
Abstract
Objective:
Increased utilization of e-health services can help to meet shortages of psychotherapeutic treatment. e-Health interventions can be effective if tailored according to the individual needs and demands of the target group. To gather comprehensive data for the development of a user-centered e-health intervention, a cross-sectional study was conducted among a heterogeneous cohort of 309 patients seeking treatment or consultation at psychosomatic university hospital in a densely populated region of Germany.
Methods:
Sociodemographic data, psychometric dimensions of mental burden, as well as needs and demands regarding an e-health intervention were assessed. A descriptive statistical analysis and a cluster analysis were performed to examine distribution of preferences and differences based on level of burden regarding needs and demands for e-health interventions.
Results:
Two hundred thirty-nine (N = 239) participants were included in the final data analysis. Among this primarily urban target group smartphone availability was favored by 77.8% of the participants. The cluster analysis revealed significant differences dependent on mental burden. 75.2% of participants with a high mental burden preferred longer interventions of 1–4 months compared with 49% in the low burden group, which also considered short interventions of up to 1 month (46%). Differences were also identified for content preferences and daily-life integration and were consistent irrespective of the initial reason for consultation.
Conclusion:
The findings of this study can provide a foundational framework for developing user-centered psychosomatic interventions. The potential relationship between individual burden and individual needs and demands highlights the crucial role of preliminary research to tailor interventions to effectively address diverse needs and preferences.
Introduction
The latest advancements in digital technology have brought a vast increase of private usage of digital web-based services. The majority of the worldwide population has access to electronic equipment and the internet. In 2020, 90% of the German population was using the internet, which highlights an increase of 15% for the past 10 years. 1 This presents a big opportunity for the health care system and, therefore, caused considerable political interest in developing e-health interventions national and international level. 2 e-Health can be defined as the usage of information and communication technologies (ICT), aiming for an improvement and facilitation in the health care system and health conditions. 3
There is an increasing availability of e-health services providing medical assessment, symptom management, and therapeutic treatment, 4 facilitating multimodal content combining text with audio, video, 5 or even virtual reality. 6 Some e-health services are already integrated in clinical practice and refundable by health care providers. On both a systemic and an individual level, e-health interventions and services offer numerous advantages, as they are not constrained by location or time and can overcome the obstacles typically associated with face-to-face interventions. 7 Furthermore, resources for face-to-face interventions in the health care system are limited, which lead to long waiting periods to access treatment. 8
Especially within psychotherapy, there is an alarming shortage of available support from professionals. 9 An increasing utilization of e-health services in psychotherapeutic treatment may provide not only faster access to professional support but also increase availability of treatment options to a greater number of people. 10
Evidence shows e-health interventions can reduce the severity of symptoms of different mental health disorders such as anxiety disorders, affective disorders, or eating disorders. Positive effects have also been identified on outcomes such as distress, stress level, negative affect, panic, and depression symptoms. 11 –13 In contrast, major limitations include participant attrition and lack of adherence, which have been the subject of research to improve effectiveness and acceptance of e-health interventions in the past two decades. 3,14 –18
In a systematic review of adherence in web-based interventions, Kelders et al. reported adherence rates for web-based interventions from as low as 10% to an average of 50%. 19 Therefore, it is essential to adjust the standards of these interventions to enhance adherence and improve overall usability, thereby ensuring that an application is utilized as intended by its creators. Moreover, it is essential to consider the needs and demands of patients in the development of need-based e-health interventions. 5
It has been shown that the involvement of a selected target group during the development process should be considered to improve acceptance and adherence among users. 19 –21 Joint dysfunctionality, describing the lack of connection between an e-health tool and health services, has also been identified to show negative effects for adherence among vulnerable groups. 5 It can be assumed that if an intervention does not consider the needs of the target group, the adherence will be lowered 17 and attrition rates will be high. Baines et al. have recently shown that due to stakeholders' availability, interests, and involvement with target groups, digital innovation often lacks involvement of patients in the early stages of design. 22
Objectives
This study aimed to investigate the needs and demands, as well as preferences regarding content, design, and framework for an e-health intervention to foster well-being in patients attending a psychosomatic university outpatient department. Patients were clustered and compared by psychometric characteristics to identify differences in the needs and demands for such an e-health intervention.
