
Abstract
Background:
Telemedicine has been differentially utilized by different demographic groups during COVID-19, exacerbating inequities in health care. We conducted conjoint and latent class analyses to understand factors that shape patient preferences for hypertension management telemedicine appointments.
Methods:
We surveyed 320 adults, oversampling participants from households that earned <$50K per year (77.2%) and speak a language other than English at home (68.8%). We asked them to choose among 2 hypothetical appointments through 12 conjoint tasks measuring 6 attributes. Individual utilities for attributes were constructed using logit estimation, and latent classes were identified and compared by demographic and clinical characteristics.
Results:
Respondents preferred in-person visits (0.353, standard error [SE] = 0.039) and video appointments conducted through a secure patient portal (0.002, SE = 0.040). Respondents also preferred seeing a clinician with whom they have an established relationship (0.168, SE = 0.021). We found four latent classes: “in-person” (26.5% of participants) who strongly weighted in-person appointments, “cost conscious” (8.1%) who prioritized the lowest copay ($0 to $10), “expedited” (19.7%) who prioritized getting the earliest appointment possible (same/next day or at least within the next week), and “comprehensive” (45.6%) who had preferences for in-person care and telemedicine appointments through a secure portal, low copayments, and the ability to see a familiar clinician.
Conclusions:
Appointment preferences for hypertension management can be segmented into four groups that prioritize (1) in-person care, (2) low copayments, (3) expedited care, and (4) balanced preferences for in-person and telemedicine appointments. Evidence is needed to clarify whether aligning appointment offerings with patients' preferences can improve care quality, equity, and efficiency.
Background
Early evidence indicates high acceptability of telemedicine, even among low-income patients of various racial/ethnic backgrounds. 1 –8 However, telemedicine may not always be the most effective or acceptable avenue to providing care to all groups. 9 –11 These findings highlight the need to develop methods health care organizations can use to efficiently identify patient preferences for telemedicine and tailor offerings to diverse patient needs and preferences. It is especially important to measure preferences of racial and ethnic minority patients and low-income patients who are often not represented in scientific studies. 12 –14
Conjoint analysis is a survey-based market research method with potential applications to assist health care organizations in better understanding and serving diverse patient's needs. 15,16 Patients' valuation of different attributes of a real or hypothetical product or service can be calculated and directly compared through repeated tasks in a conjoint survey. 17 –19 Compared with traditional survey methods, conjoint surveys allow for more realistic scenarios that increase the external validity of collected data, and provide a more detailed analysis with direct comparison of attributes. 17
To our knowledge, conjoint analysis has not been used to address patient needs and equity concerns regarding telemedicine services. Latent class analysis uses a conjoint data set to find groups of responders who share similar preferences that are not defined a priori. 17 Latent class analysis further enhances the utility of conjoint methodology over traditional survey methods by avoiding a “one-size-fits-all” approach that may not adequately capture the needs of vulnerable populations. 17,18
This work studies telemedicine acceptability among adults with hypertension. Owing to hypertension's prevalence, association with increased risk for other comorbidities, and disproportionate impact on community health center (CHC) patient populations, 20 –25 as well as its ability to be addressed through continuous monitoring, regular interactions with clinicians and other health care personnel, and quality of care improvement efforts, 22 hypertension is highly appropriate for treatment through telemedicine. 26
A systematic review by Xu et al. demonstrates the importance of addressing diverse care preferences when managing hypertension, as well as incorporating patient-centered decision making into hypertension care to maximize patient outcomes and adherence to treatment. 27 Conjoint and latent class analyses can elicit preferences and segmentation in preferences so that health care organizations and clinicians can better provide patient-centered care. 16
To understand factors that impact telemedicine acceptability for hypertension management, conjoint and latent class analyses were conducted to identify preferences of adults with hypertension in the United States typically served by CHCs.
