
Abstract
Introduction:
Almost half of veterans (44.6%) seen in the U.S. Department of Veterans Affairs outpatient setting are diagnosed with hypertension (HTN). Because of the widespread nature of HTN, use of virtual visits has the potential to improve blood pressure (BP) management. This evaluation assessed the effectiveness of video blood pressure visits (VBPVs) in the management of HTN in veterans enrolled in Veterans Health Administration primary care.
Methods:
The program was implemented within the existing veteran-centered medical home. VBPVs are scheduled where the nurse observes veterans taking their BP and provides teaching or counseling. A national training curriculum was delivered to local nurse champions through Microsoft Teams. We analyzed improvement in BP over a 2-year period. We also captured actions taken by nurses during the VBPV by searching the electronic notes. Ratings of training and comments were summarized using feedback forms completed after training.
Results:
In total, 81,476 veterans participated in VBPVs over 2 years. Of those, 44,682 veterans had an existing ICD-10 code related to HTN. Of the 18,078 veterans who had a pre- and post-VBPV BP, the average change to systolic measurement was −10.6 mm Hg (range −82 to 78). Average change to diastolic measurement was −4.61 mm Hg (range −59 to 55). Most interventions addressed medication management (77%). Nurses' evaluations of the program were positive.
Conclusions:
Video visits provide reliable and convenient veteran-centered care. Such visits enable care when unanticipated interruptions occur such as the coronavirus disease 2019 pandemic. In addition to medication management, nurse-led interventions such as counseling on lifestyle changes can be effective in HTN management.
Introduction
Hypertension (HTN) is a medical condition that can lead to serious outcomes such as heart disease and stroke, which are two leading causes of death in the United States. 1 Approximately 5.51 million veterans were cared for in the Veterans Health Administration (VHA) primary care clinics during fiscal year 2021. Of those, 44.6% (2.46 million) had a diagnosis of HTN, making it the most common chronic condition among the veteran population. Leading experts in management of high blood pressure (BP) 2 recommend out-of-office BP measurements to confirm the diagnosis of HTN and for titration of BP-lowering medication, in conjunction with telehealth counseling or clinical interventions.
Traditionally, BP visits with a clinical provider have been performed in person and can involve travel in challenging circumstances, particularly for rural veterans. As a result, veterans may neglect their appointments altogether, and lifestyle or medication interventions recommended in the veterans' care plan receive little or no follow-up, further exacerbating the veterans' condition.
The VHA's large size and diverse patient population creates challenges for access to care, thus it was an early adopter of telemedicine and other virtual technologies. Barriers to adoption of virtual care include connectivity, access to equipment, and digital literacy. 3 Video blood pressure visits (VBPVs) are an optimal introduction to the broader application of virtual care. Using the VHA Video Connect (VVC) system, in 2018 a facilitated implementation of VBPVs by nurses was conducted in two VHA health care facilities. Both sites increased from <5% VVC use to >85%. At one site, providers completed four times as many VA Video Connect visits as other providers in their regional network.
Based on their success, the VHA Performance Accountability Workgroup approved entry of visualized tele-BP measurements into the medical record for clinical use and performance reporting. The VBPV program allows veterans to replace an in-person visit with a virtual visit, helping the veterans to follow through on their treatment plan. These visits can also save the veteran time and cost of travel, stress of finding parking, cost of childcare or time off work, and a copay for the visit. Increasing home BP monitoring also helps promote veteran participation and ownership of their own health management.
Although there are multiple studies assessing the use of home telehealth technologies to closely monitor and manage chronic illness over time, this is the first program to our knowledge that uses a video clinic visit enabling a nurse to directly observe the veterans in the home taking their own BP. The evaluation reported here is a retrospective study using routine clinical management data to assess the effectiveness of VBPVs in improving BP in veterans enrolled in VHA primary care. This evaluation was reviewed and approved by the VHA Central Institutional Review Board.
Methods
VIDEO BP VISIT PROGRAM
Primary care within the VHA is organized using the patient-centered medical home model, known in VHA as Patient Aligned Care Teams (PACT). Provider teams include a primary care provider, registered nurse (RN) care manager, clinical associates (e.g., licensed practical/vocational nurses, health technicians, or intermediate care technicians), and a clinic administrative clerk. Each PACT cares for an assigned panel of patients. Using principles of population management, the RN care manager is responsible for using VHA data repositories to locate and review veteran-specific data on a variety of clinical dashboards to identify patients who need chronic disease interventions, either during scheduled visits or for between-visit care, for example, high blood glucose/A1c measures and high BP.
