
Abstract
Objective:
To demonstrate that a culturally and linguistically appropriate telehealth protocol can be implemented to improve the glycemic control of patients as an extension of regular clinical services and provide continuity of care.
Methods:
A telehealth platform was established during COVID-19 pandemic and from numerous telehealth encounters we sampled 498 patients who received telehealth intervention over a 12-month period for specific services: Rx refill, consultation for laboratory results, wellness evaluation and education, and acute or sick visits with appropriate referrals. This telehealth platform was integrated with a remote patient monitoring system utilizing a Bluetooth-enabled glucometer for patients with diabetes compared to their abnormal baseline hemoglobin A1C (HgA1C). The Blood sugar values were recorded at predefined intervals to monitor controls for diabetes. The ethnic diversity and level of education of patients required addressing the digital divide, language interpretation, and navigation at each monitoring step.
Results:
This method demonstrated that a culturally and linguistically appropriate telehealth protocol can be implemented to improve the glycemic control of patients in an intervention group compared with a control group. Validation of the glycemic control was based on 70 patients identified as eligible for participation based on the inclusion criteria: a HgA1C level of 7% or higher obtained within the last 10 months. Informed consent was obtained for 42 participants based on patient participation constraints during the COVID-19 pandemic.
Conclusions:
We conclude that telemedicine procedures utilized for patients with little or no prior knowledge of remote self-monitoring methods can support their treatment of chronic diseases, such as diabetes. The outcomes from the implementation of telemedicine services were observed in a well-defined group of underserved racial and ethnic minority patients at our clinic. We now have a protocol to expand this to other chronic diseases and used as a regular clinical procedure.
Introduction
COVID-19 placed an urgent requirement for the use of telehealth systems in a clinic setting. Telehealth allows patients to stay connected to their providers (doctors or health consultants) without in-person visits through a combination of audio and video technology, virtual examination rooms, and remote patient communication. Compliance with remote monitoring for triage and treatment at a remote location, such as the patient's home, is an important attribute of any telehealth application. During the pandemic, telehealth visits have allowed patients to continue receiving care, while minimizing the exposure and risks associated with COVID-19 and other types of infections. However, telehealth usage has some limitations. The most obvious is that it does not allow regular physical examinations or in-person laboratory tests. 1 Less obvious is patients' low confidence and lack of trust in telehealth as a reasonable substitute for in-person clinic-based health care.
Telemedicine requires various medical devices, sensors, and imaging devices connected to an interface integrated with a smartphone or tablet to measure and communicate specific health indicators. While there has been a rush to obtain a fully integrated telemedicine solution for COVID-19, 2 there is considerable work associated with education for using these devices. Patients from racial and ethnic minority populations and those with low socioeconomic status have a higher likelihood of experiencing barriers to accessing telehealth services due to poor digital literacy, lack of adequate computer equipment, and reliable internet coverage, 3 and these barriers comprise the digital divide. 4 Digital access is now recognized as a social determinant of health. 5 It is estimated that over 21 million individuals in the United States (U.S.) lack broadband internet access and have limited access to telemedicine. 6 Existing concerns about the security of personal health information shared through virtual platforms remains a barrier for the widespread use of this technology. 7
Our safety net clinic predominantly serves underserved racial and ethnic minorities who may be uninsured, have low literacy, lack technology know-how and self-monitoring techniques, and do not normally trust government health care agencies. These clients are multilingual, have unique social norms and cultural beliefs, and as such health care providers require a culturally competent framework. For example, immigrants from Chinese, Vietnamese, and Filipino communities were more likely to strongly agree that it is better to take care of one's own health without outside interference. 8 Southeast Asian people have attitudes that when they experience suffering, it is their fate or destiny, and their life span is predetermined. 9 Cambodians believe that illness results from a spiritual imbalance. Asian Americans are twice as likely to use acupuncture and the services of traditional healers as Americans. However, based on our experience, such clients are willing to participate in remote patient monitoring (RPM), in their language of choice, utilizing a patient navigator of same ethnicity for a cultural and linguistically appropriate experience. 10 We present our experience with such clients.
