
Abstract
Background
: The telemanagement model in chronic diseases needs older patients to have a certain level of e-Health literacy. According to Electronic Health Literacy model, factors associated with the e-Health literacy among older patients could be comprehensively investigated from individual, situational, and environmental aspects.
Objectives:
To investigate the e-Health literacy levels among older patients with chronic obstructive pulmonary disease (COPD) and explore associated factors.
Methods
: A cross-sectional study was conducted among older patients with COPD. The e-Health Literacy Scale was used to measure individuals' e-Health literacy. The multiple linear regression was applied to identify factors associated with e-Health literacy.
Results
: A total of 230 responses were included in the final analysis. The average score of e-Health literacy for older COPD patients was 24.66 (6.86). After adjusting the model, the results of multiple linear regression demonstrated that aging attitudes (B = 0.067, p < 0.001), technophobia (B = −0.285, p < 0.001), and self-efficacy (B = 0.431, p < 0.001) accounted for 68.3% (p < 0.001) of the total variation in e-Health literacy.
Conclusion
: This study identifies significant correlations of technophobia, aging attitudes, and self-efficacy, respectively, with e-Health literacy, and self-efficacy and technophobia may be constant predictive factors of e-Health literacy. In the future, intervention research on e-Health literacy should be conducted from a social psychology perspective, with particular emphasis on addressing negative aging attitudes and technophobia. That will promote the tele-management model of chronic diseases.
Trial Registration:
Chinese Clinical Trial Registry (ChiCTR): ChiCTR1900028563;
Introduction
With the aging of the population and the increasing prevalence of chronic diseases, human health is facing a huge burden. 1 It is well known that effective chronic disease management can improve patients' health outcomes and reduce the occupation of medical resources. However, the promotion of chronic disease management is limited by several factors, such as uneven distribution of health resources and input costs. 2 Today, information technology is developing rapidly, the management of chronic diseases through telemedicine offers the benefits of resource conservation, temporal and spatial flexibility, and economic convenience. 3 There is also evidence that tele-management model in chronic diseases guarantees patient participation and informed consent. 4
Tele-management model in chronic diseases needs patients having a certain level of e-Health literacy. 5,6 The e-Health literacy refers to an individual's ability to search, locate, comprehend, and evaluate various health information resources from electronic sources, and apply the acquired knowledge to solve health problems. 7 Unfortunately, research indicated that the e-Health literacy of older adults was at a low level. 6,8 Chronic obstructive pulmonary disease (COPD) is one of the most common chronic diseases of older adults. It is necessary to carry out research on the factors associated with the e-Health literacy in older patients with chronic diseases, and it is helpful to explore the influencing factors of low level of e-Health literacy in this population.
The current evidence suggests the correlation of symptom burden, knowledge of COPD, self-efficacy, social support, income, duration of internet usage, educational level, age, and gender, respectively, with e-Health literacy in patients with COPD. 9 –14 Kim et al. found a correlation between technophobia and e-Health literacy among individuals 50 years of age and above. 15 In addition, research suggested that there was a significant correlation between e-Health literacy and health behaviors, 16 and aging attitudes could influence health behaviors. 17 The research of Li et al. indicated a correlation between digital skills and e-Health literacy of older adults. 18 At present, the correlation of technophobia, aging attitudes, and web search skill, respectively, with e-Health literacy has not been confirmed in the older COPD population.
The Electronic Health Literacy (EHL) model, 19 also referred to as the Media Health Literacy (MHL) model, was introduced by Levin-Zamir in 2018. It comprises Personal (Sociodemographics and Individual skills), Situational (Current acute and chronic health concerns), and Environmental (Media environment and Social environment). Technologic experience and the utilization of technological media are involved in this model. Applying this model can not only comprehensively explore the factors associated with e-Health literacy in the context of tele-management model in chronic diseases, but also align with the current trend of telemedicine development. The aim of this study is to investigate the correlation of diverse factors with e-Health literacy, utilizing this model as a framework.
The factors include sociodemographics (gender, age, religion, income, education level, types of medical insurance payment), individual skills (duration of internet usage, web search skill), acute/chronic health issues (body mass index [BMI], smoking status, years with COPD, hospitalizations for COPD in the last 1 year, Global Initiative for Chronic Obstructive Lung Disease [GOLD] stage, dyspnea, symptom burden, knowledge of COPD), current emotional state (self-efficacy, aging attitudes, technophobia), media environment (types of mobile terminals), and social environment (marital status, place of residence, social support).