The VBPV program employs VVC to conduct visits for veterans with an established HTN diagnosis, veterans who have a high BP reading requiring follow-up, or veterans with diabetes. Visits may also be conducted with veterans who require screening for high BP. Once identified as needing follow-up care, the provider team schedules a VBPV with the veteran. The veteran is scheduled and receives a virtual appointment link to connect to the nurse at the agreed upon date and time.
The veteran is scheduled and receives a virtual appointment link to connect to the nurse at the agreed time and date. VBPVs are scheduled for 15 min. Only VHA-issued BP cuffs, which are standardized across all VHA locations, are used for these visits. A key component of the visit is that the nurse directly observes veterans taking their BP to ensure that an appropriate technique is used by the veteran per VHA-Department of Defense (DoD) Guidelines for Management of HTN.
For example, if more than one BP is taken during the visit, the nurse will guide the veteran to wait the appropriate time intervals between BP measurements. The nurse also may need to educate the veteran on other aspects of taking BP, for example, proper cuff placement. Based on individual veteran needs, the nurse may provide education and counseling during the visit that is documented on a designated note template in the electronic health record (EHR). Coordination with the clinical pharmacy practitioner for medication addition or adjustment may also occur.
TRAINING FOR NURSES
At each participating facility, one or more nurse champions are identified to attend training on the program. Nurses may self-enroll with the permission of their supervisor, or the nurse manager may identify which nursing staff will attend. Recruitment outreach efforts and/or program advertisements are also employed to increase registration numbers. Site selection for training is focused on sites with high rurality, low virtual care usage numbers, and/or low rates of meeting quality metrics for veteran BP control.
Sites are also identified with assistance from VHA's Office of Primary Care Monitoring and Oversight (PCMO) team. The PCMO team identifies facilities that have opportunities to enhance virtual care access. PCMO team also shares the top 10 facility access outliers and sites that trigger HTN/cardiovascular risk opportunities for improvement.
Training is delivered using the Microsoft Teams platform. All VHA employees have access to the Microsoft Teams platform. Training is delivered to a cohort of champions over eight sessions (Table 1 with outline of training topics). Sessions are provided by nurse program facilitators using live video presentations. Each presentation is recorded for later viewing if participants were unable to attend or want to review the content. Other useful documents are posted on the Microsoft Teams site for easy access to the local staff.
Overview of Training Sessions
ATLAS, Accessing Telehealth through Local Area Stations; BP, blood pressure; CVT, clinical video telehealth; PACT, Patient Aligned Care Teams; SFT, store-and-forward telehealth; VA, Veterans Affairs; VBPV, video blood pressure visit; VCM, virtual care manager; VHA, Veterans Health Administration; VISN, Veterans Integrated Service Network; VSSC, VHA Support Service Center; VVC, Veterans Affairs (VA) Video Connect.
A project action plan is submitted by participants at the conclusion of the cohort training sessions. Using a train-the-trainer model, local nurse champions both implement the VBPV program and help other nurses adopt the practice. At some sites, local leadership also attend training to learn about the program and support local buy-in and engagement. The VBPV program is accredited through the American Nurses Credentialing Center, and nurses who attend the course and complete an action plan are eligible to earn 8 h of Nursing Continuing Professional Development.
In addition to the training sessions, regularly scheduled “open houses” are used to discuss problems and issues with implementing the program. Open house sessions are targeted toward both current, prior, and future cohort participants for troubleshooting and to capture and share local knowledge.
ELECTRONIC NOTE TEMPLATE
Early in program implementation, a VBPV electronic note template was developed to document the visit. This standardized template provides an outline to conduct the VBPV and facilitates the ability to capture and document visualized veteran BP, review symptoms, and review medications. After 1 year, the template was updated to include new fields and language changes to improve data capture, streamline visit workflow, and nurse documentation. The template update is aligned with the VHA/DoD Clinical Practice Guidelines for HTN in primary care and incorporates whole health principles. National standardized structured data fields (referred to as health factors) are included to improve the ability to capture nursing activity during the visit. Additional features include: ability to capture and document self-reported BPs; inclusion of a field for documentation of pulse captured during the VBPV with the VHA-issued BP device; addition of optional fields to document date, time, and type of BP medication taken; addition of verbiage—“blood pressure directly observed by a clinician through video conferencing and the results are interpreted by a clinician,” which is required for the measurement to count for VHA BP quality metrics; and addition of a drop-down box with measurements (centimeter and inch) to document the size of the BP cuff.