The patient demographics for our clinic are shown in Table 1. These patients speak various languages: English 47%, Spanish 9%, Vietnamese 5%, Korean 6%, Chinese 4%, Arabic 5%, Burmese 6%, Russian 3%, Amharic 5%, Somali 2%, Nepali 5%, and other languages 3%. Therefore, it is necessary for support of various languages, cultural beliefs, and levels of literacy for an effective implementation of a telemedicine system.
Refugee Demographics Data Based on 1,250 Refugee Patients at Our Clinic from: Nepal, Vietnam, Myanmar or Burma, Ethiopia, and Mexico Settled in Metro-Denver Area Within Last 3 Years
From the patient's perspective, the primary aim of telemedicine is to increase their access to care and to enhance the convenience of accessing their provider. 11 It can bring care to patients who may have difficulty making appointments, such as people with language and cultural barriers, the elderly, the disabled, or those lacking sufficient transportation. It can significantly decrease the time it takes to receive medical care—travel time to health care facilities, waiting room time, and time to obtain medical care. It may also play a role in reducing health care costs for patients and even avoid costly emergency department visits or hospitalizations. 12
Methods
A VSee telehealth clinic software was set up on our server, and the client software is downloaded on a smartphone or tablet for remote use by the patient. Patients completed an online consent form customized for their language of choice with consideration of their literacy level. The case manager identified and completed the preappointment items. The provider follows the schedule, and at the time of appointment, a two-way video call is initiated. If necessary, an interpreter is added to the virtual telehealth call as a third person. We provide three examples of utilization involving some typical patients.
CASE 1
Thirty-six-year-old female has been a patient since January 2020 with Medicaid insurance. She experienced chronic pain due to trauma and has opioid dependence in remission. She has consulted for depression and received counseling for drug abuse. The provider consulted with her using VSee audio as she does not have ready access to a smart phone. Due to her disabling condition and inability to travel by herself to her clinic visit, telehealth consultation is necessary and no interpreter is necessary as she can speak English.
CASE 2
Fifty-four-year-old Spanish speaking female is uninsured and undocumented. She has a history of abnormal cholesterol or hyperlipidemia. A telehealth appointment was set up for her to discuss laboratory results. She is also pre-diabetic and required monitoring for diabetes along with the primary medical issue. VSee audio-video call was adequate for discussing her clinical data and then e-prescribing medicine at her pharmacy. She was educated on how to control her medical condition through diet, and exercise was provided. An interpreter was used to communicate with patient in Spanish as a three-person connection.
CASE 3
Thirty-year-old Mongolian female is uninsured and has symptoms of lower back pain. The provider conducted follow-up with her laboratory for her annual examination and explained the results during her virtual appointment. A Mongolian translator was used to communicate through a three-person connection.
From over 1,000 patients we sampled 498 patients who received telehealth services over a 12-month period for specific services, such as: Rx refill, consultation for laboratory results, wellness evaluation and education, and acute or sick visits with appropriate referrals. Data were captured about the race, ethnicity, type of medical condition, and whether an interpreter was required for these appointments. Results of language and category of service are shown in Figure 1, and it is clear that many multiethnic patients required interpretation. We then conducted an experiment that focused specifically on the treatment of diabetes using telemedicine and a culturally and linguistically appropriate telehealth protocol has been implemented for validating the efficacy of improving the glycemic control of patients.
