
Abstract
Introduction:
The coronavirus disease 2019 (COVID-19) pandemic made it necessary to practice social distancing and limited in-person encounters in health care. These restrictions created alternative opportunities to enhance patient access to care in the ambulatory setting. We hypothesized that by transforming clinics into centers that prioritize procedures and transitioning ambulatory appointments to telehealth, we could establish a secure, streamlined, and productive method for providing patient care.
Methods:
Clinic templates were restructured to allow the use of the physical space to perform procedure-based clinics exclusively, while switching to virtual telemedicine for all nonprocedural encounters. Staff members were given specific roles to support one of the patient care modalities for a given day (Procedures vs. Telehealth). Performance and patient satisfaction metrics were collected between two periods of time defined as P1 (February–June 2019) and P2 Post-COVID (February–June 2020) and compared. These served as proxies of periods when the clinic workflow and templates were structured in the traditional versus the emerging way. Statistical analysis was performed using bivariate analyses.
Results:
The percentage of procedures performed among all in-person visits were higher in P2 compared to P1 (45% vs. 29%, p < 0.001). Although total charges and relative value units were lower in P2, the overall revenue generated was higher compared to P1 ($4,597,846 vs. $4,517,427$, respectively). This increase in revenue was mainly driven by the higher relative income generated by procedures. Patient experience, reflected through patient-reported outcomes, was more favorable in P2 where patients seemed more likely to “Recommend this provider office” (90% vs. 85.7%, p = 0.01), report improved “Access overall” (56% vs. 49%, p = 0.02), and felt they were “Moving through your visit overall” (59% vs. 51%, p = 0.007).
Conclusions:
Our data suggest that reorganizing urology clinics into a space that is centered around outpatient procedures can represent a model that improves the patient's access to care and clinical experience, while simultaneously improving operational financial strength. This efficient care model could be considered for many practice settings and drive high-value outpatient care.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has led to massive and catastrophic worldwide losses with greater than 93 million infected and over one million dead in the United States as of August 2022. 1 Pressures to provide socially distanced, safe medical care during the pandemic presented the significant challenge of balancing viral spread containment against continued delivery of outpatient care. These pressures led to digital technology tools being increasingly utilized in health care to maintain efficiency of health care services while maximizing patient safety. 2
Traditional outpatient surgical clinics are characterized by schedule templates that mix routine in-person visits for consultations and follow-ups with procedural visits. These visit types often require different patient encounter lengths and represent very different staff workflows. This heterogeneity of clinical work can lead to long patient wait times and patient satisfaction that falls short of expectations. During the onset of the COVID-19 pandemic, not only were crowded waiting rooms and clinic spaces no longer purely patient dissatisfiers but also considered high-risk settings for viral transmission. Wide adoption of telemedicine offered a mechanism to mitigating some of these concerns by keeping patients out of the clinic space. In urologic clinics, many visit types, including procedure visits and visits requiring a physical exam, necessitate in-person patient care which can't be accomplished with telemedicine. Patient survey data suggest that video visits are not a barrier toward shifting away from traditional in-person visits in terms of patient satisfaction. 3
Multiple studies have assessed the feasibility and efficiency of telemedicine in urology and its subspecialties before and after the COVID-19 pandemic onset. However, optimal workflows that preserve care quality for patients, providers, and staff as well as the operational financial strength for the medical practice have been under-studied. Here, we describe the impact of implementing a novel approach to providing urologic surgical outpatient care.
Methods
This was a case cohort study examining the impact of a new outpatient care model. The study was approved by the Institutional Review Board as consent exempt for publication as a quality improvement project with patient information collected in an aggregate and de-identified fashion.
Patient care visits at a single high volume academic multispecialty practice were categorized as telemedicine compatible versus requiring in-person care. Telemedicine was deemed acceptable for visits that included initial patient consultation, routine follow-up for review of test results or imaging studies, and pre- and postoperative counseling. Visits that required in-person patient visits included procedural visits (cystoscopy, transrectal ultrasound-guided prostate biopsy, urodynamics, vasectomy, etc.) and physical exam visits (pelvic exams, postoperative wound evaluations, postvoid residual measurement, etc.). The clinic workflows were reimagined such that providers would be scheduled for either telemedicine or in-person work on a given day. In-person scheduling templates were arranged to maximize the number of procedures performed in any assigned day. Staff were divided into teams whose role was to either support telemedicine patient care or in-person patient care. These workflows were implemented and measures of quality of care and clinical performance were measured.