Health factors are electronic data fields that can be queried within the VA EHR to capture a variety of data. The VBPV template contains >30 health factors, including patient education topics The health factors in the VBPV template can generally be categorized into the following:
BP measurement and pulse (these structured fields allow for the data to be captured vs. free text into a narrative note);
evidence-based interventions that optimize HTN treatment, including medication adherence and standardized counseling on exercise and nutrition;
follow-up actions that prompt cointerventions to enhance the management of HTN and including weight loss, physical activity, adopting the Dietary Approaches to Stop Hypertension eating plan, moderation of alcohol consumption, and reducing sodium intake along with the ability to indicate referral/notification to the pharmacist, dietician, weight loss program (MOVE!), and home telehealth; and
whole health approach that assists the health care team in understanding and developing individualized and personalized health plans.
DATA COLLECTION AND ANALYSIS
Data were collected on the number of veterans receiving VBPVs (both unique veterans and encounters) for two fiscal years (September 30, 2020–October 1, 2022). Data were obtained through national VHA patient databases: the VHA Informatics and Computing Infrastructure (VINCI), including VHA outpatient encounter files, vital signs, vital status files; Corporate Data Warehouse (CDW); Decision Support Services National Pharmacy extracts; and Planning System Support Group (PSSG) geo-coded enrollment files.
The CDW query included patient visit instances where primary stop codes within values (322, 323, 342, 348, 350, 685, 704) (primary stop codes designate the main clinical group responsible for care) and secondary stop codes within values (179, 648) (secondary stop codes provide additional information about the clinic such as the provider type or if the service was delivered through telehealth technology). Further filters included were date of visit; provider type “nursing service” with a classification of RN, licensed practical nurse, licensed vocational nurse; and vital results—all visits where a BP measurement was taken in a VHA clinic. We then further filtered these data to leave only visits that had ICD10 codes related to HTN (Fig. 1).
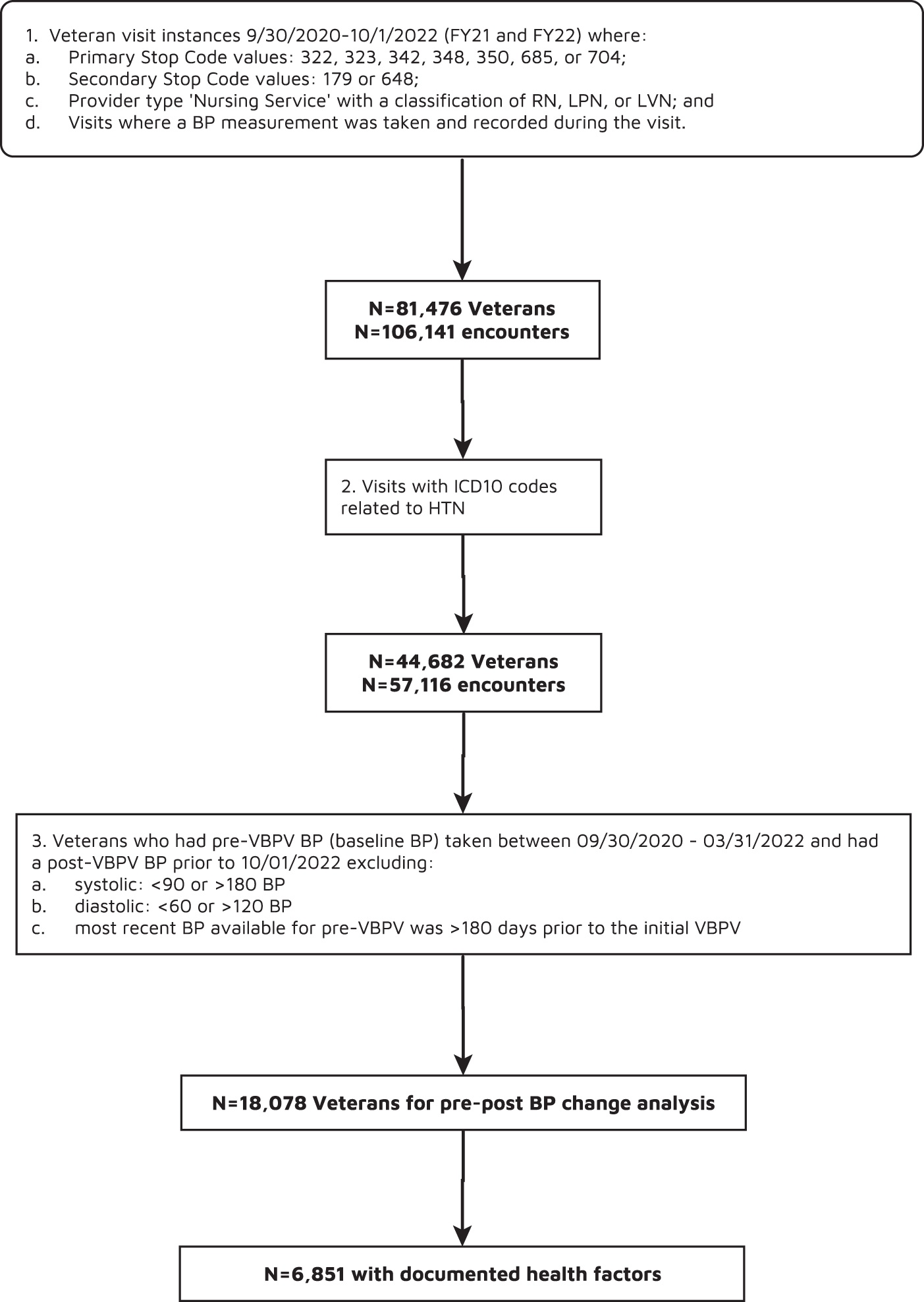
Data extraction. BP, blood pressure; HTN, hypertension; VBPV, video blood pressure visit.
To examine effectiveness, we analyzed improvement in BP, measured as the difference between the most recent BP taken in the clinic before the initial VBPV baseline visit and a subsequent BP taken after the initial VBPV. For this analysis, we included veterans who had the pre-VBPV BP (baseline BP) taken between September 30, 2020, and March 31, 2022, and had a subsequent BP taken up to October 1, 2022 (to create a minimum 6-month follow-up time frame). In this analysis, we used the following exclusion criteria: systolic, <90 or >180 BP; diastolic, <60 or >120 BP 4 ; or whether the most recent BP was obtained >180 days before the initial VBPV. We analyzed pre–post BP changes using a one-sample t-test.