Methods
DATA
Participants were recruited through Dynata, LLC from a pool of individuals with expressed interest in participating in surveys for research. Eligible participants were at least 18 years old and spoke English. Participants from households earning <$50K per year (77.2%) and who speak a language other than English at home (68.8%) were oversampled.
Our conjoint survey had a maximum of 4 levels per attribute, 12 tasks, and 2 alternatives per task, yielding a desired sample size of n = 167 individuals. The study and survey were approved by the University of California, Berkeley Office for the Protection of Human Subjects (IRB protocol ID: 2022-01-1499).
MEASURES
Participants were asked to complete a survey written in English including demographics to determine eligibility and framing for other survey questions (language spoken at home, English proficiency, age, hypertension status), 12 conjoint tasks, and additional demographics questions (gender, race/ethnicity, annual household income, employment status, parent/caregiver status, regular access to health care, number of health care visits in 2022, home internet access, and health conditions). The survey was administered through internet through a link provided to participants by Dynata, LLC that directed participants to the survey hosted by Sawtooth Software, Inc. on their website.
This website was only accessible through individualized links. Upon clicking on the link, participants were presented with a description of the study, including potential risks and benefits of participating, data privacy, a statement notifying them of their voluntary participation, and contact information for investigators and the University of California, Berkeley Office for the Protection of Human Subjects with the protocol identification number listed (Protocol ID: 2022-01-1499). The information page also included a statement notifying participants that clicking the “next” button indicated consent to participate in the study.
The statement also indicated that participation could be declined or revoked at any time by closing the window or contacting the investigators. Beyond oversampling of low-income individuals and individuals who spoke a language other than English at home, no selection criteria were used for recruitment. Participants indicating an age <18 years or English proficiency less than “well” or “very well” were directed to a webpage informing them of their ineligibility.
Six individual attributes of interest (ability to see a clinician with whom there is an established relationship, profession of available clinician, copayment, appointment type, time of available appointment, and earliest available appointment) were established for the conjoint tasks. Attributes were determined from prior qualitative research eliciting barriers and facilitators of telemedicine adoption through clinician and patient interviews from federally qualified health centers. 28 Each task was presented alongside a scenario about ongoing hypertension management for those with hypertension (46.3%) and a simulated scenario for those without a hypertension diagnosis (34.7%).
Participants were presented with a binary choice between two visits varying by the ability to see a clinician with whom there is an established relationship, profession of available clinician, copayment, appointment type, time of available appointment, and the earliest available appointment. Participants could also choose not to select either of the two presented options through a button marked “NONE: I would not choose any of these.” Attribute choices were randomized for each of the 12 conjoint tasks, though the exact same question (both options having the same levels of the 6 attributes) was not presented to the same participant across the 12 tasks. A sample conjoint task is presented in Figure 1 and the full survey is presented in Supplementary Content S1.
