
Abstract
Background:
The COVID-19 pandemic prompted the widespread adoption of telemedicine to deliver health care services while minimizing in-person contact. However, concerns persist regarding equitable access to telemedicine, especially for vulnerable populations. This study examines the utilization patterns of telemedicine by race in the United States, considering different modalities, medical specialties, and geographic regions.
Methods:
A comprehensive review of 26 articles published between January 2020 and August 2022 was conducted to analyze racial disparities in telemedicine use during the pandemic. Data from electronic health records and self-reported race were compiled for analysis. Variations based on geography, clinical care types, telemedicine modalities (audio or video), and study design were explored.
Results:
The findings indicate the presence of racial disparities in telemedicine utilization, with minority groups exhibiting lower usage rates compared with Whites. The location of outpatient clinics and clinical care types did not significantly influence telemedicine use by race. Among studies comparing telemedicine modalities, African Americans were more likely to choose audio/phone visits over video visits. Studies employing a pre-post design were less likely to identify disparities in telemedicine use by race.
Conclusions:
This study consistently demonstrates increasing racial disparities in telemedicine use. Future research should focus on identifying contributing factors and developing strategies to address these disparities. Policymakers should consider implementing initiatives promoting equitable access to telemedicine, including financial assistance, improved broadband infrastructure, and digital literacy programs. By addressing these barriers, telemedicine can play a crucial role in reducing health care disparities and improving access to care for all Americans.
Introduction
The delivery of health care underwent a substantial transformation due to the COVID-19 pandemic. With the need to minimize in-person interactions to reduce the spread of the virus, telemedicine emerged as a critical tool for providing medical care. 1,2 Telemedicine allows patients to consult with health care providers remotely, using videoconferencing, phone calls, or other forms of communication technology.
Telemedicine has long been promoted because of its potential to reduce a range of barriers typically present in usual care, including geographic (e.g., travel distances), temporal (e.g., travel and waiting time), financial (e.g., transportation and parking costs), and potentially cultural (e.g., privacy concerns) barriers. 3 There is a consensus that, before COVID-19, telemedicine had been underutilized in health care. 4,5 Also, before COVID-19, there were marked disparities in the availability of telemedicine, with telemedicine far less available to certain segments of the population, especially those who belong to vulnerable groups. 6,7 Even though telemedicine may now be more broadly available, there are still concerns that access to telemedicine is not equitable. Individuals might not use telemedicine because they cannot afford the technology, do not live in a geographic area with easy or consistent connectivity, or because they lack experience with technology—that is, they have poor digital literacy. 8 Furthermore, those with less trust in the health care system might be more reluctant to use telemedicine. 9
Very early in the epidemic, many were already concerned that existing racial disparities might increase with the greater use of telemedicine. 6,10 To examine this premise, we examined the literature, looking for patterns in service use by race. We aimed to understand whether racial differences appear to vary by type of telemedicine (specifically, video vs. audio/phone), by medical specialty, and by geographic region of the United States.
Methods
Our aim was to gain an overview of reports related to racial differences in the expanded telemedicine use during the COVID-19 epidemic. We did not intend to conduct a formal systematic review, a meta-analysis, a critique of study designs, or an assessment of the strength of the evidence in each report. Rather, our goal was to look for overall patterns in findings.
INCLUSION CRITERIA
To select articles, we first narrowed dates to those published between January 2020 and August 2022. We used the search terms “telemedicine,” “racial disparities,” and “COVID-19” on the PubMed and Embase databases to identify relevant articles. From the initial 72 articles identified, we narrowed the search to include only those that discussed outpatient service use, were from the U.S. health care system, and included information on race. We did not exclude articles based on the type of medical care provided, study design, or geographic location. Since one of our interests was to examine differences between telemedicine delivered in real time by video and telemedicine delivered by phone, we did not include articles that defined telemedicine as use of a patient portal, as a virtual hospital, or described asynchronous video visits. When articles did not specify a particular modality, we attempted to contact the authors to clarify and then eliminated articles where the modality was not specified. After applying these inclusion and exclusion criteria, we had 23 articles. We then reviewed the citations in each of these articles and identified 3 more articles that met our criteria, for a total of 26 articles.