Two study periods were defined—P1 spanned February to June 2019 before change in clinical workflows and P2 spanned February to June 2020 after the new care model was implemented. Outpatient productivity metrics were collected and extracted through the University of California, San Francisco (UCSF) Dashboard and Metric catalog. Productivity metrics included the total volume of visits as well as visit breakdown by type, percentage of slots booked overall and completed encounters. Productivity metrics also included “access to care data” reflected by the percentage of new patients booked and assessed for each period and the percentage of referrals scheduled within 5 and seen within 14 days. Financial strength was measured for the two periods by examining the total relative value units (RVUs), global charges, and payments for each period.
Finally, patient-reported outcomes related to their care experience were analyzed as measure of care quality and compared between the two periods using the Clinician and Group Consumer Assessment of Health Care Providers and Systems (CGCAHPS) and the PRESS-Ganey (PG) survey instruments. These instruments provide data generated by surveys randomly sent to a prespecified number of patients who come to the clinic for outpatient care during these two periods and reflect patients' experience and satisfaction.
Descriptive statistics were reported, and analysis was performed using the Chi-Square test for categorical variables and the Z-test for independent samples. All p-values were two-sided with p < 0.05 considered significant.
Results
The total volume of outpatient clinic visits decreased between P1 and P2 from 6,518 to 5,819 visits. Total visit breakdown and distribution are shown in Figure 1. In-person office visits decreased from 66% of total in period 1 (P1) to 28% in period 2 (P2), while telemedicine visits increased from 6% in P1 to 45% in P2. Although the total number of procedures performed decreased from 1,746 procedures in P1 to 1,310 procedures in P2, an increase in the percentage of procedures performed of the total number of office visits was observed from 29% in P1 to 45% in P2 (p < 0.01).
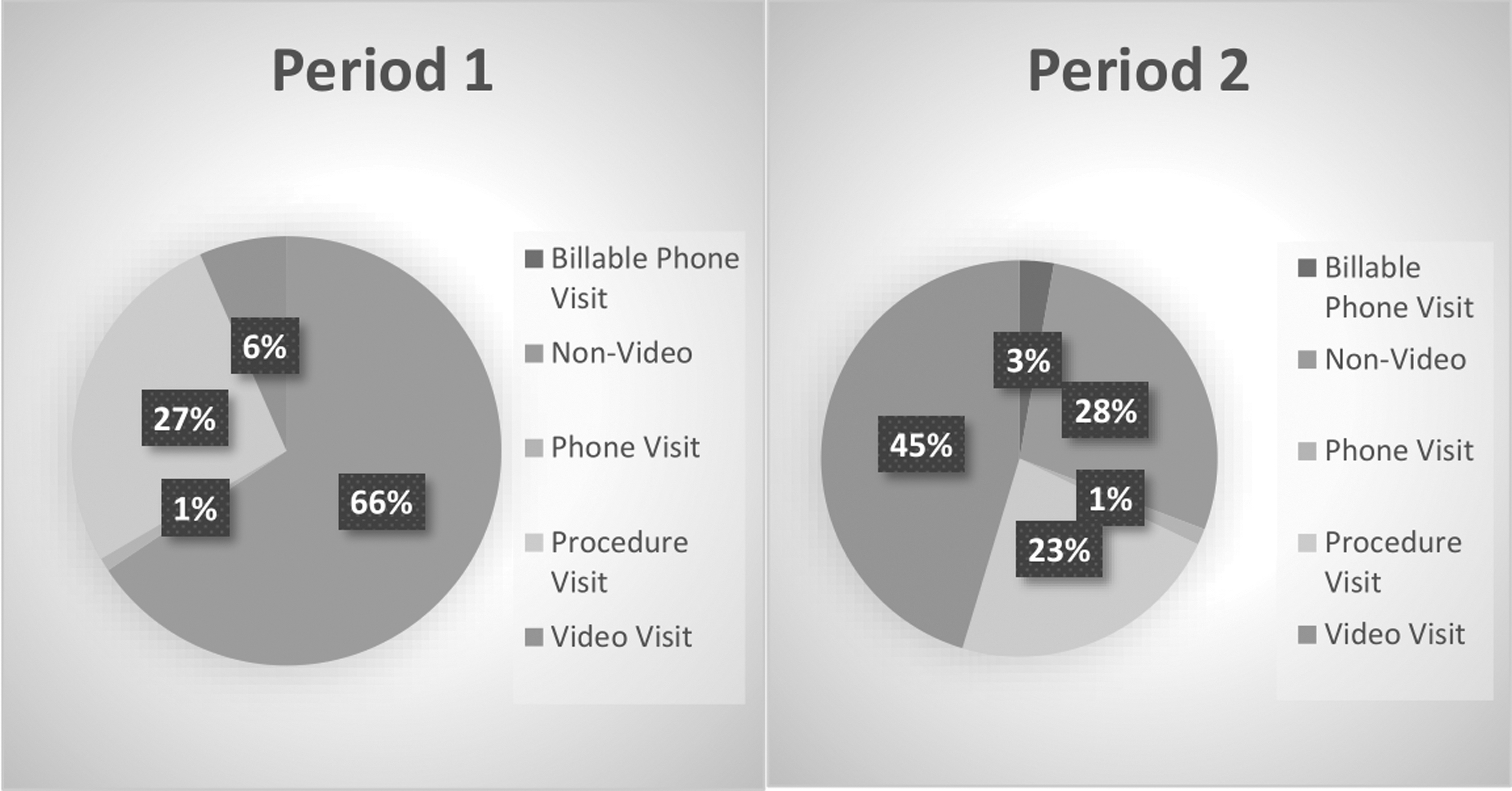
Outpatient visits breakdown by type of visit.
Additional productivity metrics are reported in Table 1. There was a statistically significant increase in the percentage of new patients scheduled within 14 days (46.1% in P1 vs. 70.6% in P2, p < 0.001) as well as the percentage of patients scheduled within 5 days (41.1% in P1 vs. 55% in P2, p < 0.001).
Outpatient Clinic Productivity Metrics and Access to Care Data
Bold text shows improvement in outcome (meaning values in P2 higher than P1).