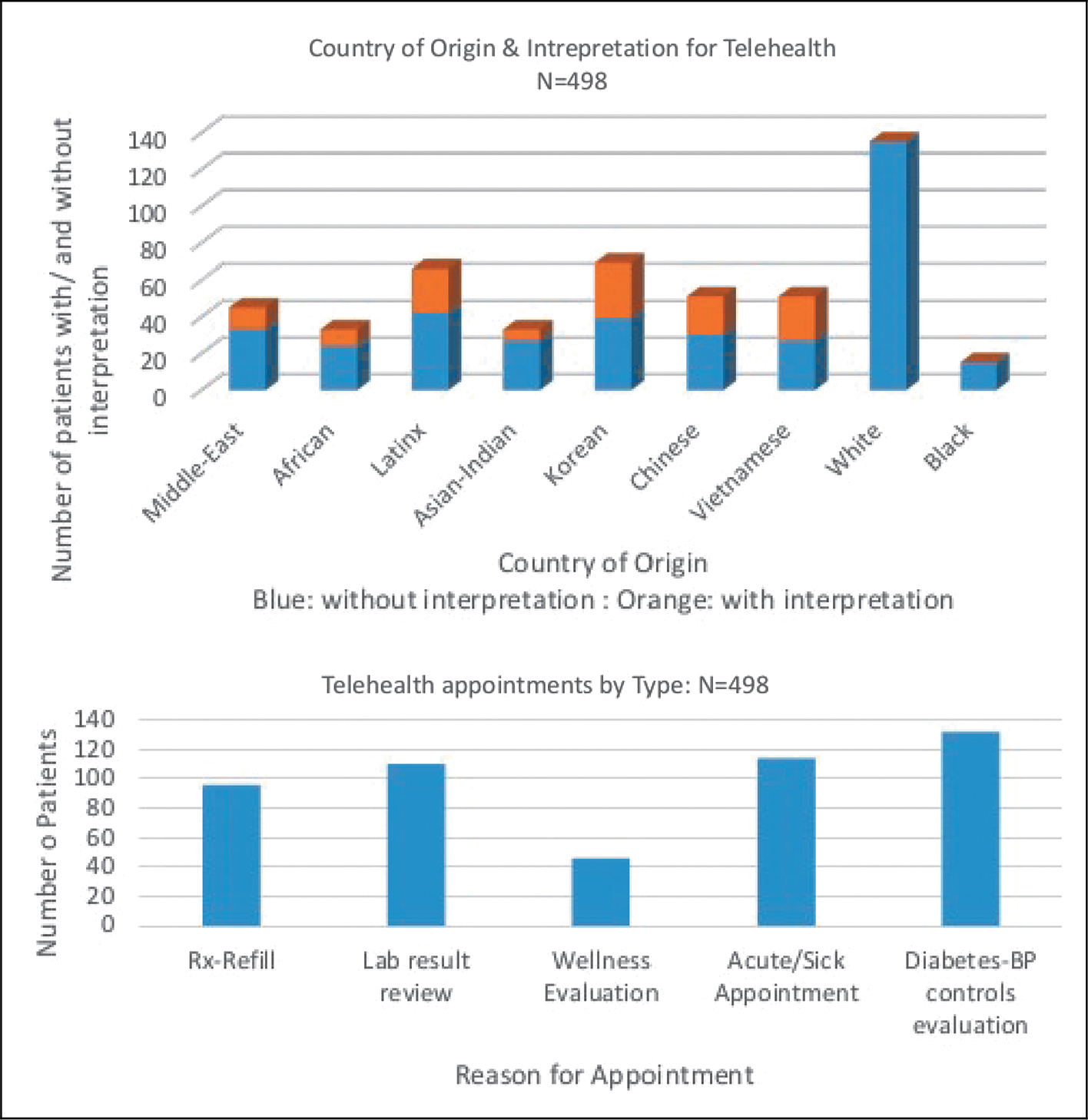
Telehealth appointments at the family medicine clinic.
Diabetes was selected based on results from a 2021 American Diabetes Association survey that showed that 68% of lower-income bracket and people of color are disproportionately affected by diabetes mellitus (DM). Approximately 28% of Americans with DM are undiagnosed, and another 86 million American adults have blood glucose levels that greatly increase their risk of developing type 2 DM over the next several years. 13 Minority populations are more likely to develop type 2 diabetes and constitute 25% of all adult patients with diabetes in the U.S. 14 Twenty one percent of adults with type 1 diabetes have never checked their blood sugar; 47% of insulin-treated type 2 diabetes patients were never monitored.
Typically, patients visit their doctors once every 4–8 weeks and a lot can happen at that time, and only 15% of patients bring daily logs of their blood-sugar measurements to these visits. Doctors may not hear significant issues until long after the fact, and it is easy for patients to forget details after several weeks. The pandemic adversely affected people with diabetes based on fact that 43% of people with diabetes have delayed seeking routine medical care during the pandemic. More than half of them cited their fear of COVID exposure, 15 and 73% of people with diabetes have used telehealth services during the pandemic, compared to only 11% before COVID-19. A small portion (32.5%) of 3,500 respondents living with type 1 or type 2 diabetes say that lack of access to reliable transportation affected their ability to receive diabetes care. 16 Figure 2 shows a flow diagram of the telehealth implementation for diabetes patients at our family practice clinic and its use for monitoring blood sugar in at-risk diabetes patients.