We also captured actions taken by nurses (using health factor data fields) during the VBPV by searching the electronic notes on the date of the visit of veterans identified. Finally, ratings of training and comments were summarized using feedback forms that nurse champions completed after training.
Results
There were 81,476 unique veterans and 106,141 unique veteran encounters who participated in a VBPV during the study time period. Of those, 5,356 were rural veterans (VHA stations that met 50% rurality designation) and 6,921 unique encounters in rural facilities. When these data were filtered by presence of an ICD-10 diagnosis for HTN, there were 44,682 unique veterans and 57,116 unique encounters who participated in a VBPV. Of those, 3,398 were rural veterans and 4,235 unique encounters in rural facilities.
Of the 18,078 veterans who had both a pre-VBPV BP (baseline BP) taken between September 30, 2020, and March 31, 2022, and had a subsequent BP taken before October 1, 2022, the average change to systolic blood pressure (SBP) measurement was −10.6 (range −82 to 78). Average change to diastolic blood pressure (DBP) measurement was −4.61 (range −59 to 55). We then examined changes in SBP and DBP measurements using the following increments: 25–35 days (mimic 1 month); 55–65 days (mimic 2 months); 85–95 days (mimic 3 months); and 170–190 days (mimic 6 months). We used two different methods for handling days where multiple BPs were documented on same day: (1) averaging the BPs taken in unique visit and (2) taking lowest BP taken in unique visit.
A one-sample t-test was used to assess any significant change in systolic and diastolic measurements from initial VBPV measurement. All time increments showed a statistically significant decrease (<0.00001) in both systolic and diastolic values for every increment whether an average BP or the lowest BP was used (Table 2). We then explored the nursing or medical interventions where there was health factor data recorded (n = 6,851) in the veteran group included in the effectiveness analysis (Table 3).
Mean Change in Blood Pressure by Increments
If veteran had multiple BPs in increment, latest one used.
p-value <0.0001 for all increments.
Interventions (N = 6,851) for Veterans Who Had a Pre- and Postvisit Blood Pressure
Multiple interventions may be used per veteran.
Individual intervention percentages reflect interventions within the category.
Total percentages reflect the overall category.
HTN, hypertension.
