
Abstract
Introduction:
The ability to access telepsychiatry through audio–video technology versus audio-only (telephone) technology potentially leads to inequitable outcomes. This study examines the characteristics of patients who relied on the telephone to complete outpatient telepsychiatry visits in a large health system.
Methods:
This is a retrospective analysis of all telepsychiatry outpatient visits conducted from May 1, 2020, to December 31, 2021. Demographic, clinical, and socioeconomic factors were extracted from the electronic health record. Two-sample t tests were used for continuous variables and χ2 tests for categorical variables for bivariate analyses. Multiple logistic regression was used to examine the association between only telephone visits and all input variables.
Results:
Eight hundred ninety-four (8.9%) patients completed all visits only by telephone during the study period. In bivariate analyses, factors associated with telephone-only visits included male sex, non-English primary language, Black race, unmarried status, non-Hispanic ethnicity, older age, Medicare enrollment, uninsured status, and higher social vulnerability index (SVI). Psychiatric diagnoses associated with only telephone visits included substance use disorders and psychotic disorders. In multivariate analyses, factors associated with higher odds of only telephone visits included older age, inactive patient portal, comorbid diabetes, higher SVI, and higher broadband adoption. Psychiatric diagnoses associated with higher odds of completing only telephone visits included psychotic disorders, substance use disorders, or intellectual/developmental disabilities.
Conclusions:
Several patient-level factors are associated with a reliance on the telephone to complete telepsychiatry appointments.
Introduction
Telepsychiatry, defined as the use of virtual technology to deliver psychology or psychiatry services, has been shown to be equivalent or superior to certain types of in-person behavioral health care. 1 –5 The use of telepsychiatry expanded dramatically at the onset of the SARS-CoV-2 (COVID-19) pandemic, and this modality may now account for 50% of all behavioral health visits in the United States. 6 While access to telepsychiatry services has been crucial for many patients during COVID-19, access to services may not be equal to all. Certain populations may utilize telepsychiatry at different rates for various reasons, including stigma, access to technology, access to internet/data, digital literacy, or personal preference.
For example, older age, Asian race, non-English preferred language, and Medicaid insurance have been associated with fewer telemedicine visits. 7 In addition, the specific modality of how patients access telemedicine may differ as older age, female sex, Black race, Latinx ethnicity, and lower household income have been associated with lower use of video technology for telehealth visits. 7 –10 However, others have suggested that appropriate use of telehealth technology may help to reduce bias and help address some mental health equity concerns. 11
To the best of our knowledge, no analysis has occurred specifically for any factors associated with the usage of different modalities for telepsychiatry visits. Such an analysis is an important first step to understanding any effects on mental health equity that may occur as a result of reliance on telepsychiatry. In this study, we present an analysis of telepsychiatry outpatient visit data from a large, academic medical system to determine what factors are associated with reliance on telephone for telepsychiatry visits compared with the usage of video technology.
Methods
This retrospective observational study investigated the characteristics of patients of all ages who virtually visited the mental health clinics of a large, academic health system during the COVID-19 pandemic. Specifically, the study compared patients who used only telephones for their virtual visits with those who used video. The University of North Carolina (UNC) Health is the academic health system for the School of Medicine at the University of North Carolina-Chapel Hill. The Department of Psychiatry contains more than 400 clinical and research faculty and 95 clinical trainees (psychiatric medical residents and psychology interns). Like many others, the department went to a largely virtual treatment model for outpatient visits following the onset of the COVID-19 pandemic. The study was reviewed and deemed to be exempt by the institutional review board of the University of North Carolina-Chapel Hill.
The structured data of all mental health visits to UNC Psychiatry clinics from May 1, 2020, to December 31, 2021 were extracted from the UNC Clinical Data Warehouse, a data repository that hosts historical clinical, research, and administrative data harvested from the electronic health record system at the UNC Health. Completed visits only were included in the analyses. Visits completed by nonbehavioral health providers represented a tiny fraction of all visits and were excluded. Based on the description in the field “visit type” of a visit, the study coded a visit as a telephone visit if the keyword “telephone” was present in the description and a video visit if the keyword “video” was used in the description.