Methodology
This study adopted a cross-sectional design. The study is reported using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for a cross-sectional study. 20 The study was reviewed and approved by the Medical Ethics Committee of Jiangnan University (JNU20220310IRB17). Before conducting the survey, all study participants were informed.
SAMPLING
Older patients with COPD from the respiratory medicine wards and outpatient clinics of three general hospitals in a city were recruited as the study population from November 2022 to April 2023. The sample of study is 202 cases according to G.Power 3.1. 21
Inclusion criteria met the diagnostic criteria in the GOLD (2023), 22 ≥65 years of age, and could complete the questionnaire independently or with the help of the researchers. Exclusion criteria were patients with severe mental, cognitive impairment, or hearing or speech dysfunction.
SURVEY INSTRUMENTS
A home-made demographic and disease-related information questionnaire was used to collect data. The data included gender, age, BMI, religion, marital status, place of residence, monthly income, education level, types of mobile terminals, duration of internet usage, web search skill, types of medical insurance payment, smoking status, years with COPD, hospitalizations for COPD in the last 1 year, and GOLD stage.
The e-Health Literacy Scale (e-HEALs) was used, which was compiled by Norman and Chineseized by Guo et al. (Cronbach's alpha coefficient was 0.913). 23,24 The higher scores indicated the higher e-Health literacy.
The modified Medical Research Council Dyspnea Scale was used, which was recommended by the GOLD guideline. 22 The higher grades indicated the more severe breathing difficulty.
The COPD assessment test was used (Cronbach's alpha coefficient was 0.84), which was recommended by the GOLD guideline. 22 The higher scores indicated a greater impact of the disease on the patient's health status and a greater symptom burden.
The Chronic Obstructive Pulmonary Disease Knowledge Questionnaire (COPD-Q) was used, which was developed by Maples P (Cronbach's alpha coefficient was 0.72). 25 This questionnaire was widely used in China. 26 The higher scores indicated the higher levels of knowledge.
The General Self-efficacy Scale was used (Cronbach's alpha coefficient was 0.87), which was compiled by Schwarzer and Chineseized by Wang et al. 27,28 The higher scores represented the higher levels of self-efficacy.
The Attitudes to Aging Questionnaire was used, which was compiled by Laidlaw and Chineseized by Huang et al. (Cronbach's alpha coefficient was 0.83). 29,30 The higher scores represented the more positive the aging attitudes.
The Technophobia Scale was used, which was compiled by Khasawneh and Chineseized by Sun et al. (Cronbach's alpha coefficient was 0.911). 31,32 The higher scores represented the higher the levels of technophobia.
The Social Support Rating Scale was used, which was compiled by Xiao (Cronbach's alpha coefficient was 0.92). 33 The higher scores represented the higher social support.
The Web search skills questionnaire was used, which was a home-made questionnaire. Ask the patient complete the task using common search engine within 1 min. The task includes four steps as following. Firstly, use input methods (typing, speech, handwriting, etc.). Secondly, enter question into the search box and click the search button. Thirdly, click on the web page that contains the query. Fourthly, find out the details. The score is given based on the actual completion. One point indicated totally unperforming task within 1 min. Two points indicated performing task with the assistance of others within 1 min. Three points indicated performing task independently within 1 min. The questionnaire had a test/retest reliability of 0.928 and the content validity of 1.
DATA ANALYSES
SPSS Statistics version 26.0 was used. Demographic and disease-related characteristics of the study participants were analyzed by descriptive statistics, and multiple linear regression analysis to explore the factors associated with e-Health literacy in older COPD patients. All statistical tests were two-sided (α = 0.05). Two linear regression models were used to explore the correlation between independent variables and e-Health literacy. One model was unadjusted while the other model was adjusted for demographic and disease-related information, as well as web search skill.
In addition, to further validate the heterogeneity of the results, subgroup analyses were performed to determine whether the association differed by age and web search skill. The conditions of normality, variance chi-square, multicollinearity, and independence of multiple linear regression were clearly met by residual histograms, P-P plots, residual scatter plots, variance inflation factors, and Durbin Watson.
Results
STUDY PARTICIPANTs' DEMOGRAPHIC AND DISEASE-RELATED CHARACTERISTICS
The flow diagram is shown in Figure 1. Descriptive data on the demographic and disease-related information of the study population are shown in Table 1.
