
Abstract
Background:
Telehealth was adopted to maintain HIV care continuity during the COVID-19 pandemic; however, its use was unequally distributed. This study examined variation in HIV care visit patterns and whether telehealth use was associated with viral suppression.
Methods:
Electronic health record (EHR) data from a large HIV clinic in South Carolina was analyzed using multivariable logistic regression to characterize variation in telehealth use, having a viral load (VL) test, and viral suppression in 2022.
Results:
EHR data from 2,375 people living with HIV (PWH) between March 2021 and March 2023 showed telehealth use among 4.8% of PWH. PWH who are 50+ years and non-Hispanic Black had lower odds of telehealth use (odds ratio [OR] 0.59, 95% confidence interval [CI 0.40–0.86]; OR 0.58, 95% CI [0.37–0.92] respectively). Telehealth use was not associated with viral suppression and VL testing.
Conclusion:
Telehealth disparities in HIV care affected older and non-Hispanic Black PWH, requiring tailored strategies to promote telehealth among them.
Introduction
During the COVID-19 pandemic, people living with HIV (PWH) in South Carolina (SC) faced high levels of HIV care interruptions, as HIV care was at least partially interrupted in over 80% of HIV clinics funded by the Ryan White HIV and AIDS Program and completely interrupted in about one in four clinics for limited periods during the pandemic. 1 To mitigate HIV care interruptions, telehealth was implemented throughout the United States. 2 However, after a couple of months of high rates of telehealth utilization, 2,3 telehealth use reverted back and HIV care was predominantly provided through in-person care. 4,5 Findings regarding variation in telehealth use among subgroups of PWH are conflicting; there is no consensus whether sociodemographic and clinical characteristics of PWH are associated with telehealth use in HIV care. 5 –8
This study aims to provide insights into the utilization of telehealth in SC, a priority state for the Ending the HIV Epidemic campaign targeting high HIV transmission areas. 9 SC is among the top 10 states with the highest rates of HIV diagnoses in 2021, 10 with a disproportionate burden of HIV among historically marginalized racial and ethnic groups and people living in rural areas. 11 –13 Electronic health record (EHR) data from the largest HIV care provider in SC were analyzed to examine trends in telehealth utilization and variation among subgroups of PWH between March 2021 and March 2023, when the initial wave of telehealth use as a response to the COVID-19 pandemic and related public health measures abated. This study aims to examine variation in HIV care visit patterns by race and ethnicity, age, legal sex, and distance to the HIV clinic. It further assesses whether HIV care visit type was associated with viral suppression.
Methods
Design, setting, and data
A retrospective observational study design was used to assess variation in telehealth use and viral suppression among PWH in SC. The study protocol was approved by the Institutional Review Board at Prisma Health Midlands (FWA00000128; IRB Protocol No. 1902952). EHR data from Prisma Health's Immunology Center (PIC) in Columbia, SC, were utilized. PIC is the largest HIV care provider in SC and serves a heterogeneous patient population of ∼2,400 PWH. Study data comprise the universe of visits of eligible patients between March 2021 and March 2023 (25 months). EHR inclusion criteria were (a) Patient is 18 years or older; (b) Patient is living with diagnosed HIV infection; and (c) Patient received HIV care at PIC during the study period. EHR data were extracted using Epic's Caboodle database (Epic, Verona, WI). Data stored in the Caboodle database were retrieved by a data analyst using structured query language coding and shared in deidentified format.
Variables of interest
HIV care visit patterns were defined as PWH who had (1) only in-person visits versus PWH who had (2) at least one telehealth visit (including video and telephone visits). The secondary outcome variable, viral load (VL) test history in 2022 was categorized into two groups: no VL test versus at least one VL test. The tertiary outcome variable, viral suppression in 2022, was defined as PWH whose VL test results were <200 (i.e., virally suppressed), vs. PWH who had at least one VL test result ≥200.