Due to the limited use of virtual care before the onset of the COVID-19 pandemic, the data were restricted to visits occurring after May 1, 2020. While video visits were technically possible between March 16 and May 1, 2020, many practitioners chose to use telephone appointments due to a lack of training and access to an approved video visit platform. However, by May 1, all providers at the institution had access to and had been trained on a video visit platform. The data set analyzed thus reflects more on the autonomous decisions of the patients and providers and less on technological readiness of the providers.
The outcome variable of the study is whether a patient used exclusively telephone or video for telepsychiatry visits. To assign a patient to either group, we aggregated the visit data at the patient level. If a patient had only telephone visits during the period, then the patient was designated as “telephone visit only.” If a patient had only video visits during the period, then the patient was designated as “video visit only.” If patients had both telephone and video visits or video visits only during the period, the patient was designated as “telephone and video visits.” We assumed that individuals who completed telephone visits only were unable to complete video visits for largely technical reasons (no device, lack of internet access/mobile data, no private space to conduct a visit, poor digital literacy, etc.), whereas individuals who had both video and telephone visits were likely able to complete video visits but chose to complete telephone visits due to personal choice, convenience, or provider/health system preference.
For the primary analyses, we compared individuals in the “telephone visit only” group with those in the “video visit only” group. We also conducted a secondary sensitivity analysis to test our assumptions, where we compared those patients in the “telephone visit only” group with those in the “telephone and video visits” group. To examine any differences in virtual visit modality completion by provider type, the following groups were used: physicians (MD and DO), advanced practice providers (PMHNP, FNP, PA-C), psychologists (PhD, PsyD), and therapists (LCSW, LCSW-A, LCAS, LCMHC, LMFT, MSW). The percentage of virtual visits completed by telephone was calculated for each group.
To understand the impact of demographic, clinical, rurality, administrative, social determinants of health, insurance, and broadband factors on patients' modality of virtual visits, we included a number of demographic, clinical, and internet access variables. These variables included age, gender, race, ethnicity, marital status, patient portal activation status, social vulnerability index (SVI),
12
geographic area (rural vs. urban as defined by the North Carolina Department of Health and Human Services:
Descriptive statistics were performed on all variables of interest. The study used two-sample t tests for continuous variables and χ 2 tests for categorical variables for the comparison of the two outcome groups. The study conducted multiple logistic regression analysis to examine the association between the outcome variable and all input variables in the same statistical model.
The study used the Python Pandas package (1.5.0) for data preprocessing, TableOne (0.7.12) for descriptive statistics, 13 and the statsmodels package (0.13.2) for the multiple logistic regression analysis. The study measured the variance inflation factor (VIF) and tolerance statistics to ensure no existing collinearity between variables. All statistical tests used 0.05 as the alpha level unless specified.
Results
During the study period, 12,213 patients completed an outpatient visit virtually using telephone and/or video technology. The population was largely unmarried (68.5%), relatively young (mean age = 36.3 years), and majority female (58.3%). The vast majority primarily spoke English as their preferred language (97.0%). The majority of patients (55.7%) had private insurance, whereas 20.8% were on Medicaid and 11.3% were uninsured. The racial and ethnic makeup of the population closely matches that of the general population in North Carolina, with 69.3% of patients identifying as White, 17.6% as Black, 2.6% as Asian or Pacific Islander, and 0.9% as American Indian or Alaskan Native. Approximately 7.4% of patients identified as Hispanic. Among patients completing virtual visits, 894 (7.3%) completed all visits only by telephone, 9,169 used video technology only (75.1%), and 2,150 (17.6%) used both telephone and video technology.
The mean number of visits for those completing telephone visits only was 4.9 ± 0.5, the mean number of visits for those completing video visits only was 6.8 ± 0.2, and the mean number of visits for those completing both telephone and video visits was 16.4 ± 0.7. The telephone and video visits group had a much higher percentage of patients who were seeing both psychotherapists and prescribers (42.4%) compared with the telephone only (18.2%) or video only (15.8%) groups. Weekly completed video visits for all patients and those in the video visit only group showed a gradual increase until around April 2021 and then trended downward (Fig. 1A, B).