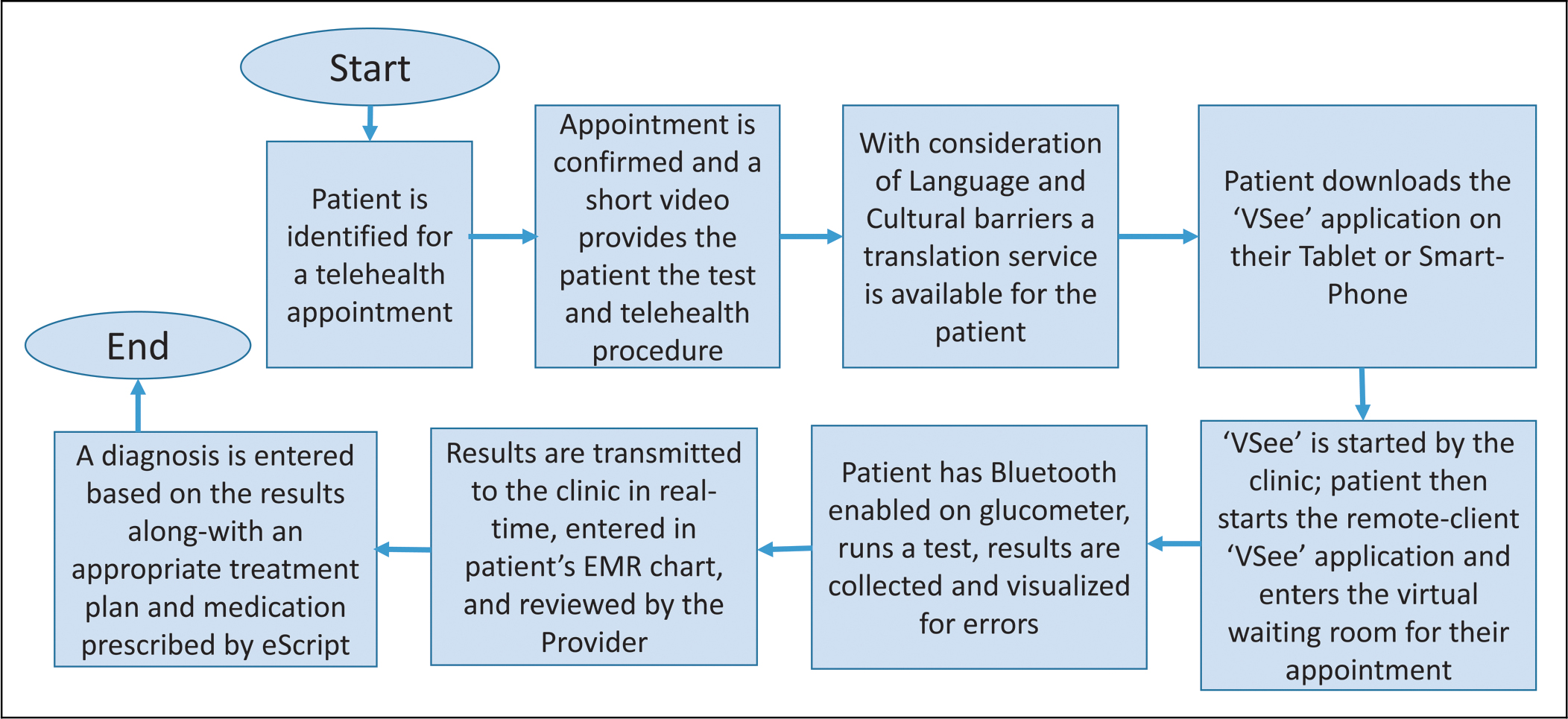
Process flow diagram for telehealth implementation for diabetes patients.