To assess variation in HIV care visit patterns, VL test history, and viral suppression, the following covariates were examined. Current age of PWH (at the time of data extraction in June 2023) was categorized into two groups: 18–49 years old versus 50 years or older. Distance to the HIV clinic was described by differentiating between PWH who were living in the same county as the clinic location versus PWH who were living in any other county at the time of data extraction. Race and ethnicity were categorized into three groups: non-Hispanic White versus non-Hispanic Black versus other PWH and people whose race and ethnicity was unspecified. Legal sex was categorized into two groups: female versus male. For VL test history and viral suppression analyses, HIV care visit patterns were included as a covariate.
Data analysis
Descriptive statistics were used to describe the study sample regarding the abovementioned covariates. The distribution of visit types was presented graphically by calendar month and covariates. For analyses to characterize variation in telehealth use, having a VL test in 2022, and viral suppression in 2022, multivariable logistic regression analyses were conducted. Logistic regression results were reported as odds ratios (OR). p < 0.05 were considered statistically significant. Analyses were performed in StataSE version 18 (StataCorp, College Station, TX) and Microsoft Excel 365 (Microsoft Corporation, Redmond, WA).
Results
Sample characteristics
Table 1 summarizes demographic and clinical characteristics of 2,375 PWH cared for by PIC between March 2021 and March 2023. Around 95.2% of PWH used in-person HIV care exclusively and more than four in five PWH had consistently suppressed VL tests in 2022. Compared with in-person visit-only users, telehealth users were more likely to be between 18 and 49 years of age. Between March 2021 and March 2023, 440 PWH per month were seen on average; out of these 9 PWH were seen through telehealth.
Characteristics of Patients Living with HIV
Bold values indicate statistically significant p-values at p < 0.05.
p-values are calculated by Pearson's chi-square test.
VL, viral load.
Distribution of visit types over time