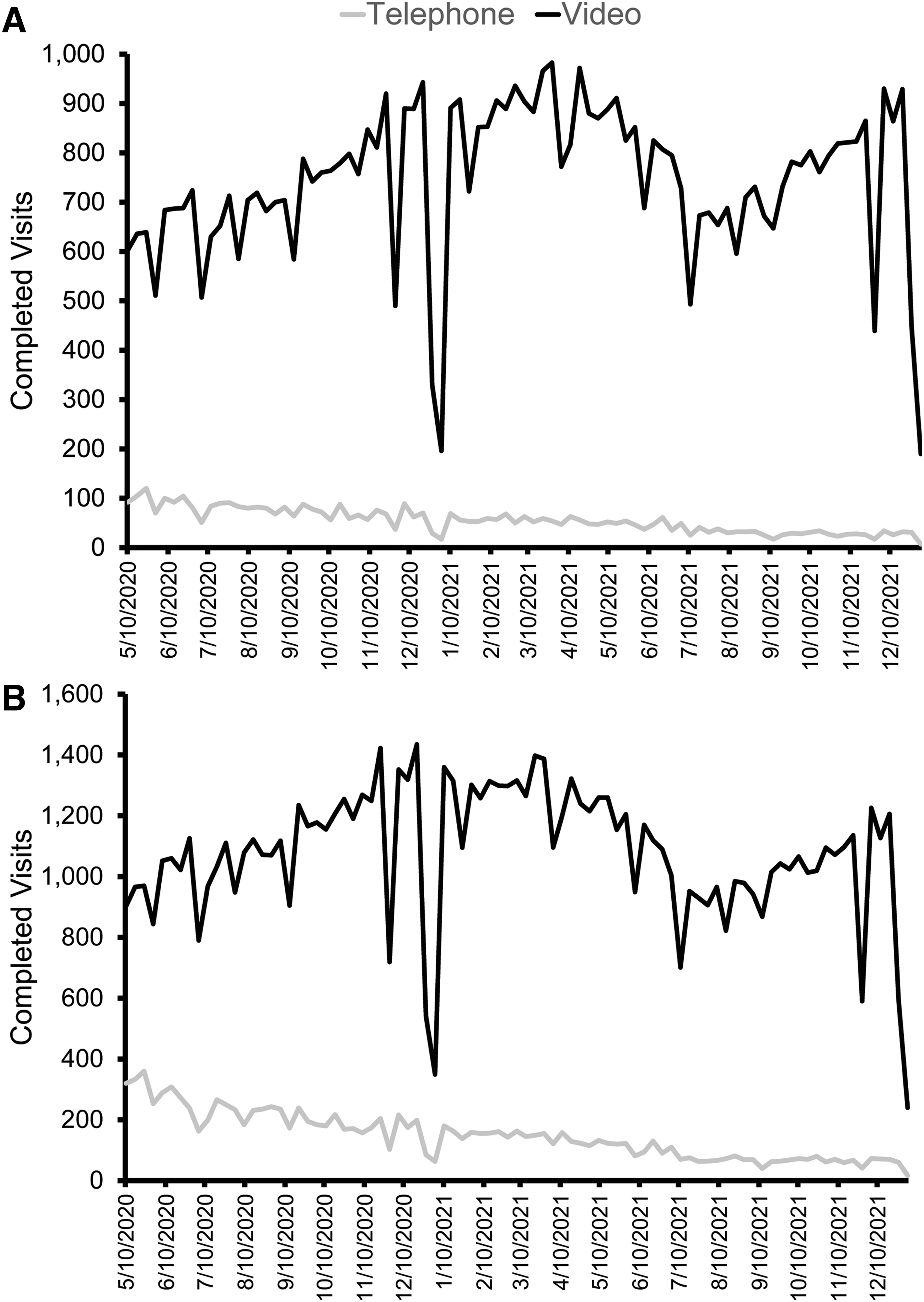
Weekly outpatient psychiatry virtual visit counts.
Weekly telephone visits for all patients and those in the telephone visit only group peaked at the start of the study period and gradually decreased over time (Fig. 1A, B). The percentage of virtual visits completed by telephone differed among provider types, with therapists relying the most on telephone visits (18.2%), followed by advanced practice providers (14.6%), physicians (11.8%), and psychologists (3.1%) (Supplementary Table S1 in the Supplementary Information). In regard to treatment modality, more patients completing telephone visits only saw prescribers only (44.4%), compared with psychotherapists only (36.9%), or both prescribers and psychotherapists (18.2%).