The experiment used the VSee telehealth platform and combined it with a Bluetooth-enabled “Contour” glucometer for patient with abnormal baseline Hemoglobin A1C (HgA1C) to record blood sugar value at predefined measurement intervals of a medically underserved migrant population. The project compared the mean HgA1C reduction rates at baseline and endpoint before and after intervention and compared it to a control group selected from existing patients of our clinic. The blood glucose result was taken and uploaded to a central telehealth system utilizing a hub-type remote monitoring device. The patients were educated on the use of this device in their homes so that they could report biometric data in real time. This intervention improved patient compliance with oral diabetic agents or insulin, blood glucose monitoring, and quality of diabetes self-care.
Initially, 70 patients were identified as eligible for participation in this project based on the inclusion criteria: a HgA1C level of 7% or higher obtained within the last 10 months. However, the collection of informed consent had to be stopped for 42 participants due to patient participation during the COVID-19 outbreak in the clinical facility. For a total of 42 participants who were identified with a baseline HgA1C level of 7% and above, 21 were randomized to each intervention and control group, and baseline data (HgA1C) and demographic data were collected. This experiment included patients with type 2 diabetes who migrated from over 13 countries. The majority of patients were 45–64 years old, representing 66.7% (n = 26) of all project participants; 59% were male and 41% were female. In addition, 53.8% of the total participants were Asian, and 20.5% were Black, 12.8% were non-Hispanic White, and 10.3% were Latinx. Approximately 43% of the participants reported earning <200% federal poverty level, 51% of the participants were unemployed, and 69% of the participants had Medicaid coverage. This project compared the improvement in HgA1C level at baseline and endpoint in the intervention and control groups. Each participant, randomized to the intervention group, was provided with a Bluetooth glucometer. Telehealth sessions for patients in the intervention group were provided individually for ∼20 min every week. Participants in the intervention group were encouraged to check their blood sugar level at least once a day, and if recommended by the provider, they checked their blood sugar level twice a day. Participants in the intervention group were encouraged to report their blood sugar levels through data files automatically generated by the Bluetooth glucometer smartphone application during individual telehealth sessions. A flow diagram showing various steps is shown in Figure 3.
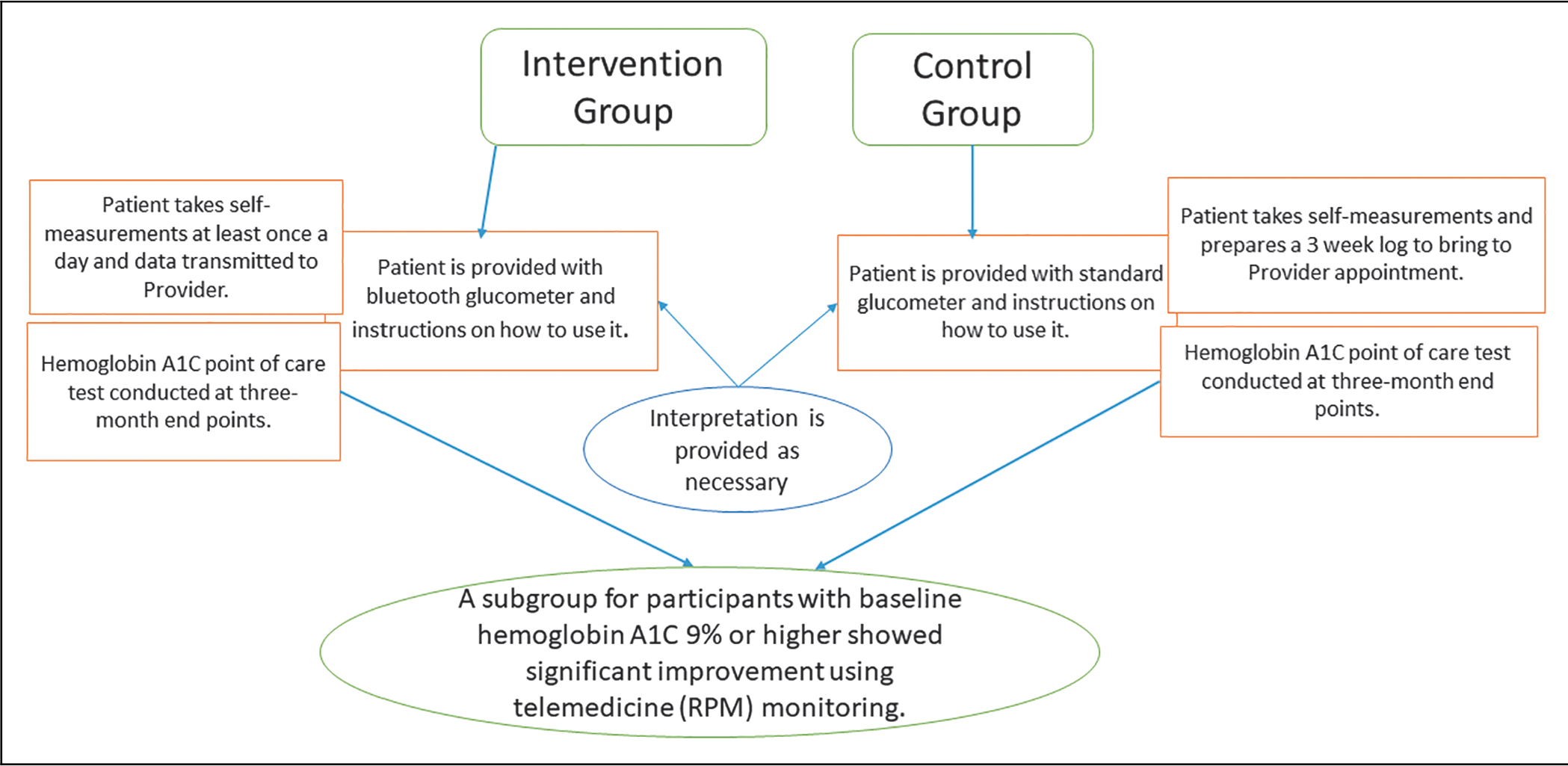
Flow diagram for intervention and outcomes.
Results
From numerous telehealth encounters we sampled 498 patients who received telehealth services over a 12-month period. Figure 1 shows the language services and health service categories.