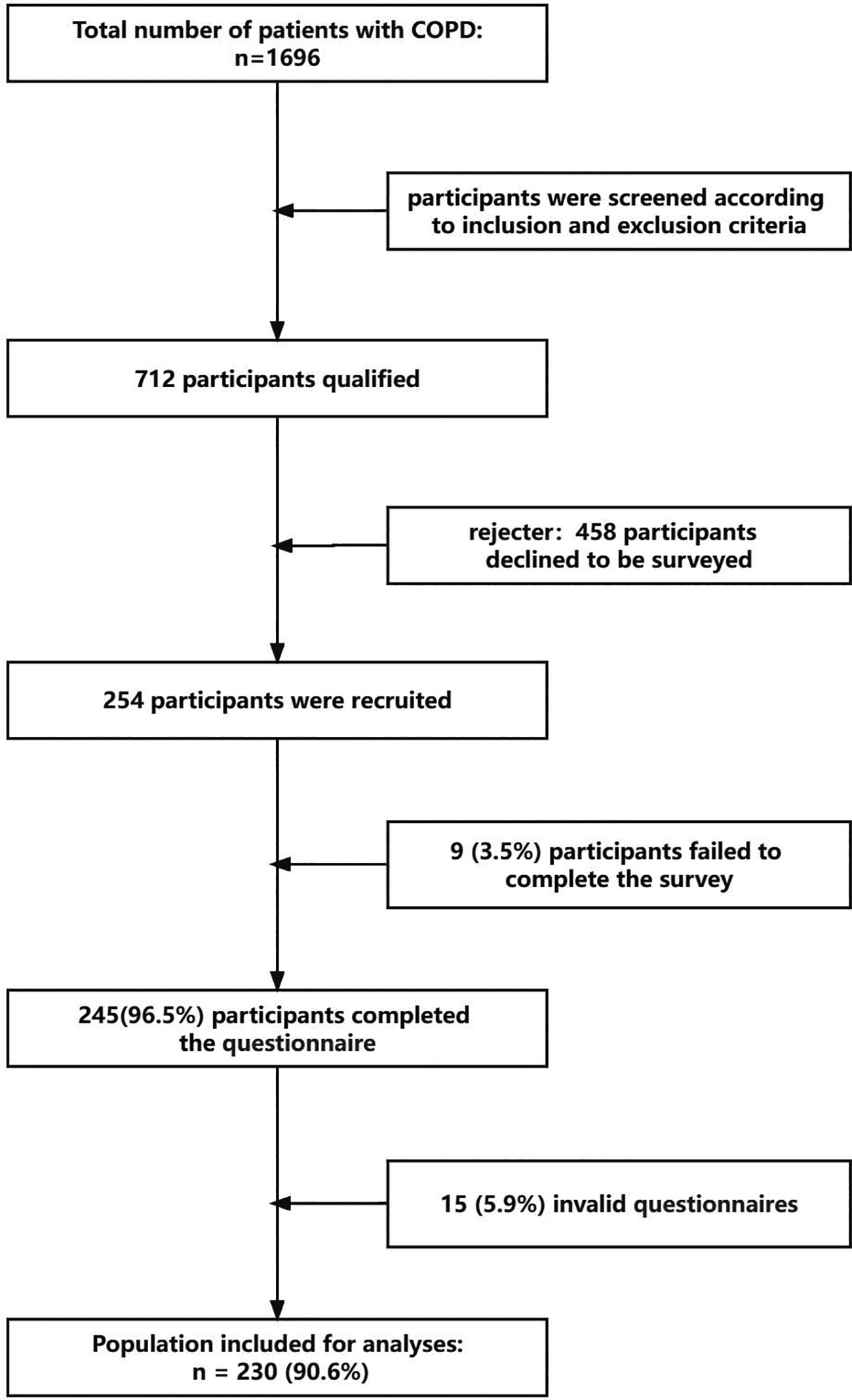
The flow diagram.
Demographic and Disease-Related Characteristics of the Study Participants and Differences of e-Health Literacy by Characteristics (n = 230)
Independent samples t tests.
One-way analysis of variance.
COPD, chronic obstructive pulmonary disease; e-HEALs, e-Health Literacy scale; GOLD, Global Initiative for Chronic Obstructive Lung Disease.
DESCRIPTIVE STATISTICS AND CORRELATION ANALYSIS RESULT OF STUDY PARTICIPANTS
The scores of e-HEALs corresponding to other variables are detailed in Table 2, and the results of the correlation analysis are shown in Table 3.
Descriptive Statistics of Variables (n = 230)
AAQ, Attitudes to Aging Questionnaire; CAT, COPD Assessment Test; COPD-Q, Chronic Obstructive Pulmonary Disease Knowledge Questionnaire; GSES, General Self-efficacy Scale; mMRC, modified Medical Research Council Dyspnea Scale; SSRS, Social Support Rating Scale; TS, Technophobia Scale; WSSQ, Web Search Skills Questionnaire.