TELEPHONE ONLY VERSUS VIDEO ONLY
Table 1 shows the descriptive statistics of the variables examined comparing patients in the “telephone visit only” and “video visit only” groups. In bivariate analyses (Table 1), demographic factors associated with a higher proportion of telephone visits included male sex, race (other than White), unmarried relationship status, non-Hispanic ethnicity, and rural residence. Patients completing only telephone visits were significantly older than those completing video visits. Insurance status was associated with visit modality, with patients identified as having Medicare or as uninsured having higher rates of only telephone visits.
Characterization of Patients Who Completed Psychiatry Visits Using Only Telephone Compared with Those Using Only Video Technology
AAPI, Asian and Pacific Islander; AIAN, American Indian and Alaskan Native; F, female; M, male; SVI, Social Vulnerability Index.
Patients using only telephone visits had a higher mean SVI, indicating greater social vulnerability. Patients with an inactive patient portal account were more likely to use only telephone services. Among the five chronic conditions examined, depression, diabetes, heart failure, and hypertension were associated with higher proportions of patients completing only telephone visits. Psychiatric diagnosis groups associated with higher use of telephone visits compared with video visits included mental disorders due to a physiological condition, substance use disorders, psychotic disorders, and other psychiatric diagnoses. A significantly higher broadband adoption score was seen in patients who completed only telephone visits.
Multiple logistic regression analyses (Table 2) identified several factors that were associated with a higher odds of completing telephone-only visits. Those included older age, preferred language other than English, an inactive patient portal, comorbid diabetes, higher SVI, and higher broadband adoption. Psychiatric diagnoses associated with higher odds of completing only telephone visits included psychotic disorders, substance use disorders, personality disorders, and intellectual/developmental disabilities. Variables associated with significantly lower odds of completing only telephone visits included seeing a prescriber, comorbid asthma, and private insurance. Psychiatric diagnoses associated with lower odds of completing only telephone visits included anxiety and trauma stressor disorders, eating disorders, pervasive and specific developmental disorders, and disorders of childhood.
Multiple Logistic Regression of Patients Completing Telephone Visits Only Compared with Those Completing Video Visits Only
Bold indicates statistically significant.
CI, confidence interval.
TELEPHONE ONLY VERSUS TELEPHONE+VIDEO
Table 3 shows the descriptive statistics of the variables examined comparing those patients in the “telephone visit only” and those in the “telephone and video visits” group. In bivariate analyses, demographic factors associated with a higher proportion of only telephone visits included male sex, race (other than White), and non-Hispanic ethnicity. Patients using telephone only were significantly older than those using both telephone and video to complete visits. Insurance status was associated with visit modality, with patients identified as having Medicare or as uninsured having higher rates of only telephone visits. Patients using only telephone visits had a higher mean SVI, indicating greater social vulnerability.
Characterization of Patients Who Completed Psychiatry Visits Using Only Telephone Compared with Those Using Both Telephone and Video Technology
Patients with an inactive patient portal account were more likely to use only telephone services. Patients seeing prescribers had slightly lower rates of telephone only visits. Among the five chronic conditions examined, diabetes, heart failure, and hypertension were associated with higher proportions of patients completing only telephone visits. All psychiatric diagnosis groups were associated with higher use of telephone visits compared with video visits, except for personality disorders, intellectual disability disorders, and other mental disorders. A significantly higher broadband adoption score was seen in patients who completed only telephone visits.
Multiple logistic regression analyses (Table 4) identified several factors that were associated with a higher odds of completing telephone only visits. Those included older age, Black race, an inactive patient portal, comorbid diabetes, higher SVI, and higher broadband adoption. Psychiatric diagnoses associated with higher odds of completing only telephone visits included psychotic disorders, substance use disorders, and intellectual/developmental disabilities. Private insurance coverage, married relationship status, seeing a prescriber, and seeing a psychotherapist were associated with significantly lower odds of completing only telephone visits. Psychiatric diagnoses associated with lower odds of completing only telephone visits included anxiety and trauma stressor disorders, eating disorders, pervasive and specific developmental disorders, and disorders of childhood.