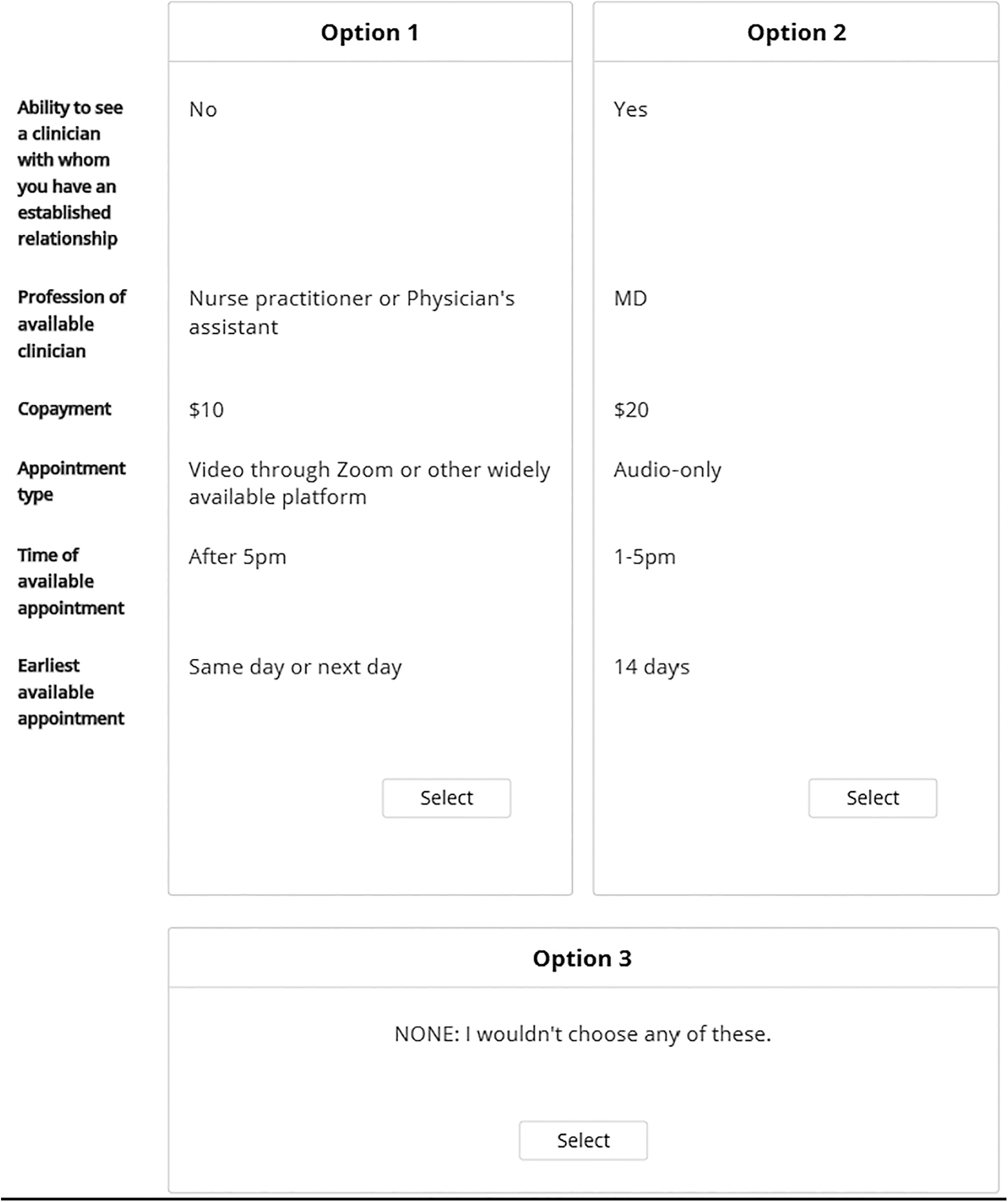
Sample conjoint task.
STATISTICAL ANALYSES
All conjoint and latent class analyses were conducted using Lighthouse Studio 9.14.2 (Sawtooth Software, Inc.). Through 12 repetitions of the conjoint task, individual utilities for hypertension management appointments across attributes were constructed using logit estimation, allowing for aggregate utility estimations for the entire sample population.
Incomplete survey responses (n = 85) and responses from participants who spent <150 s to complete the survey (n = 30) were excluded from final analyses. These exclusions helped ensure accuracy and validity of responses.
Predictive validity was examined through asymptotic t-tests to test for validity of individual attributes and likelihood ratio tests for the overall validity of models to ensure usefulness for predicting patient choice of telemedicine or in-person visits under varying attribute levels.
Given multiple submodalities of telemedicine, a nested logit model was used (Fig. 2). 29 The number of latent classes was determined through goodness-of-fit for models, including the Bayesian information criterion.

Diagram of nested logit model.