Results of Correlation Analysis Between the e-Health Literacy and Other Variables (n = 230)
Spearman correlation analysis.
Pearson correlation analysis.
p < 0.001.
UNIVARIATE ANALYSES OF THE FACTORS ASSOCIATED WITH e-HEALTH LITERACY
The differences in levels of e-Health literacy by demographic and disease-related information are shown in Table 1. The results of the study showed differences in the e-Health literacy of older COPD patients by age, place of residence, education level, duration of internet usage, web search skill, and types of medical insurance payment (p < 0.05).
RESULTS OF MULTIPLE LINEAR REGRESSION ANALYSIS OF e-HEALTH LITERACY OF THE STUDY PARTICIPANTS
The results of multiple linear regression analysis are shown in Table 4. In the unadjusted model, the results show that self-efficacy, aging attitudes, and technophobia are factors associated with e-Health literacy of older people with COPD, together explaining 60.9% of the total variance in e-Health literacy levels in older COPD patients (R 2 = 0.614, adjusted R 2 = 0.609, F = 119.660, p < 0.001). After controlling for demographic and disease-related information, and web search skill in the model, the results show that self-efficacy, aging attitudes, and technophobia are factors associated with e-Health literacy of older people with COPD, together explaining 68.3% of the total variance in e-Health literacy levels in older COPD patients (R 2 = 0.693, adjusted R 2 = 0.683, F = 71.511, p < 0.001).
Results of Multiple Linear Regression Analysis of e-Health Literacy of the Study Participants (n = 230)
B, unstandardized regression coefficient; Beta, standardized regression coefficient; SE, standard error; VIF, variance inflation factor.
Additionally, the subgroup analyses were according to age and web search skill. The associations of self-efficacy and technophobia with e-Health literacy are statistically significant in both the unadjusted and adjusted models. The age subgroup analysis shows a statistically significant difference between the two groups (p < 0.001). Aging attitudes score of age group from 65 to 74 is 78.79 (19.77), the score is 68.07 (19.82) of age group ≥75. In the subgroup of web search skill, there is no difference in COPD-Q scores among the three groups (p > 0.05).
Discussion
This study investigates the determinants of e-Health literacy among older patients with COPD according to the EHL model. 19 In addition, this study identifies significant correlations of technophobia, aging attitudes, and web search skill, respectively, with e-Health literacy in the older COPD population for the first time. The study also finds that there are many factors associated with e-Health literacy, including dyspnea, symptom burden, knowledge of COPD, self-efficacy, social support, age, place of residence, level of education, duration of internet usage, and types of medical insurance payment.
Currently, there is a lack of standardized norm for the development of e-Health literacy. Research suggested that the average, median, or 26 points of e-Health literacy could be regarded as criteria for norm. 34 –36 However, currently there are no norms for the older population, especially those with chronic diseases. A multicenter survey is imperative to establish a norm for e-Health literacy level among the older population and subgroups with chronic diseases, thereby facilitating future research in this area. This study also highlights the importance of considering the e-Health literacy level of older patients with chronic diseases, when providing them online health information, to ensure accessibility to e-Health literacy and promotion of tele-management model in chronic diseases.
This study reveals a negative correlation between technophobia and e-Health literacy, which is consistent with the findings of Kim et al.'s research on adults 50 years of age or above. 15 Technophobia refers to the irrational fear and apprehension that individuals experience toward various digital technologies, including mobile communication devices, artificial intelligence, and robots. 31 That results in emotional reactions such as fear and nervousness, so that individuals avoid using technology altogether. 37 –39 Nimrod discovered that older adults with higher levels of technophobia exhibited reduced internet usage during the COVID-19 pandemic, thereby impeding efforts to enhance e-Health literacy. 40 Undoubtedly, mitigating technophobia among the older can enhance their adoption of mobile technology. According to the Technology Acceptance Model, 41 patients are more likely to adopt positive attitudes to technology and related services when they perceive easy to use (PEOU) and perceive useful (PU). The presence of technophobia directly influences individuals' perception of usability.
Positive emotional experience is conducive to technology acceptance that originates from PEOU and PU. 42,43 This requires cooperation from all sectors of society to address the problem of technophobia, such as utilizing co-creation methods to develop operational platforms. In addition, the role of social environment can also be leveraged. As study suggested providing an environment that can relieve technophobia. 15 This study reveals a post-pandemic e-Health literacy level of 24.58 (9.58) among older individuals in China, which is different from the prepandemic level of 17.24 (9.34). 8 The reason for this phenomenon may be attributed to the extensive use of mobile devices for online health reporting and accessing epidemic-related information among the Chinese population during the COVID-19 pandemic.