Methods
STUDY DESIGN AND PARTICIPANTS
Participants of this study were patients of the outpatient department of the Clinic for Psychosomatic Medicine and Psychotherapy of the LVR-University Hospital in Essen, Germany. The patients were seeking general psychosomatic outpatient consultation, consultation before undergoing bariatric surgery, psycho-oncological care, as well as treatment of eating disorders, psychosomatic disorders, or traumatic experiences. The digital assessment was administered through the platform PRO|M|SPACE. Recruitment was conducted from September 20, 2021 to November 8, 2021.
Eligibility requirements were age ≥18 years, sufficient German language skills, and internet access. Electronic informed consent was obtained before filling in the survey and participation was voluntary. The study was conducted in accordance with the Declaration of Helsinki and the Ethics Committee of the Essen Medical Faculty (18-8450-BO) approved the study.
MEASURES
Sociodemographic characteristics and medical history
Sociodemographic and medical data, including weight, height, and treatment history, as well as patients' wishes for future treatment, were assessed.
Psychometric characteristics
Different dimensions of mental burden as well as self-efficacy were assessed. Participants' distress in the past week were measured by the Distress Thermometer (DT), 23 which is scaled from 0 = “no distress” to 10 = “extreme distress.” Cutoff scores of 4 or higher indicate elevated distress. The Patient Health Questionnaire-8 (PHQ-8) 24 was used to measure depression symptoms on a 4-point Likert scale. A cutoff score of >10 indicates clinically relevant levels of depression symptoms. The internal consistency was high (α = 0.87).
Generalized anxiety symptoms were assessed by the Generalized Anxiety Disorder Scale-7 (GAD-7), 25 scaled on a 4-point Likert scale. Cutoff scores of 5, 10, and 15 indicate mild anxiety, moderate anxiety, and severe anxiety, respectively. In this sample, internal consistency was high (Cronbach's α = 0.9). The Insomnia Severity Index (ISI), 26 scaled on a 5-point Likert scale (0 = “not at all” to 4 = “very severe problem”), was applied to evaluate the severity of insomnia.
A cutoff score of 10 or higher indicates insomnia. Internal consistency was high in this sample (Cronbach's α = 0.87). The General Self-Efficacy Scale (GSE), 27 scaled on 4-point Likert scale, was used as a measurement of participants' self-efficacy expectations. In this sample, internal consistency was excellent (Cronbach's α = 0.91).
Needs and demands regarding an e-health intervention to promote well-being
Different aspects of needs and demands regarding an e-health intervention promoting well-being were assessed through multiple choice questions that were self-constructed by the research group and were based on previous research. 20,21,28 Participants responded to items concerning the availability, format, and aim of the e-health intervention. Furthermore, patients responded based on which recommendation they would consider the intervention trustworthy and which channels they would use to search for e-health interventions. In addition, preferred phase of use, context of use, duration of the intervention, frequency of new material, interval for notifications, and length of session were assessed.
Different topics (e.g., sleep problems) that should be addressed by the e-health intervention were assessed on a 5-point Likert scale (0 = “irrelevant” to 4 = “very relevant”). Participants were given the opportunity to provide further topics of interest.
STATISTICAL ANALYSES
Statistical analyses were performed using R (version 4.0.3). 29 Descriptive statistics in form of distributions, mean scores, and standard deviations (SDs) were performed. Sum scores for PHQ-8, GAD-7, ISI, and GSE were calculated. Cutoff scores were computed for DT, PHQ-8, GAD-7, and ISI. Relevant psychometric characteristics (PHQ-8, GAD-7, and ISI) were used to perform a cluster analysis. To evaluate the clustering tendency of the date, Hopkins' H statistic was used.