IDENTIFYING PATTERNS
We compiled an inclusive table displaying various characteristics of the 26 studies (refer to Table 1). Data from each study were collected and subjected to thorough analysis, in most cases, from electronic health records where race was usually self-reported. We then used the table to look empirically at the categories of interest: geographic location of the study, type of clinical care where telemedicine was used, modality of telemedicine (audio or video), and study design. We looked for differences related to geography using several different ways to categorize studies in terms of where they were conducted, for example, using two groups (eastern United States vs. western United States; northern United States vs. southern United States) and four regional groups (East, West, Midwest, and South).
Studies Included in the Review
Racial groups abbreviation: AA, African American; AI, American Indian; AN, Alaska Native; AS, Asian; H, Hispanic; NH, Native Hawaiian; PI, Pacific Islander; W, White.
YOP, Year of Publication.
We also considered the type of clinical care, trying various ways of categorizing clinical care, and finally arriving at the categories of primary care (e.g., general medical, pediatrics, emergency room), surgery (e.g., general surgery and orthopedics), and specialty care (e.g., HIV care, ophthalmology, dermatology). To examine the potential effect of design, we compared those articles describing service use within a single cross-sectional cohort with those articles comparing two cohorts, pre- and post-COVID.
Results
OVERALL
Table 1 shows the racial categories used for each study. Since most of these reports were derived from electronic medical records, and the distribution of racial groups varies across the United States, the races in each study also varied, consisting of those who sought care at those sites. Every study included Whites and African Americans, and some also included Hispanic and Asians patients. Eight of the studies reported on a wider range of racial groups. White race was typically the comparator group.
Of the 26 studies included in our sample, 22 studies (84%) found differences in telemedicine use by race post-COVID, 4 studies (15%) noted no differences, 1 study found relative increase in use by African Americans, and 1 study found mixed results, that is, increased use by African Americans but decreased use by Hispanics.
As shown in Table 1, African Americans and Whites were included in all the studies. All but two of the studies included in our review found that African Americans either used fewer telemedicine services or their use of telemedicine did not differ from other groups. Two studies found that African Americans used more telemedicine. 11,12 Hispanics were included in 21 of the 26 studies in our review; 13 of these (about 2/3) found less use of telemedicine among Hispanics relative to other groups. Asian Americans were included in 12 studies, and 8 of these (about 2/3) found decreased use of telemedicine among Asian Americans.
Among the studies finding that those in minoritized groups were less likely to use telemedicine, in most cases, the disparities in use of telemedicine occurred between Whites and persons of color. As shown in Table 1, where there was a difference in use, with few exceptions, 11 –13 African Americans were included in those racial groups less likely to use telemedicine. In a few studies that involved larger populations and a variety of racial/ethnic groups, there were some more granular differences across races. For example, in the study by Weber et al., 14 conducted in New York City, less telemedicine use was common for both African Americans and Hispanics compared with Asian and White patients. Where the general population included relatively small numbers of a minoritized group, the number of patients in the data may have been too small to detect differences. For example, the study by Luo et al. 15 used data from Wisconsin and found that Asian and Latino patients were less likely than Whites and African Americans to use telemedicine; however, only a small portion of the patients (4%) were Hispanics.