The number of veteran patient sites receiving training was n = 139 (out of 140 VHA Healthcare Systems). All Veterans Integrated Service Networks (VISNs) have been reached with training. Training sessions were highly rated by participants. The following program benefits were identified in comments written on the course evaluation form: encouraging use of virtual visits with veterans, offering an alternative means for monitoring BPs through virtual encounters, increasing veterans' knowledge, increasing knowledge about existing patient databases by nurses and how to use those to manage patient panels helping address population-specific disparities in care, and facilitating patient-centered care. Participants identified a need to learn more about coding visits to better capture nursing workload.
Discussion
Implementation of a VBPV program demonstrated significant BP reductions in veterans enrolled in VHA care. The average decrease found in this study of around −9 SBP and −3 DBP is close to what other studies find for SBP changes, whereas other literature has DBP changes around 4–5. 5 Prior research has shown that nurse-led telehealth interventions can lower BP, and influence HTN awareness, self-efficacy, and self-control. 6 Nurse participants reported highly positive ratings of the training program using the Microsoft Teams platform.
To our knowledge, this is the first study to employ nurse-visualized BP measurements by patients, ensuring the most accurate BP possible. Kallioinen et al. reviewed and categorized 29 possible sources of inaccuracy in BP measurement into 4 categories: patient, device, procedure, and/or observer related. 7 Visualized BP measurements provide an opportunity to address these sources of inaccuracy and obtain more accurate measurements in the veteran's home environment to optimize treatment plans. Benefits for veterans include an efficient check-in from home with a nurse using readily available equipment.
An additional advantage of this program is that it was implemented within the existing veteran-centered medical home in the VHA. Using principles of population management, the RN care manager is responsible for reviewing clinical dashboards of data populated from VHA data repositories to identify veterans who need chronic disease interventions, either during scheduled visits or for between-visit care, for example, high blood glucose/A1c measures and high BP. Use of VBPVs enables nurses to address between-clinic visit needs, promote provision of health and lifestyle information, and correct errors in the use of BP monitor.
The primary care team collaborated to identify patients likely to benefit from this intervention. Furthermore, the VBPV may have facilitated attention on medication adjustments. The training also facilitated greater understanding by RN care managers of how to access and use existing veteran data in panel management. Using VBPV as a model, nurses envision expanding this approach to other conditions that may be amenable to a video visit for population management. Finally, the program provided an invaluable opportunity for nurses to participate in a performance improvement project and promote career development.
The Microsoft Teams platform provided a shared space for each cohort to interact, ask, and answer questions; share what worked at their local site; and communicate with facilitators and other cohort members. Part of the training was visualizing and practicing a video visit providing a “hands-on” experience with the process. Facilitators also provided ongoing troubleshooting to support the participants. Local champions were highly motivated and committed to telehealth, as many had previous experience with telehealth and/or implementing new programs.
Each participant completes an action plan on how they will implement VBPVs in their own practice and at their VHA location. The formatting of the class and the options to review the recordings later off-line helped facilitate a training program implemented in the primary care setting. The benefits of the Microsoft Teams channel and networking continue to be a part of the success of the program.
There were limitations in the program evaluation. Use of a pre–post evaluation design precluded comparison with veterans who did not participate in the program. We were unable to analyze specific changes in medication for veterans over time. Although a common electronic medical record is used at all VHA facilities, not all sites use the VBPV template when conducting a visit, thus we were unable to capture a complete picture of interventions used. Continuing emphasis and training will be needed for nurses to understand how EHR data influence the ability to measure the effect of nursing interventions on patient outcomes.
Other factors may have contributed to the growth in encounters, for example, coronavirus disease (COVID-19) and the VHA's increasing emphasis on use of telehealth. Although we did not collect formal feedback from veterans regarding use of the program, prior study has shown that veterans are receptive to remote management for support between visits if it is tailored to their needs. 8
In conclusion, video visits provide reliable and convenient veteran-centered care. Such visits enable care when unanticipated interruptions occur such as COVID-19. In addition to medication management, nurse-led interventions such as counseling on lifestyle changes can be effective in HTN management. This is the first study to employ nurse-visualized BP measurements by patients, ensuring the most accurate BP measurement possible. Opportunities exist to apply lessons learned from virtual nurse-led clinics to improve access to care for other chronic conditions in primary care.
Footnotes
Acknowledgments
The opinions expressed herein do not necessarily reflect the views of the U.S. Department of Veterans Affairs or its affiliates nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government.
Disclosure Statement
No competing financial interests exist.
Funding Information
This project was funded by the Veterans Health Administration Office of Rural Health.