The cluster analysis was based on the k-medoids method for its robustness against outliers. The optimal number of clusters was identified (parameters package) 30 and a two-cluster analysis was performed. R 2 statistic was used to evaluate the model's overall cluster performance. The model's classifiability was investigated using linear discrimination analyses. Group comparisons between the clusters were conducted in form of t tests and χ 2 tests. The level of significance was set to α = 0.05 for all tests. Bonferroni correction was applied to control for multiple testing.
Results
STUDY POPULATION
Out of 309 patients who received the digital questionnaire during the time of recruitment (September 2021 to November 2021), 239 (77%) completed the questionnaire and were, therefore, included. Two hundred thirty-nine patients were included in the final data analyses, of which 70.9% (n = 168) identified as female. The mean age was M = 40.69 (SD = 13.23) years. The youngest participant was 18 years old and the oldest 73 years old. The majority of 71.5% (n = 171) came from urban areas (residency in a large city >100,000 residents). Patients were grouped by their self-provided initial reason for seeking treatment or consultation. Table 1 shows detailed sample characteristics.
Sociodemographic Data
PSYCHOMETRIC CHARACTERISTICS
In this population, 79.5% (n = 190) of the patients reached DT scores ≥4, indicating elevated distress in the past week. For depression symptoms, 59.8% (n = 143) of the participants reached PHQ-8 scores ≥10, indicating clinically relevant levels of depression symptoms. 31.4% (n = 75) of the patients reached GAD-7 scores ≥5, 21.8% (n = 52) responded with values ≥10, and 21.8% (n = 52) reached scores ≥15, indicating mild, moderate, and severe generalized anxiety symptoms, respectively. For the ISI scale, 71.1% (n = 170) of participants reached the cutoff score for insomnia (≥10). Table 2 gives an overview of psychometric characteristic by patient group.
Psychometric Characteristics by Patient Group
DT, Distress Thermometer, GAD-7, Generalized Anxiety Disorder Scale-7; GSE, General Self-Efficacy Scale; ISI, Insomnia Severity Index; PHQ-8, Patient Health Questionnaire-8; SD, standard deviation.
PATIENTs' NEEDS AND DEMANDS REGARDING E-HEALTH INTERVENTIONS
Most of the participants responded that e-health interventions should be available as a smartphone application. It should first of all provide psychoeducational information and skills training. The e-health intervention would be deemed trustworthy if recommended by experts (e.g., doctors or psychologists). When searching for an appropriate intervention the majority would contact an expert before using search engines. Most patients would prefer to use an e-health intervention after psychotherapeutic treatment. The preferences for the overall length of an e-health intervention and the length of one session of use were heterogenic among the cohort. For a detailed description of patients' needs regarding e-health interventions, see Table 3.
Patients' Needs and Demands Regarding e-Health Interventions
app, application.
TOPICS THAT SHOULD BE ADDRESSED BY E-HEALTH INTERVENTIONS
Based on the patient's responses, the most important topics that should be addressed by e-health interventions were Quality of life (73%, n = 175), Helplessness/overwhelm (73%, n = 174), and Self-worth/self-esteem (69%, n = 165). The least important topic according to this population was Faith/spirituality (52%, n = 125) and Sexuality/intimacy (33%, n = 80). Overall, 14 of the 16 topics were deemed important by at least 50% of the sample. See Figure 1 for all of participants' responses. Additional topics suggested by participants in form of open questions are supplied in the Supplementary Table S1.