LOCATION OF OUTPATIENT CLINICS
The 26 articles we examined were conducted in outpatient settings across the United States, usually at an academic medical center. Academic medical centers frequently draw patients from a wide geographic area, encompassing catchment areas that extend beyond the city in which they are located and where the investigations are conducted. Therefore, while Table 1 may list only one city under “sites,” the actual patients who appear in the data usually resided not only in that city but also in the surrounding areas, sometimes even extending into neighboring states. Of the 26 articles, only 1 article included a nationwide sample, a study of military veterans, the only study specifically of veterans. 16 George et al. examined data from a system of rheumatology clinics across 27 states, 17 whereas Rodriguez et al. included outpatient visits across 6 New England states. 18
Of the remaining 23 studies, 4 studies were conducted in the South (Texas, Tennessee, Alabama, North Carolina); 13,19 –21 9 were conducted on the east coast (New York, Connecticut, Maryland, Massachusetts, Washington DC); 11,12,14,18,22 –26 4 were in the West (California, Colorado); 27 –30 and 6 were in the middle of the country (Illinois, Ohio, Minnesota, Missouri, Wisconsin). 15,31 –35 Only a few studies 16,17,20,33,35 included samples from rural areas and commented on any differences related to rural residence. Examining the data in our table empirically, we did not note any apparent differences in race across these locations, regardless of how we categorized the sites. Figure 1 shows the map of the United States demonstrating the locations where the studies were conducted.
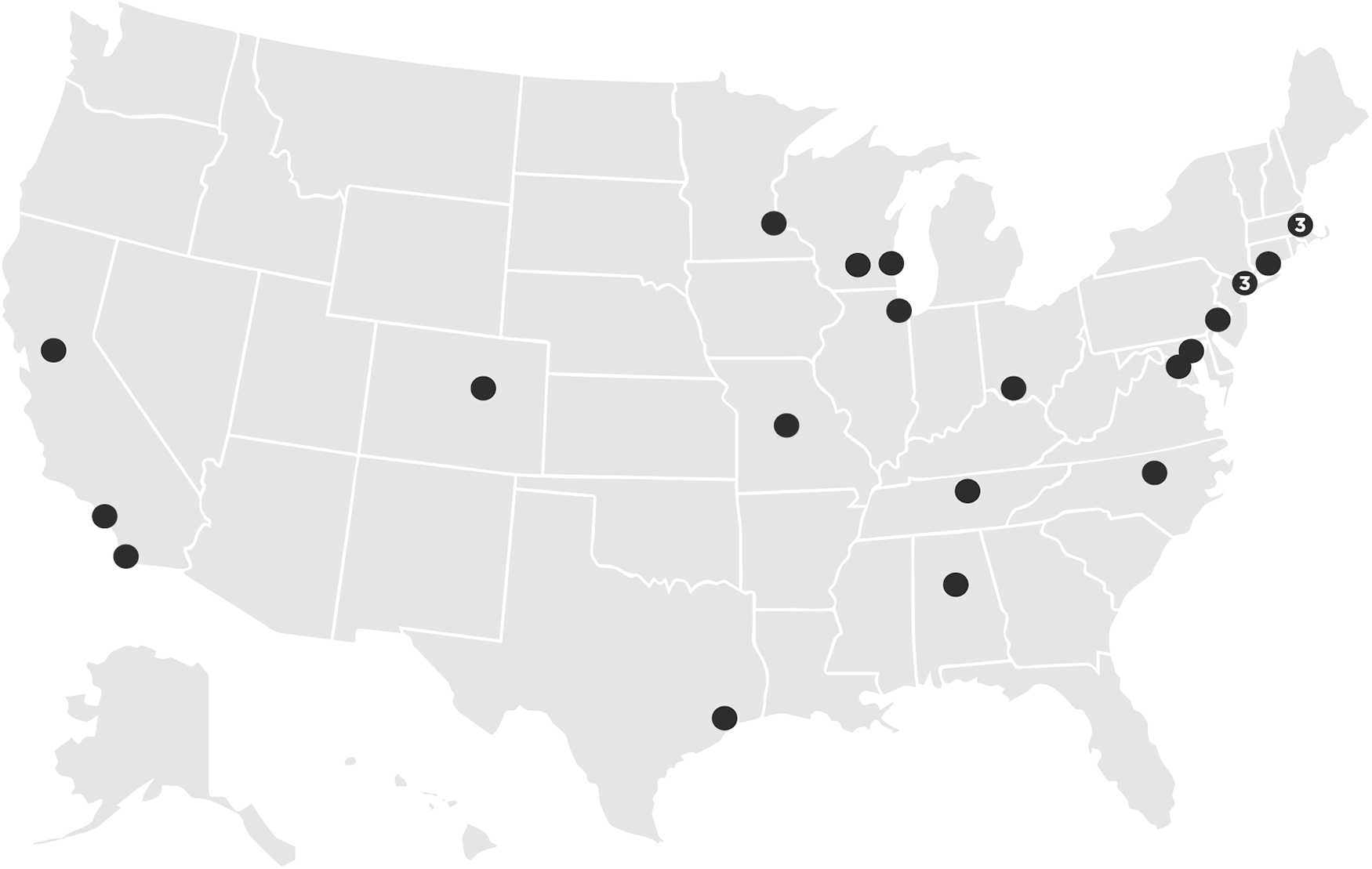
The U.S. map outlining the locations of studies included in this review. Ferguson et al. and George et al. are excluded from the map. Ferguson et al. conducted a nationwide study, whereas George et al. included 27 states.
TYPES OF CLINICAL SETTINGS
A range of types of medical care was represented in this sample. Ten studies were conducted in general medical, urgent care, or pediatric clinics; 11 were conducted in medical specialty settings, such as HIV, oncology, and ophthalmology; and 2 were in general surgical or orthopedic clinics. One report included only patients with COVID-19, and two reports provided information about patients with diabetes only. In empirically examining these data, differences in service use by race did not appear to vary by the type of medical care.