The resulting latent classes were compared for differences in demographic composition using chi-square tests for overall demographic distribution and dummies for each level of demographic characteristics. Any groups without sufficient counts to maintain statistical power were combined with other groups or dropped from subanalyses. 30
All equations for conjoint and latent class analyses are presented in Supplementary Content S2.
SENSITIVITY ANALYSES
To examine differential preferences for participants with and without a current hypertension diagnosis, we striated the sample by hypertension status and conducted independent conjoint analyses (using logit models), comparing the zero-centered utilities for each attribute between the two groups. Linear regressions examined the relationship between self-efficacy in managing hypertension and telemedicine preferences.
Statistical analyses were conducted using Stata 17.0 (StataCorp, LLC). The University of California, Berkeley's institutional review board approved the study protocol.
Results
A total of 435 adults participated in the conjoint survey. Participants who did not complete the survey (n = 85, 19.5%) and those who spent <150 s completing the survey (n = 30, 6.9%) were excluded, resulting in a final analytical sample of 320 adults of which n = 148 (46.3%) had a hypertension diagnosis. Most (n = 247, 77.2%) participants belonged to households making <$50K per year, 95.9% (n = 306) of participants reported having access to broadband internet at home and had an average of two chronic conditions (average: 1.9, standard deviation = 2.3, range: 0–12) (Table 1).
Demographics of the Analytical Sample
For questions where not all participants answered, counts of the number of participants that answered are presented with percentage of the total sample (n = 320).
Some demographic groups did not contain enough individuals to be adequately powered for analyses. Individuals in the 75–84 years old (n = 6) and the 85+ years old (n = 5) age groups were combined into a new 75+ years old age group. Those reporting contract or temporary employment (n = 8) were combined with those reporting part-time employment (n = 64). Those who reported speaking English “not well” (n = 2) were combined with those reporting “well” (n = 36).
Those reporting Veterans Affairs as their regular source of health care (n = 3) were combined into the “some other place” category (n = 13). These changes are reflected in Table 1, which reports our final analytical sample. The individuals reporting “other” as their gender (n = 1) and the n = 4 individuals reporting “other” as their race/ethnicity were also excluded from gender- and race/ethnicity-based analyses, although they are included in the overall analytical sample.
Overall, respondents had positive zero-centered utility for in-person visits (0.353, standard error [SE] = 0.039) and video appointments conducted through a secure patient portal (0.002, SE = 0.040), meaning patients preferred these appointment types over audio-only visits or visits through a popular consumer video call platform (Table 2). Respondents preferred visits before 5 pm (8–11 am: 0.010, SE = 0.040; 11 am–1 pm: 0.034, SE = 0.040; 1–5 pm: 0.006, SE = 0.040) and appointment options with availability within the next 7 days (same day or next day: 0.375, SE = 0.039; within 7 days: 0.094, SE = 0.040).
Results of Logit Analysis for Overall Sample (Zero-Centered Differences)
SE, standard error.
Respondents also preferred seeing a clinician with whom they have an established relationship (0.168, SE = 0.021) and visits with a physician (0.111, SE = 0.032). Participants had positive zero-centered utility for copays $10 or less ($0: 0.330, SE = 0.039; $10: 0.091, SE = 0.040), meaning, in general, patients were willing to pay a small copay to meet their preferences.
Latent class analysis yielded four major groups of participants based on their priorities when selecting an appointment for hypertension management. Although major test-of-fit statistics showed improvement in statistical fit with more fragmented grouping, results for the five-group analysis yielded two groups with an overlap in preference characteristics (similar ranking of attribute importance with different magnitudes of measured utility for each attribute). Therefore, we proceeded with a four-group model categorized as the “in-person” group (26.5% of participants), “cost conscious” group (8.1%), “expedited” group (19.7%), and “comprehensive” group (45.6%) (Table 3).