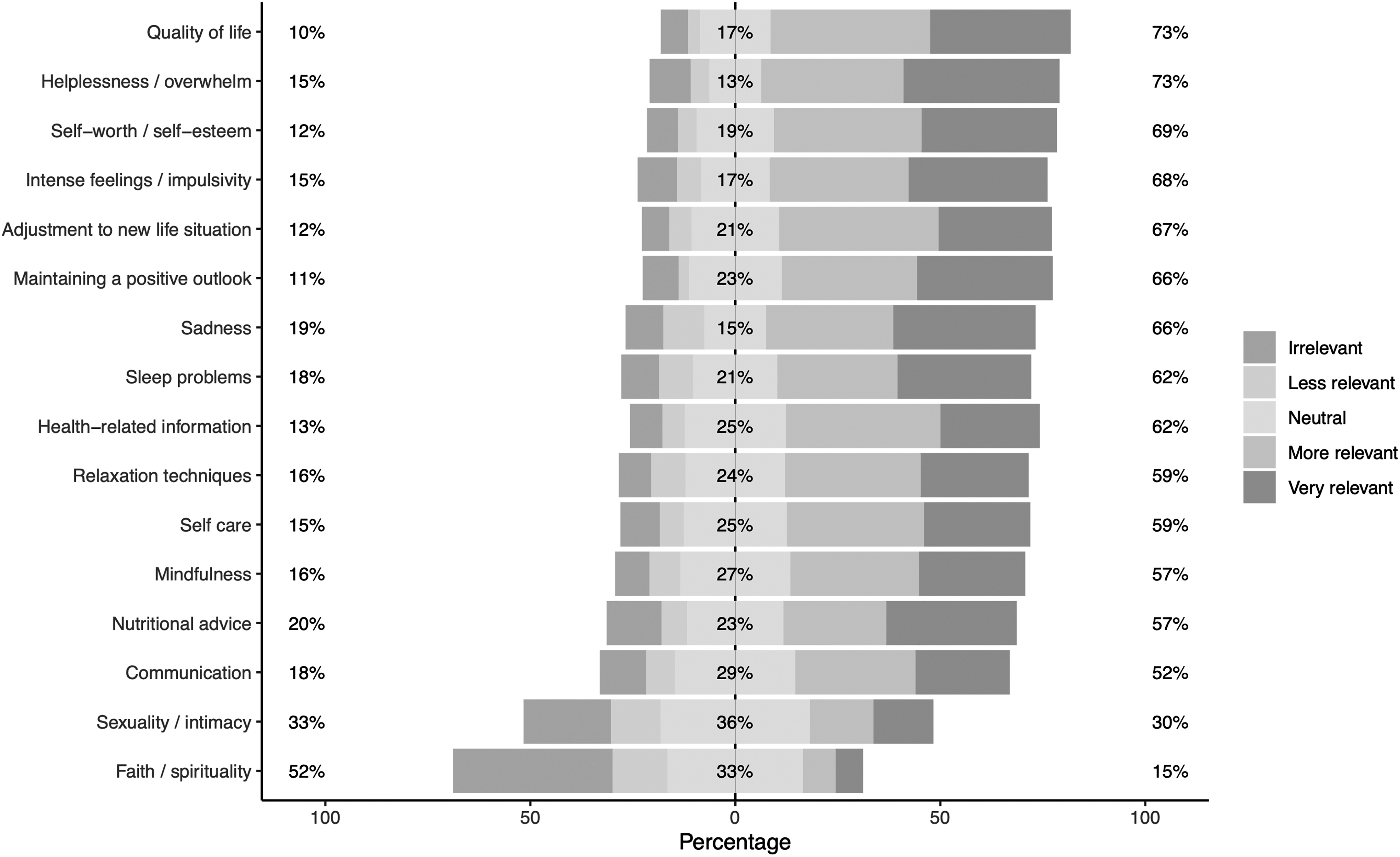
Topics that should be addressed by e-health interventions. Included as high-resolution image.