MODALITIES OF TELEMEDICINE
Of the 26 articles included in our sample, 11 articles (about 42%) examined only televideo, and the remainder included both video and audio/phone visits. Of those 12 reports including video and audio visits, 4 articles analyzed audio and video use combined, whereas the remaining 11 articles used compared those who used video with those who used audio.
Among the 11 articles that compared video and audio, 7 articles (64%) found that some groups were more likely to use audio than video, usually African Americans, 20,24,25,33 but sometimes, Latinx 11 or both 34,36 were more likely to use phones compared with video for distance connections. These authors all noted that the disallowance of phone-based telemedicine post-COVID would likely disproportionately and detrimentally impact these racial groups. In fact, a study not included in our review, 37 because it examined phone use exclusively, found that for postpartum care when audio visits were allowed during COVID, disparities based on race actually decreased rather than increased.
DATA AND DESIGN ISSUES
Most articles predominantly relied on clinical electronic medical records for data analysis, whereas only a single article 20 utilized claims data. Most researchers used visits as the unit of analysis, but a few used unique patients 14,15,25,28,30,36 rather than visits. Sample sizes varied widely, from more than 5 million visits in the national Veterans' study to only 190 visits in Geriatric clinic. Excluding the very large sample in the Veteran study and the smallest study analyzing visits, the mean sample size was about 125,990 visits and the median was about 31,331 visits. Most investigators used a cross-sectional design of a cohort of service users after the onset of COVID-19 and described differences in service use by race. Others used a pre-post COVID-19 design comparing two cohorts of service users, one before and a second after the onset of the COVID-19 epidemic. A few articles described service use over time. 11,12,17,21,23,25,30,31 None were truly longitudinal in nature, meaning that no study tracked the same patients over an extended period of time.
As shown in Table 1, there appeared to be an effect of design across these studies. Studies using a pre-post design were less likely to find a disparity in use by race.