Figure 1 displays the distribution of PWH over time by visit type and selected patient characteristics. Figure 1A shows that both the in-person and telehealth visit rates were higher for those who are 18 to 49 years of age. Visit rates by residence were similar for in-person and telehealth visits (Fig. 1B). In-person visit rates were highest among PWH of other races and ethnicities or whose race and ethnicity is unspecified with notable spikes every three months as compared with non-Hispanic Black and White PWH (Fig. 1C). Telehealth visit rates were highest among non-Hispanic White PWH between March 2021 and May 2022. Starting in June 2022, telehealth visit rates were highest among PWH of other races and ethnicities or whose race and ethnicity is unspecified. Figure 1D shows that in-person and telehealth visit rates among females were slightly higher than among males.
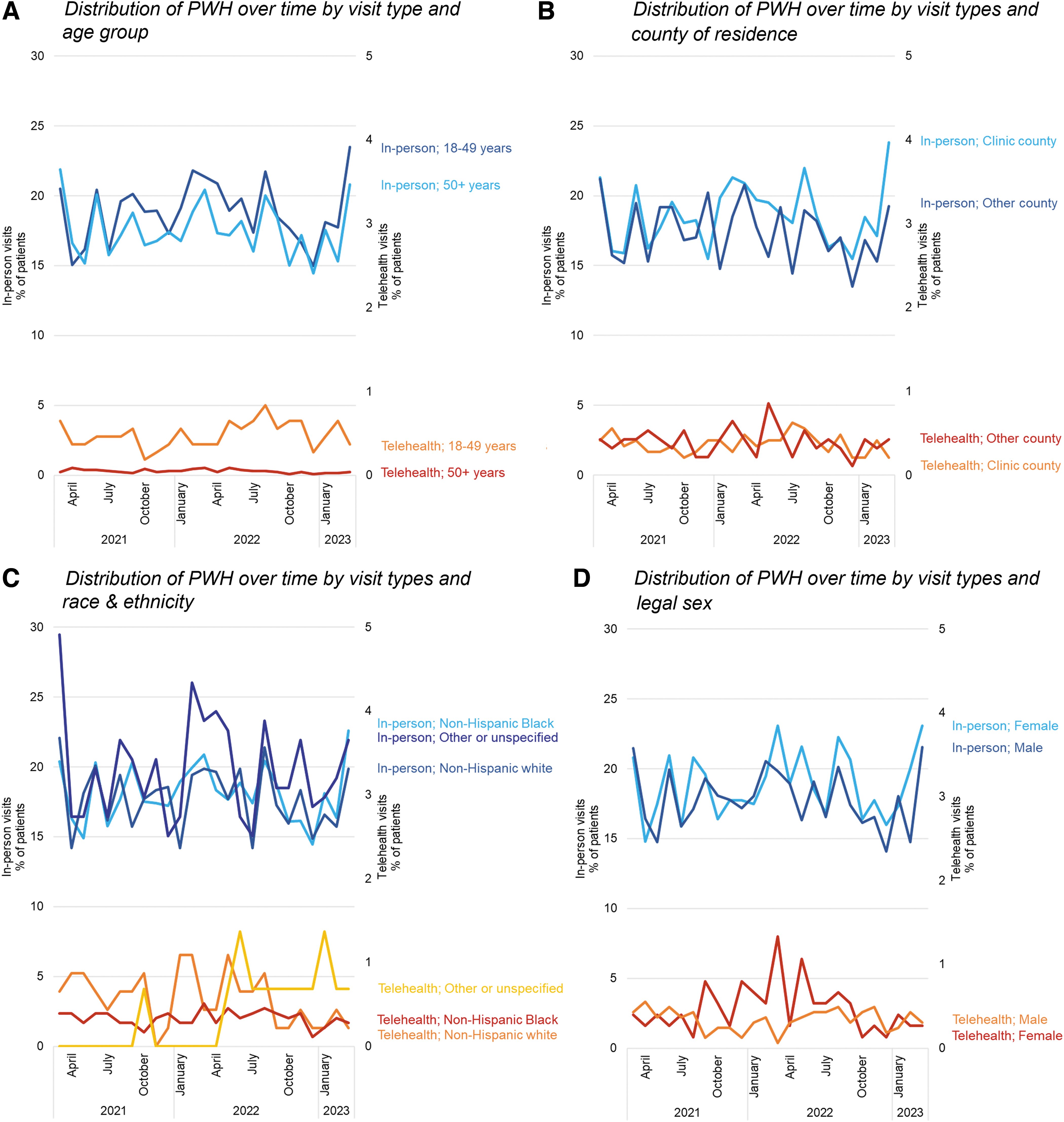
Distribution of PWH over time by visit type and selected characteristics of PWH. PWH, people living with HIV.
Variation in HIV care visit patterns, VL test history, and viral suppression
Table 2 shows the results of three multivariable analyses examining the association of sociodemographic characteristics with HIV care visit patterns, and the association of sociodemographic characteristics and HIV care visit patterns with having a VL test in 2022 and viral suppression in 2022. After adjusting for sex and the county of residence, the odds of telehealth use were lower for PWH who are 50 years or older and non-Hispanic Black PWH. Visit type was neither associated with having a VL test in 2022 nor with viral suppression in 2022. However, after adjusting for sex, race and ethnicity, and the county of residence, the odds of having a VL test in 2022 were higher among PWH who are 50 years or older. Among people who had a VL test in 2022, the odds of being consistently virally suppressed in 2022 were higher among PWH who are 50 years or older and lower among non-Hispanic Black people after adjusting for sex and the county of residence.
Multivariable Regression Associations of Sociodemographic Characteristics with HIV Care Visit Type Patterns, Viral Load Test History in 2022, and Viral Suppression
Bold values indicate statistically significant p-values at p < 0.05.
Discussion
Our study is the first to assess telehealth disparities in HIV care in SC providing important findings on how telehealth has been sustained after the steep increase in response to the COVID-19 pandemic and public health measures controlling COVID-19. Telehealth HIV care was used by <1 in 20 PWH (4.8%) cared for by PIC between March 2021 and March 2023.