Multiple Logistic Regression Comparing Patients Completing Telephone Visits Only with Those Completing Both Telephone and Video Visits
Bold indicates statistically significant.
CI, confidence interval.
Discussion
In this study of a large, outpatient academic psychiatry practice, reliance on telephone technology for virtual care appointments was associated with certain demographic (older age and unmarried status), clinical (substance use disorders, psychotic disorder, personality disorders, intellectual disability disorders, diabetes), and social/geographic (inactive patient portal, SVI, broadband adoption) factors. Many of these factors likely overlap and are related to each other, as we know certain psychiatric conditions are present at higher rates in certain populations, and these individuals can also be associated with higher social vulnerability.
Our findings are both similar to and differ from earlier studies that suggest that race and income play a role in utilization of video technology for virtual visits. 8 –10 While race did not appear to have a significant association with telephone visits in our primary analysis, Black race was associated with a higher odds of completing exclusively telephone visits in our secondary analysis. This could mean that our primary analysis was underpowered to see this association. Our work expands on prior work by identifying that individuals with certain physical health or behavioral health conditions may also be less likely to use video technology for virtual care.
Conversely, certain psychiatric diagnoses were associated with lower reliance on telephone visits only to deliver care. This is likely related to the clear challenges in delivering behavioral health care via telephone for individuals with pervasive and specific developmental disabilities and children. It is not clear why individuals with anxiety disorders, trauma stressor-related disorders, or eating disorders had less reliance on telephone visits only. Similar to psychiatric diagnoses, where an individual lives affects the use of video technology for virtual care access. Interestingly, however, higher rates of broadband internet adoption seemed to be associated with a higher odds of using only telephone visits. It is unclear why that would be the case, although we should point out that the data available to us regarding broadband availability and adoption were at the county level, which may not accurately depict an individual patient's ability to utilize broadband technology at their home.
Also, the most recent data available for broadband availability and adoption were from 2019 and may not reflect any changes that occurred during the study period. Surprisingly, we did not see a difference in reliance on telephone for virtual visits based on urban versus rural residence. We should note, however, that we had a small number of individuals in our study who resided in “rural” counties. This is surprising, given that 70 of the 100 counties in North Carolina are considered rural, but likely reflects the fact that most of the clinics included in our data set are in urban or suburban areas. It may be that a data set that included more rural residents may have seen different results.
For our study, we assumed that individuals who completed telephone visits did so due largely to technical, operational, or financial reasons (lack of internet availability, unable to afford internet access, lack of video-enabled device, limited technology literacy, lack of private space for video appointment, etc.), as opposed to individuals who completed both telephone and video visits, who may have completed telephone visits out of personal preference, provider/health system preference, or convenience. The results of our secondary analyses are nearly similar to our primary analyses, which suggest that those individuals who completed both telephone and video visits are more similar in the variables studied to those individuals who completed video visits only, as opposed to those who completed telephone visits only.
Discussions with department outpatient leadership revealed that early in the COVID-19 pandemic, patients and providers were often given the choice to complete visits via either telephone or video. However, over time, providers were encouraged to only allow video visits for patients who were capable of doing so. This is evident in the trend of telephone visits over time, which generally trail off over the study period. Thus, those who completed both telephone and video visits over the study period likely were allowed/encouraged to complete telephone visits early during the pandemic, despite having the ability to conduct video visits. They then switched over time to video virtual visits once they were encouraged/forced by their providers. Thus, our primary analysis is likely the best way from our available data to examine factors associated with patients who could not complete video virtual visits.
It should be noted, however, that there did appear to be some difference in virtual visit modality completed based on provider type, with psychologists performing relatively few telephone visits (3.1%) compared with other provider types. This is somewhat surprising, given that other types of therapists had the highest percentage of virtual visits completed by telephone (18.2%). Given both groups of psychotherapists are presumably delivering evidence-based psychotherapies, this suggests that the difference could represent either a difference in the patient populations served or a personal preference among different types of therapists. Further investigation is needed to identify the reasons for this difference.
In addition, virtual visits completed by psychologists composed a relatively small percentage of total virtual visits completed during the study period (14.7%), and it is possible that in a practice with a different provider makeup, our primary analyses may produce different results. In addition to type of provider seen, treatment modality also appears to play a role, as in both our primary and secondary analyses, seeing a prescriber was associated with lower odds of reliance on telephone technology for visits.