Comparison of financial strength between the two periods identified an increase in total revenues during P2 compared to P1 ($4,597,846 vs. $4,517,427, respectively). This was accompanied by a decrease in the total charges (from 11,233,245 to 9,522,345) as well as the total generated RVUs (from 10,097 to 7,306) in P2. Financial strength metrics are broken down by type of visit in Table 2, demonstrating an increase in revenue generated by telemedicine visits and a decrease in revenue generated by in-person visits. Revenue generated by procedures increased by more than $400,000 despite fewer total procedure performed overall for the same period.
Financial Metrics Breakdown by Type of Visit
Bold text shows improvement in outcome (meaning values in P2 higher than P1).
wRVUs, work relative value units.
The types of procedures performed were compared between both periods; during P2, a higher number of urodynamic studies, bladder Botox injections, vasectomies, and Xiaflex injections were performed, generating a $488,000 increase in payments compared to P1.
Patient-reported outcomes improved for most of the CGCAHPS and PG scores domains during the pandemic (Tables 3 and 4). This improvement was statistically significantly increased for the CGCAHPS question “Recommend this provider office” (90% vs. 85.7%, p = 0.01), and the PG questions “Access overall” (56% vs. 49%, p = 0.02), and “Moving through your visit overall” (59% vs. 51%, p = 0.007).
Patient Reported Outcomes (Press-Ganey Score)
Italics represents significant p values.
Bold text shows improvement in outcome (meaning values in P2 higher than P1).
Average.
Patient Reported Outcomes (Clinician and Group Consumer Assessment of Health Care Providers and Systems)
Italics represents significant p values.
Bold text shows improvement in outcome (meaning values in P2 higher than P1).
Discussion
We describe herein a reimagined clinical care model that integrates leverages telemedicine to separate outpatient visits into in-person and telehealth work lanes for the providers, staff, and patients. These data examining the impact of this model at a high-volume large group subspecialty urology clinic demonstrated several favorable performance characteristics. This model performed comparably to the prior period in terms of productivity metrics, with significant increases in new patients seen within 14 days of referral (46.1% to 70.6%) and referral scheduling within 5 days (41.1% to 55%). Despite the decrease in total charges and RVUs, total revenues were higher with the new care model. Most importantly, superior patient satisfaction and quality of care was achieved based on patient-reported experience measures.