For participants whose baseline HgA1C was 7% or higher, the mean of the reduction rates in HgA1C levels showed a significant difference between the intervention group and the control groups. It was quite apparent that these patients experience challenges in health care access due to cultural and language barriers. These medically underserved migrant populations rarely attempt to monitor their diabetes due to communication concerns caused by language barriers and, as such, defer their structured diabetic care management. The result of the two-tailed independent samples t-test was significant based on an alpha value of 0.05, t(11) = −2.67, p = 0.022, indicating that the mean reduction rates of baseline HgA1C from endpoint HgA1C levels were significantly different between the intervention group and control groups in the subgroup. 17 Figure 3 shows the workflow of the experiment consisting of an intervention and control group.
Conclusion
The implementation of a telemedicine service model for a well-defined group of underserved racial and ethnic minority patients at a Colorado safety-net primary care clinic was successful. These patients lacked prior knowledge of self-monitoring approaches along with language and cultural barriers that contributed to the health disparities for such patients. Our data suggested that with the introduction of continuously monitored virtual care there is the potential to increase quality and continuity of care. Such interventions show that telemedicine has the potential to become widely adopted and it can support various patient-wearable devices for the continuous tracking of vital signs that can minimize risk of chronic diseases such as diabetes, hypertension, and cardiovascular. We believe that such an intervention will also contribute to closing the digital divide for the vulnerable racial and ethnic minorities. Based on this project our clinic has now adopted RPM as a standard protocol for remote health care services and has also completed integration of asynchronous remote monitoring patient data with their electronic medical records.
Footnotes
Acknowledgments
The Family Medicine Clinic for Health Equity was involved in all aspects of the implementation of this project, and various students, volunteers, and co-authors directly contributed to this work.
Authors' Contributions
A.S.: conceptualization, methodology, telehealth infrastructure, writing, clinical site management. J.L.: statistics and hypothesis validation, patient selection and interaction. A.S.: data collection, data analysis, and telehealth equipment setup, reviewing, and editing.
Ethical Approval
Approved by the Institutional Review Board (IRB) of the College of Adult and Graduate Studies at Colorado Christian University, IORG# 0010176, IRB# IRB00012085, on September 9, 2020, through a full review.
Data Access Statement
Research data supporting this publication are available through email at admin@cahep.org
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from the Colorado Health Foundation and the Colorado Access.