CLUSTER ANALYSIS AND GROUP DIFFERENCES BETWEEN CLUSTERS
Relevant psychometric properties (i.e., PHQ-8, GAD-7, and ISI) were chosen as foundation for the cluster analysis. The given data were suitable for clustering (Hopkins' H = 0.33). The choice of two clusters was supported by 14 out of 28 methods (50%). Therefore, a cluster analysis was performed based on the k-medoids algorithm. Modell performance was R 2 = 0.432 and overall accuracy of classification was 97.49%. The analysis resulted into two clusters, which can be interpreted as “high burden cluster” (n = 109) and “low burden cluster” (n = 130).
In the high burden cluster PHQ-8, GAD-7, and ISI were significantly higher than in the low burden cluster (p adj < 0.001). More detailed sociodemographic and psychometric characteristics of the two clusters can be found in the Supplementary Table S2. A visualization of the two clusters is shown in Figure 2.
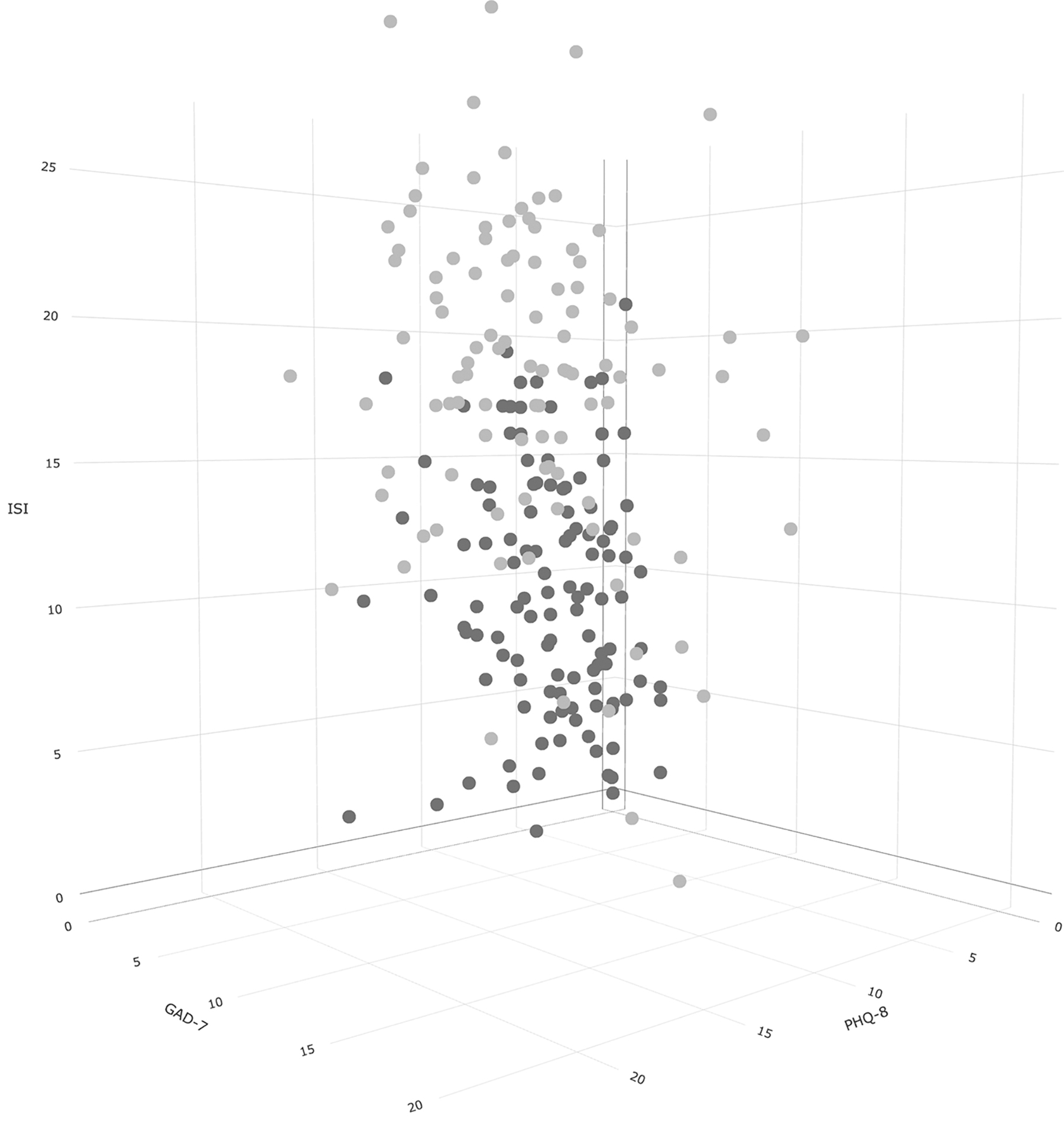
Visualization of the two clusters. Included as high-resolution image. Two-cluster solution of patients attending a psychosomatic outpatient clinic. GAD-7, Generalized Anxiety Disorder Scale-7; ISI, Insomnia Severity Index; PHQ-8, Patient Health Questionnaire-8.