We found disparities in telehealth use among older and non-Hispanic Black PWH, which is mirroring other literature, 5,6 and contributes important evidence to conflicting literature. 7,8 While EHR data may not be able to provide reasons for these disparities, PWH face various barriers to telehealth HIV care, including access to technology and sufficient internet, digital literacy, feeling uncomfortable with telehealth, and perceiving telehealth as impersonal. Literature further suggests that some of these telehealth barriers are intensified among older PWH and PWH who belong to historically marginalized racial and ethnic groups. 2,14 Strategies to increase telehealth use among older and non-Hispanic Black PWH to support HIV care should be explored.
Visit type was neither associated with having a VL test nor with viral suppression. However, younger people were less likely to have a VL test, and among PWH who had VL test results documented in their EHR, we found that younger and non-Hispanic Black PWH were less likely to be consistently virally suppressed. COVID-19's toll on mental health and other sociodemographic factors impacting antiretroviral adherence may have contributed to disparities in VL testing and viral suppression. 15 In-depth analyses to understand the mechanisms and reasons for these disparities are needed to develop tailored strategies to improve VL testing and viral outcomes among PWH experiencing disparities, including younger and non-Hispanic Black PWH. Nonclinic-based strategies for VL testing may be explored (e.g., local laboratory test referrals, home-based VL testing and monitoring 16 ) to increase testing rates.
Limitations
Several limitations of this study are worth mentioning. First, this study used EHR data from one HIV care clinic in SC, which limits generalizability beyond this population. Second, our analyses utilized a small number of covariates based on their expected association with telehealth use. Nevertheless, findings from this study warrant future research expanding the analysis to include other known sociodemographic and clinical characteristics associated with HIV care utilization, VL testing, and viral suppression. Third, due to very low numbers of PWH receiving telehealth only (N = 5), visit type patterns were collapsed onto a binary variable assessing any telehealth use. To fully understand the impact of telehealth on HIV care outcomes, separating between the telehealth only and a combination of telehealth and in-person HIV care is recommended for future research. Fourth, the study period (March 2021 to March 2023) was impacted by limited data availability. PIC transitioned to Epic EHR management software in February 2021, and data from the previous EHR management system (i.e., pre-March 2021) are not easily accessible.
Conclusions
Telehealth in HIV care was used by <5% of PWH, and disproportionately less by older and non-Hispanic Black PWH, between March 2021 and March 2023. Telehealth use was not associated with VL testing or viral suppression. Strategies to increase telehealth use among older and non-Hispanic Black PWH to support HIV care should be explored.
Footnotes
Acknowledgment
The authors greatly appreciate the support from the Data Support Core at Prisma Health, especially Dr. Joseph A. Ewing and Criosanna Allred, for the electronic health record extraction.
Authors' Contributions
V.Y., J.O., S.W., N.N., B.O., and H.A. contributed to the study conception and design. The electronic health record data extraction strategy was developed by V.Y. and J.O. Data collection and analysis were performed by V.Y. and J.O. The first draft of the article was written by V.Y. and all authors commented on previous versions of the article. All authors read and approved the final article.
Data,Materials,and/or Code Availability
Deidentified, aggregated data that support the findings of this study are available from the corresponding author, V.Y., upon reasonable request and documentation of approval or exemption by the relevant IRBs.
Ethics Approval
The study protocol was approved by the Institutional Review Board at Prisma Health Midlands (FWA00000128; IRB Protocol No. 1902952).
Disclosure Statement
No competing financial interests exist.
Funding Information
Research reported in this publication was supported by the Agency for Health care Research and Quality (AHRQ) Grants for Health Services Research Dissertation Program (Grant No. 1R36HS029267), the 2022 Health Sciences Center at Prisma Health Research Seed Grant Program, and the SPARC Graduate Research Program from the Office of the Vice President for Research at University of South Carolina. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Health care Research and Quality, Prisma Health, or the University of South Carolina.