The concept of remote medicine and Telehealth is not a novel concept. In fact, the first article published on the matter dates to 1879 and was published in The Lancet, reporting on the potential use of telephone calls to reduce patient's visits. 4 Further development of available technologies pushed the field of Telehealth even more, from teleradiology and early video communications in the 1950s 5 to the high-speed telecommunication that is readily available today.
The global COVID-19 pandemic onset marked a new era of adoption for telemedicine. Before 2020, the most common application of telehealth was using video visits to assess follow-up with patients. Telehealth was also adopted in Telementorship, and the use of telehealth technology to help train clinical providers remotely. 6 Despite the lack of widespread use and adoption of telemedicine in urology, most prepandemic studies reported high levels of patient and provider satisfaction associated with virtual care. 6 Several challenges were identified as likely impediments against the widespread adoption of telemedicine including privacy, legal, and billing issues. 7 In 2020, the COVID-19 crisis led many urology practices across the United States to postpone or cancel many outpatient visits, as many urology clinic visits are not urgent. To contextualize our data, in this study, this was reflected by the lower number of overall visits during P2 and the higher proportion of video visits that were performed compared to the total number of visits. Telemedicine in a pandemic context offered an option to avoid interrupting outpatient clinical care while still minimizing unnecessary patient exposures and help reduce financial strains on clinical enterprises. 8,9
Our care model intervention leveraged telemedicine to create a model that optimized all visit types in the outpatient setting. These advantages are applicable regardless of pandemic status. We noted that the widespread adoption of telemedicine was associated with increased patient satisfaction. These results are in line with prior literature that assesses urologic patients' satisfaction with Telehealth including pediatric urology patients, patients with infertility, patients with genitourinary malignancies, and for patient follow-up after urethral sling placement. 10 –13 We hypothesize this effect to be related to multiple factors. First, patients with chronic conditions requiring frequent visits may be burdened by the commute to appointments, which may be logistically cumbersome and financially exhaustive due to indirect costs of transportation and parking. Second, senior individuals make up a significant portion of patients cared for by urologists, and these patients might need a caregiver to accompany them to the clinic resulting in lost wages. The same applies to pediatric patients who need to be accompanied by their parents. Third, this model could provide increased access to care not limited by geographic location. Fourth, expedient scheduling of newly referred patients with acute complaints would positively impact patient perspective and satisfaction. Finally, several studies have documented improved adherence to treatment and improved patient outcomes due to the ease of monitoring and regular care using telemedicine. 14 –16
While telemedicine was associated with many positive outcomes, the value of this care model was separating visit types per provider per day. This allowed the provider and staff to focus on one type of visit on a given day. Such focus allows for streamlining efficiency in the clinic. When shifting between clinic visits and procedure visits as is frequently done in a traditional care model, inefficiencies are created when rooms need to be set up for different types of care and team members attention can more easily be diverted to shift between procedures and other clinic visit types. When team members are focused on delivering one type of visit in a repetitive fashion, routine can be established that leads to efficiency. While not specifically studied, these efficiencies would also be expected to be associated with shorter patient waiting times in the clinic. The high proportion of procedures out of total visits was an important contributor to generating revenue, facilitating increased financial strength over the traditional care model.
LIMITATIONS
We acknowledge that the application of this new care model might be challenging outside of a large group practice type setting. Low-volume clinics might not be able to consolidate visit types into two groups to fill an entire day with either telemedicine or in-person procedural visits. Hence, generalizing this care model to different types of centers might require some level of adaptation. For example, one might imagine doing a half-day of telemedicine and a half-day of procedural visits to achieve the same advantages at a smaller scale.
Another limitation is that the improvement in patient's reported outcomes might not necessarily be related to the model itself but rather a reflection of patient's behavioral changes during a global pandemic, where a higher appreciation of medical care may have been intrinsic.
Conclusions
Our data suggest that reimagining physical urology clinics into a space that is mainly dedicated to outpatient procedures can represent a care model that improves patient access to care and clinical experience, as well as strategically bolstering financial strength. This care model may represent a future state of efficient, high-quality outpatient urology care.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.