Group comparisons of different needs and demands regarding e-health interventions revealed a significant association between cluster and preferred duration of use of the e-health intervention, χ 2 (4) = 23.16, p < 0.001. Although 75.2% of participants in the high burden cluster preferred a duration of at least 1 month up to 4 months, 46% of the participants in the low burden cluster preferred a duration of 1 week up to 1 month.
In the high burden cluster (n = 73, 67.0%) more participants agreed that the e-health intervention should support application in daily life compared with participants from the low burden cluster (n = 67, 51.5%), χ 2 (1) = 5.20, p = 0.023. For the high burden cluster (n = 49, 45.0%), positive responses toward the aim to give impulses for daily life were divided, whereas the low burden cluster (n = 41, 31.5%) responded more negatively to this aim, χ 2 (1) = 3.99, p = 0.046. More participants from the high burden cluster (n = 87, 79.8%) would consider an e-health intervention to be reliable if an expert would recommend it compared with the low burden cluster (n = 86, 66.2%), χ 2 (1) = 4.87, p = 0.027.
The high burden cluster deemed the following topics as significantly more important than the low burden cluster (p adj < 0.05): Sadness, Sleep problems, Intense feelings/impulsivity, Helplessness/overwhelm, Self-worth/self-esteem, Adjustment to new life situation, Maintaining a positive outlook, and Mindfulness.
Significant differences in burden were present among all patient groups (initial reason for consultation), ranging from 23% highly burdened participants in the “Bariatric surgery” group, to 65% in the “Eating disorder” group.
Discussion
As to our knowledge we are the first to identify and report content and format related preferences among patients attending a psychosomatic university outpatient clinic as a baseline assessment for an e-health intervention to improve well-being in this patient population. As expected, participants showed clinically relevant levels of distress, depression, and anxiety symptoms and, therefore, qualify as a potential target group for e-health interventions.
The vast majority (77.8%) considered the smartphone as most important channel of delivery, consistent with the high availability of smartphone devices in the general population and their frequency of usage 31 and in line with recent research. 20,21 A “mobile first” approach (meaning it is intended to be used primarily on a smartphone but can be used on other devices as well) can be beneficial and increase reach in everyday life, as smartphones are already part of everyday routines. 32
In addition, smartphones allow users to perform exercises and monitor symptoms immediately before and after crucial events. 33 Smartphones have smaller screens and typically lack physical keyboards, requiring intervention designs to account for these limitations. However, adopting a mobile-first approach allows for anticipation of future technological advancements (integrated biometric devices, smart watches, etc.) as implied by Baker et al. 34 Still, the usage on a desktop computer or laptop was deemed important by more than half of the participants. This reveals clear implications for multiplatform development strategies.
When asked for the aim of intervention, the majority expected it to “Provide information” (66.9%) or provide “Skills Training” (65.3%). Furthermore, “application in daily life” (58.6%) and “impulses for daily life” (37.7%) reached considerable approval rates.