Latent Class Analysis of Hypertension Management Care Preferences
The “in-person” group strongly weighted in-person appointments, the “cost conscious” group prioritized the lowest copay, the “expedited” group prioritized getting the earliest appointment possible, and the “comprehensive” group had multiple high-priority preferences, including appointment type (with a preference for in-person or video visit through secure patient portal), copay (with a preference for $0 to $10 copays), and the ability to see a familiar physician to prioritize appointment selection ( Tables 3 and 4 ).
Results of Latent Class Analysis in Zero-Centered Differences in Utility
Participants in the “in-person” group tended to be older than those in other groups and participants in the “comprehensive” group tended to be the youngest (χ 2 = 48.396, p < 0.001). Those in the “cost conscious” group were more likely to have low household annual incomes (<25K/year: 50.0%; $25K–$49,999/year: 38.5%) and participants in the “comprehensive” group had the lowest percentage (27.4%) of participants making <$25K/year and the highest percentage (14.4%) making >$100K/year (χ 2 = 37.615, p < 0.001).
Those in the “comprehensive” group were also most likely to have full-time employment (χ 2 = 50.874, p < 0.001). Members of the “cost conscious” group were also least likely to be a parent or caregiver or have an established place of care and members of the “comprehensive” group were most likely to be a parent or caregiver and have an established place of care (parent/caregiver: χ 2 = 11.078, p = 0.011; established place of care: χ 2 = 11.080, p = 0.011). Those in the “expedited” group reported the most appointments in the past year and members of the “cost conscious” group reported the least number of visits in the past year (χ 2 = 20.880, p = 0.013).
The groups did not significantly differ on other demographic characteristics, including race/ethnicity or whether the participant had diagnosed hypertension. Full demographics comparisons of the groups are presented in Table 5.
Demographics Comparison of Latent Classes
For questions wherein not all participants answered, counts of the number of participants who answered are presented with percentage of the total sample (n = 320).
When participants with and without a hypertension diagnosis were examined separately, logit analysis revealed participants with hypertension exhibited a positive utility for in-person appointments (0.338, SE = 0.057) and video telemedicine appointments through a secure patient portal (0.036, SE = 0.058), whereas participants without a diagnosis only exhibited positive utility for in-person appointments (0.372, SE = 0.054). Participants with hypertension also exhibited a positive utility for appointments from 8 am to 1 pm (8–11 am: 0.076, SE = 0.058; 11 am–1 pm: 0.021, SE = 0.058), whereas those without hypertension exhibited a positive utility for appointments from 11 am to 5 pm (11 am–1 pm: 0.040, SE = 0.055; 1–5 pm: 0.051, SE = 0.055).
Results of the analyses separated by hypertension status are presented in Supplementary Content S3. There were no differences in latent class distribution for participants with hypertension based on their confidence in managing their hypertension (Supplementary Content S4).
Discussion
We found that video-based telemedicine through a secure patient portal had a positive zero-centered utility for adults. Preferences for video encounters through secure patient portals, rather than widely used platforms, underscore the need for health care organizations to invest in telemedicine infrastructure, especially patient portals that support secure, encrypted, and Health Insurance Portability and Accountability Act of 1996 (HIPAA) 31 compliant video chat services. This study contributes evidence that telemedicine is a worthwhile investment for health care organizations providing care to patients with hypertension.
Telemedicine appointments also provide opportunities for patients to have lower copayments, 32 which may increase utilization among lowest income patients and help meet the needs and priorities of all patients. Our results related to copayments are consistent with evidence that telemedicine increases cost-effectiveness of mental health treatment at the organizational level, which could translate to hypertension care, 33,34 creating a scenario where both patients and hypertension care providing institutions can save on care-associated costs.