Discussion
Our review of 24 studies on the utilization of telemedicine services and racial differences in health care service use shows that, despite the potential benefits of telemedicine, there are legitimate concerns about equity in use of telemedicine services for racial and ethnic minority groups. Two studies found that African Americans used more telemedicine. Regarding these outliers, it is possible that the study by Hayrapetian et al. did not find a difference because the researchers used a broader definition of “telemedicine,” i.e., they included all types of e-messaging, which may have allowed more access for African Americans than the other studies in our review. In studies that included Hispanics, about 2/3 found less use by that race. Similarly, in about 2/3 of studies including Asian Americans used less telemedicine. Since American Indians, Alaska Natives, and Pacific Islanders were included in only a few studies, and even in those studies comprised small sample sizes, it may be unwise to draw conclusions about these populations' telemedicine use from this review.
Taken together, the studies we examined were conducted across the United States. Even though all states were not included, there was reasonably good representation of different geographic regions. Likewise, our findings of racial differences in use of telemedicine service seem to hold true regardless of the type of medical care provided. Therefore, concerns about inequities in use appear to be valid across all geographic areas of the United States and across all types of medical services.
One of our key findings may have important policy implications. That is, we found that when audio visits were allowed post-COVID, racial differences in use of telemedicine services were often decreased rather than increased. This might be explained in that the vast majority of the population, including those with fewer resources, have access to telephones, whereas access to video telemedicine may be more restricted to those with more resources and better digital literacy. The comparison of these two types of telemedicine use was made possible because of the reductions of policy constraints on medical care provision that occurred due to COVID. Insurance companies and states are now in the process of putting prior policies in place again. Video telemedicine use is likely to remain as a reimbursable service, whereas audio visits are less likely to be allowed. 38 This policy change could have a marked impact on those who were using audio visits during COVID—African American and, to some extent, Latinx patients.
We found that studies that compared two cross-sectional samples were less likely to find differences in service use by race than those examining differences only within one post-COVID sample. One possible explanation for this could be that persons less familiar with technology or digital platforms may have improved their digital literacy over time with continued use of, and practice with, these modalities. Recent studies have indeed found that willingness to use telemedicine has increased from 50% in February 2019 to 62% in March 2021 and that the greatest increase in willingness is reported by non-Hispanic White, and non-Hispanic American Indian or Alaska Native adults were more likely to use telemedicine compared with Hispanic, non-Hispanic Black, and non-Hispanic Asian adults. 9,39
Therefore, it is possible that if and as telemedicine continues to be utilized in routine care, the differences in service use by race may attenuate. The COVID-19 epidemic has forced those within health care systems as well as patients to become far more proficient in using telemedicine technology, and, in effect, forced a broad adoption of telemedicine—something that might not have happened otherwise. This can pave the way for better access to care. Assuring that all persons have access to telemedicine and can use the technology should be a priority.
Our review has many limitations. We primarily utilized PubMed and Embase due to their extensive coverage of medical literature, but, other than that, we had no logical reason for selecting these. Most of the research was conducted at academic medical centers where, it can be argued, medical care may be somewhat different from care-as-usual offered in the community. It is also important to note that we did not conduct a formal systematic review or a meta-analysis. The authors whose articles we reviewed in general used descriptive, not experimental, designs and a variety of approaches to analyze data. A more rigorous review might have resulted in different findings. At the same time, it is perhaps even more remarkable that, despite these differences, an overall pattern of increasing racial disparities with telemedicine is very clear.
Further research is needed to better understand the factors contributing to racial disparities in telemedicine use and to identify strategies to overcome these disparities. Policymakers should also consider developing policies and programs to promote equitable access to telemedicine services, particularly for vulnerable populations such as racial/ethnic minorities. Such policies could include providing financial assistance to patients who cannot afford technology, improving broadband infrastructure in rural areas, and promoting digital literacy among underserved communities. By addressing these barriers, telemedicine could become a truly valuable tool in service of reducing health care disparities and improving access to care for all Americans.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for the completion of this work. The research was conducted without the support of any external funding agency or institution.