The wish for audio/video formats or interactive content was indicated by participants in line with the findings of a meta-analysis by Arsenijevic et al. reporting multimodal content may increase intrinsic motivation. 5 However, overall format preferences varied among the participants, in general, which stresses implications by Baker et al. to recognize and address heterogenic demands of target groups. 22,34
Participants responded positively to nearly all of the 16 preselected topics that should be included in an e-health intervention. Therefore, it would be beneficial to incorporate optional modules based on cognitive-behavioral models, as suggested by Kim et al. 35
The highest trustworthiness concerning a recommendation for e-health Interventions is reached when it is given by an “expert” (89.5%) followed by governmental institutions (42.3%) and friends (36.8%). This is in line with previous research conducted in the field of acceptance regarding digital health interventions, which shows that social influence in terms of professional recommendation is important for the acceptance of e-health interventions in different fields. 21,36,37
It substantiates the necessity to involve health care professionals not only in distribution but also in development of the intervention as recommended by Baker et al. 34 In addition, integrating e-health directly into current clinical procedures could potentially enhance endorsement from health care providers and consequently result in greater approval and compliance rates.
The intended phase of use was assessed in acknowledgment of patients' current wish for face-to-face treatment and showed a slight bias toward the utilization after face-to-face treatment or at a later phase of treatment. Using an e-health intervention combined with in-person treatment received surprisingly low consideration. This finding can probably be explained by a perceived priority to consult a professional since participants were recruited from a group currently seeking face-to-face consultation. Another factor may be a difficulty to actually imagine blended care since it is rarely practiced outside of research.
Within the investigated population, two clusters could be identified as high or low burden according to PHQ-8, GAD-7, and ISI scores. Participants associated to the high burden cluster preferred longer durations and showed a more positive attitude toward daily life application, which may represent the self-perceived level of assistance that is deemed necessary to reduce burden and willingness to use supportive content to improve well-being. Highly burdened participants could be identified within each sociodemographic group, regardless of the initial reason for consultation.
These findings highlight the significance of conducting psychometric evaluations before developing an intervention, even when targeting well-established and distinct groups (such as patients with eating disorders). Previous research has indicated that burdened individuals express a greater intention to use e-health interventions. 38,39 Designing interventions with burden-adaptive content may enhance adherence and trust by addressing individual needs and demands.
LIMITATIONS
The results of this study should be interpreted considering the following limitations. Design implementations for a post-treatment e-health intervention should be further investigated since the results of this study do not identify needs after in- or outpatient psychotherapy since it was conducted before treatment. Participants were looking for further therapeutic evaluation or treatment when participating. Data were self-reported through digital questionnaires. The questionnaire that assessed needs and demands was created based on the expertise of the research group.
Since the sample was recruited in the outpatient department of our psychosomatic clinic, the sample should not be considered representative for the general population or people with mental illness in general. Furthermore, education level was higher compared with the general population and was mostly female. The majority of patients came from large cities in the vicinity of the hospital, which is located in a densely populated area in western Germany. Still, the sample represents a target group that could be addressed with an e-health intervention.
Conclusion
In summary, this study shows design and content-wise implications for an e-health intervention supporting patients attending a psychosomatic outpatient clinic to foster well-being. Our findings indicate that a compact e-health intervention, requiring <30 min per week and focusing on major topics, could receive high acceptance in a heterogenic group that seeks psychosomatic consultation or treatment. It should implement continuous development and quality analysis as suggested by previous research. 22,34
Furthermore, differences in needs linked to the individual amount of burden could be identified across multiple potential target groups, implying the need to develop interventions accordingly. Our findings can offer insights into basic needs of a particular target group of e-health interventions and, therefore, serve as a blueprint for first-stage development research of e-health applications.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
We thank the Open Access Fund of the University of Duisburg-Essen for supporting the publication of the article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.