There was a strong preference for the ability to see a familiar clinician by patients across the board, which is consistent with recent literature on telemedicine adoption that found established relationships between clinicians and patients are a major facilitator of successful telemedicine adoption. 28,35 –38 Our finding that the “in-person” group was composed of older individuals also matches literature pointing to potentially low interest and less satisfaction with telemedicine appointments among older patients. 10,11 Also, our findings of positive zero-centered utilities for in-person and video visits and negative zero-centered utility for telephone visits are supported by previous evidence finding high interest in video visit among various demographics groups, including patients typically served in safety net settings. 1 –8
Finally, our finding that telemedicine preferences for hypertension care did not differ by race/ethnicity further supports the idea that telemedicine could support equitable care. 39 Our results highlight that low-income adults are interested in telemedicine, consistent with recent evidence. 4,7,11 Telemedicine can help overcome access barriers that disproportionally impact low-income patients, including travel time and childcare needs compared with in-person appointments. 35,40 –45
These factors could be key considerations for patients in the “comprehensive” group, who are more likely to be parents or caregivers, and patients in the “cost conscious” group, who have less flexibility in their schedules or more barriers to attending in-person appointments. Satisfying patient preferences for care modalities may improve patients' experiences of care.
A few limitations of this study should be considered. First, participants were recruited through a service with an established participant pool and the survey was distributed and administered through a digital interface. The results may not generalize to adults with lower technology literacy and without broadband internet at home. Survey data collection services, like the one used for this study, do not always have populations reflective of the general population based on race/ethnicity, gender, and age. 46,47 The information initially used to sample participants is self-reported. 46 To address potential misclassification, we added screeners in the survey to verify key demographics.
In addition, some participants using services such as Dynata, LLC may rush through surveys, yielding low-quality data. 46,47 To improve data quality, we used our own statistical accuracy screener to remove respondents who spent <150 s to complete the survey from the analytic sample. Second, although there are many strengths of conjoint and latent class analyses in maximizing resources and efficiency, as well as predicting the best offerings in general for different patients, results of this and similar studies should not be taken as a replacement for working with patients on an individual level to develop a care plan.
Third, we do not have data on some participant demographics that may influence preferences outside those measured in this study. Participants' perceptions of relationship quality with their primary care provider may influence preferences for the ability to see a familiar clinician. Previous experiences receiving care from nonphysician clinicians may influence their utility for clinician profession. Also, the details of participants' insurance coverage and benefits, such as deductibles, may influence preferences around copay.
Finally, for our conjoint analysis we also assume that introducing a new alternative would not significantly impact the choice between the two presented alternatives in each conjoint task. However, our methodology has shown to be successful in predicting choice and utilities despite this limitation. 19
Latent class analyses of patient preferences for remote care help guide clinicians and staff responsible for scheduling hypertension care appointments in offering different modalities for patients in settings where these options are available. Telemedicine may also allow more flexibility of appointment times for care teams to address the needs of large groups of patients, including patients who fall into the “expedited” and “comprehensive” groups. 5,48
Future research should expand the participant population of conjoint and latent class analyses beyond the convenience sample used in this study and use these methods to determine patient utility for different modalities of appointments for conditions beyond hypertension. These methods could also be used internally in health systems and provider organizations to increase access to care, meet patient preferences, and improve the quality of care through telemedicine adoption, adaptation, or sustainability.
Conclusions
Conjoint and latent class analyses of appointment preferences for hypertension management indicate that participant preferences can be segmented into four groups with different preference orderings that prioritize (1) in-person care, (2) low copayments, (3) expedited care, and (4) balanced preferences for in-person and telemedicine appointments through a secure portal, low copayments, and the ability to see a familiar clinician. Evidence is needed to clarify whether aligning appointment offerings with patients' preferences can aid with reducing no-show rates and improving treatment adherence, quality of care, equity in patient outcomes, and efficient allocation of resources.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded by a grant from the Center for Information Technology Research in the Interest of Society (CITRIS) and the Banatao Institute. A.A.T. received support from the Agency for Health Care Research and Quality (Grant No. T32HS022241).
Supplementary Material
Supplementary Content S1
Supplementary Content S2
Supplementary Content S3
Supplementary Content S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.