Recognition of factors associated with higher reliance on telephone technology for virtual visits is important when considering the equity of mental health care. Evidence suggests that certain types of psychotherapies are just as effective when delivered over the telephone as they are in-person, 2,4 and this modality may be sufficient when working with certain populations. However, further study is needed to fully understand whether there is equivalent efficacy for all types of psychotherapies or medication management via telephone when delivered to patients with varying behavioral health conditions. According to our own findings, having a substance use disorder was highly associated with completing only telephone visits.
However, given that much of the care for substance use disorders relies heavily on evidence-based psychotherapies, utilization of telephone technology for virtual care in that population is unlikely to lead to worse patient outcomes. There may be greater concern, however, in a population where treatment more heavily relies on medication management, such as individuals with psychotic disorders. There is insufficient evidence to know whether this patient population can be safely managed via telephone visits alone, and further study is needed.
A similar situation exists when considering whether individuals with unmodifiable factors associated with higher rates of telephone use for virtual care, such as non-White race or older age, are achieving equity in the treatment of their behavioral health conditions. Further study is needed to understand the interplay of these demographic, clinical, and societal factors on the effectiveness of virtual care as delivered through different technologies.
Our study has several limitations. First, the overall proportion of individuals who completed only telephone visits was small in our study population. This likely reflected a strong emphasis by the health system and clinical department leadership on utilization of video visit technology when able to deliver care. Thus, our study may not have enough power to fully recognize factors that are associated with reliance on telephone technology for care delivery. However, given that many of the factors that might be expected to be associated with reliance on telephone technology were significant in our study, it is likely that our findings are legitimate. A second limitation is that documentation of demographic factors within the electronic medical record may not be entirely accurate and are sometimes missing. However, with the exception of patient marital status, there were very few missing data from our study set. An additional limitation is the lack of data about patient income, which is likely associated with a patient's ability to conduct virtual visits for a variety of reasons.
We would suspect that lower income individuals would be more likely to rely on telephone technology for virtual visits, but we are not able to assess that with our data set. The small number of patients in our study that resided in counties identified as “rural” is another limitation of our data set. As a result of this, it is unlikely that we can say with clear certainty that there is not an association between rural residency and reliance on telephone technology for virtual visits. Our results are therefore more applicable to an urban/suburban population, and a data set with a larger number of rural residents may show different results.
Finally, while our data can identify certain factors associated with reliance on telephone technology for virtual appointments, we cannot speculate on the ultimate reasons individuals exclusively used that technology. Patient preference, access to broadband internet access, access to a device (smartphone/laptop/desktop/tablet), technology literacy, and privacy are just a few factors that could drive the patterns seen in our data. Further study is necessary to better understand and interpret our data to address any inequities that may exist in care delivery. While not necessarily a limitation, we should point out that the academic department studied has several different centers and clinics with different types of mental disorders, which represent different patient populations. There may be a need to drill down on the data further to the individual clinic level to understand factors associated with reliance on telephone technology for specific patient populations.
Conclusions
Overall, our study supports earlier work that suggest that certain patient populations utilize video technology at lower rates than others when engaging in virtual care. In particular, older unmarried patients who live in socially vulnerable areas and who have certain mental health disorders are more reliant on telephone to complete virtual behavioral health appointments. This information can be useful to health system leaders in attempting to understand how their virtual care technology is being utilized and where efforts may be necessary to improve access to video technology for care delivery. Further study is needed to fully understand the effect of reliance on telephone for behavioral health care delivery on patient outcomes.
Ethics Approval/Exemption Statement
The study was reviewed and deemed to be exempt by the institutional review board of the University of North Carolina-Chapel Hill.
Footnotes
Acknowledgment
The authors would like to acknowledge Stacey Burgin for her assistance with data collection.
Authors' Contributions
N.A.S. contributed to the conceptualization, formal analysis, investigation, methodology, project administration, and writing for this study. X.Z. contributed to the conceptualization, formal analysis, data curation, investigation, methodology, and writing for this study.
Disclosure Statement
The authors have nothing to disclose related to this work.
Funding Information
The authors have no funding to report that supported this work.
Supplementary Material
Supplementary Information
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.