initial CMM visit immediately post-discharge, the success rate for subsequent follow-up visits among treated patients decreased to 68.6% and 42.1% of patients having successful CMM visits 30 days and 60 days post-discharge, respectively.
Patient satisfaction was measured through a survey after each visit. On a scale of strongly agree (1) to strongly disagree (4), 20.6% of patients completed an optional patient satisfaction survey, averaging a 1.1 for satisfaction with care received, 1.0 for the ability to ask the pharmacist any question/concern they had, and 1.1 for leaving the appointment with a clear understanding of the purpose of all their medications.
During the program's launch, engagement methods with health care providers were not yet fully developed, and provider engagement was identified as the final secondary objective to be measured. Upon receiving feedback from pharmacists regarding patient concerns, the authors adapted their approach. They began evaluating the number of interventions made by pharmacists, as well as the acceptance rate of these interventions by health care providers.
Subsequently, it was observed that patients with HF received a higher average number of interventions, leading to the development of a provider engagement model for this particular subpopulation. The study concluded with a total of 483 pharmacist interventions implemented for the HF group (n = 647), including optimizing guideline-directed medical therapy, improving access to medical care and HF medications, identifying poor adherence to HF medications, and addressing HF exacerbation symptoms. Given the emergent nature of some interventions, health care providers were contacted 45 times, with a 59% acceptance rate.
Discussion
CMM benefit was observed due to key factors such as the continuity of care achieved by monitoring of medications between encounters, the multidisciplinary WPH Cares team that assessed and guided care coordination and social factors, an emergent issue protocol, EMR access, and most importantly, building a trusting pharmacist-patient relationship through various engagement processes to increase individualized medication action plans for patients.
This study investigated the impact of implementing a structured telehealth-based QI program focused on decreased readmissions and ED visits, while driving patient engagement, and program enrollment utilizing a multidisciplinary team. The study observed positive outcomes resulting from each process improvement, indicating a beneficial influence on the overall program. Comparing the program's start to its end, there was an overall average increase in patient volume, enrollment rates, and patient engagement. Through our methodical approach to QI and implementation of such a program, we noted enhancements in patient engagement, the provision of personalized interventions, streamlined communication processes, heightened program enrollment rates, and ultimately improved program effectiveness through the course of this initiative. These results highlight the importance of utilizing a structured QI approach with a multidisciplinary team to drive QI efforts within health care organizations.
This is the largest-sized prospective QI initiative of a telehealth pharmacist service implemented to date across a diverse and complex patient population. This confirms and adds value to the current literature by demonstrating a statistically significant reduction in all-cause hospital readmissions. 20
There were several limitations to this study. Enrolling 57.5% of outreached patients prevented the observation of the full benefit of CMM. However, this was a program to evaluate the feasibility of a detached telehealth program; therefore, there was no inpatient protocol to notify patients of the program and outreach proceeded to occur after discharge. This workflow design can be improved by making initial contact with eligible patients before discharge. Second, the Cureatr Clinic team had read-only access to WPH's EMR, which limited the team's success with engaging providers regarding recommendations and medication issues. Third, there were many patients who were referred and received help from social work specialists; however, quantifiable data regarding these visits were not produced. Additional studies addressing these limitations will provide this model with a more holistic view of its benefits.
Future Directions
Ensuring the sustainability of a QI intervention is of high importance. To achieve lasting impact, several key strategies come into play. First, integrating the intervention's data and outcomes into the EMR system is pivotal to effectively incorporating it into the hospital's workflow. This facilitates data sharing and empowers health care professionals to monitor patient progress and trends across sites, and make informed decisions. Second, the establishment of indicators for course correction is crucial as the initiative expands. By setting clear metrics, the team can continuously assess the intervention's efficacy, enabling real-time adjustments to keep it aligned with its goals and adaptable to emerging challenges. Finally, integrating the intervention with existing hospital workflows promotes a holistic patient care approach, fostering sustained improvements through synergies with broader health care strategies and interdisciplinary collaboration.
Conclusion
In the largest telehealth pharmacist intervention report to date investigating the role of CMM in transitions of care of vulnerable patient populations, our study demonstrated statistically significant reductions in readmission and ED utilization for treated patients, in addition to sound mechanisms for increasing patient volume, engagement, and enrollment into similar programs. The favorable contributions of telehealth pharmacist services and CMM strategies recognized in this study have the potential to provide integral care coordination capabilities necessary to achieve national policy goals for enhancing the impact of primary care models of care. 21 These additional benefits may be best realized by improving health outcomes in the therapeutic management of patients with complex care issues in rural, underserved, and disadvantaged populations. CMM pharmacist services may play a key role in achieving benchmarks of chronic disease management in designing future value-based care reimbursement models.
Footnotes
Acknowledgments
The authors acknowledge these individuals for their support and participation: From White Plains Hospital - Leigh Ann McMahon, DNP, MHA, RN, NEA-BC, Rafael E. Torres, MD, FACEP, Michael J. Palumbo, MD, FACP, Priscilla Harmon, MHA, Karen Banoff, DNP, and Jonathan Sege. From Cureatr Clinic - Tatiana Wright, PharmD, Meghan Smart, PharmD, Vidhi Patel, PharmD, BCPS, Zarah Mayewski, PharmD, BCPPS, and Phillip Kelly. From CWH Advisors - Tanner Johnson. From Olive AI - Jason Silverstein, MBA
Authors' Contribution
Conceptualization: F.N.J.; Methodology: T.T., M.P., G.D., E.O., B.C., and F.N.J.; Data curation: T.T., M.P., and E.O.; Formal analysis: T.T., M.P., and E.O.; Investigation: T.T., M.P., G.D., E.O., and F.N.J.; Writing–original draft: T.T., M.P., G.D., E.O., B.C., and F.N.J.; Writing–review & editing: T.T., M.P., G.D., E.O., B.C., and F.N.J.; Funding acquisition: F.N.J.
All authors have read and approved the final article.
Author Disclosure Statement
Eric Olmsted received monetary compensation from Cureatr Clinic for his statistical analysis services for the analysis of this research article. The remaining authors declare that they have no conflicts of interest to disclose.
Funding Information
This study was not funded by any external source.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.