The study reveals a positive association between e-Health literacy and aging attitudes. The aging attitudes refer to an individual's perception and evaluation of their own process and state of aging. 29 It includes positive and negative orientations. This study reveals that individuals with positive attitudes not only exhibit optimal physical and mental wellbeing, but also actively engage in societal activities. They can create substantial value for the society. Simultaneously, they are eligible to receive social security benefits when they need help. These findings align with the World Health Organization's notion of active aging. 44 The active aging concept underscores “health,” “participation,” and “security” as fundamental principles. 44,45 The primary objective of all e-Health literacy models is to enhance the promotion of “health.” 19,46 –50
The concept of “participation” is a common element among the five models of e-Health literacy. 19,47 –50 These models include Integrative Model of e-Health Use, comprehensive model of e-Health literacy, Expanded User-Task-Context Matrix for e-Health Literacy, Transactional Model of e-Health Literacy, and EHL model. The concept of “security” is incorporated in three models. 19,49,50 These models include Expanded User-Task-Context Matrix for e-Health Literacy, Transactional Model of e-Health Literacy, and EHL model. Clearly, there are intersections between the concepts of active aging and the e-Health literacy model. Additionally, this study reveals that patients with negative aging attitudes exhibit lower levels of e-Health literacy.
There are two types of negative aging attitudes. 6,51 –53 One is that the general public portrays the older population as less independent, less productive, more vulnerable, and forgetful. The other is that older individuals themselves are inclined to embrace these stereotypes of aging. Consequently, older individuals have developed a perception that they lack the ability to effectively utilize online health information. Furthermore, within the age subgroup analyzed in this study, the correlation has been found between more positive aging attitudes and higher levels of e-Health literacy.
Interestingly, this study indicates that the aging attitudes score of 75.43 or above seems to affect a change in e-Health literacy. This suggests that when the aging attitudes are used as the intervention target in the future, it may be necessary to improve the aging attitudes score to a level above 75.43. However, this result needs to be verified through large-scale intervention experiments. In the future, positive psychology can change the negative aging stereotype of society and individuals, so as to improve the e-Health literacy level of the older. Simultaneously, it is imperative to improve the offline community health service system to mitigate feelings of technological deprivation among older individuals who have negative aging attitudes and low e-Health literacy.
Regardless of adjustment, the sub-analysis of web search skill in this study indicates that there is no difference between the totally unperforming group and the other assisted group in explanatory variables or R 2 for e-Health literacy. These findings highlight the critical importance of prioritizing interventions targeting web search skill within e-Health literacy programs. This study reveals that self-efficacy and technophobia consistently exist in the model. So self-efficacy and technophobia may be constant predictive factors of e-Health literacy. Future interventions should prioritize addressing these influential variables. Furthermore, this study reveals the correlation of COPD knowledge, symptom burden, social support, dyspnea, duration of internet usage, educational level, and place of residence with e-Health literacy. These findings align with previous research outcomes. 9 –14,54,55
LIMITATION AND FUTURE RESEARCH
This study has several limitations. First, the study design is cross-sectional and cannot confirm the causal relationship between the variables. To address it, future relevant longitudinal studies should be conducted to explore the causal relationships between variables. Second, the survey is conducted in a single region, and the sample size is 230 cases that may have led to slight bias in the subgroup results. In the future, large-sample and multicenter studies are needed to further verify these conclusions. Third, although the e-HEALs is the most commonly used tool in the research, 56 there are also other tools to assess e-Health literacy. More tools will be suggested to assess e-Health literacy in future research.
Conclusion
This cross-sectional study has enhanced the comprehension of factors associated with e-Health literacy among older patients with COPD by utilizing the EHL model. The study highlights the necessity for a standardized norm of e-Health literacy development among older patients with chronic diseases, and this is the first study, which found a significant correlation between aging attitude and e-Health literacy, while self-efficacy and technophobia may serve as constant predictive factors among the older patients with chronic diseases. In future research, it is imperative to underscore the pivotal role of social psychology in enhancing e-Health literacy among older COPD patients. The e-Health literacy could be promoted by intervention of aging attitudes, technophobia, and self-efficacy. That will enhance the effectiveness of tele-management model in older adults with chronic diseases and promote active aging. Furthermore, greater attention should be given to older individuals who exhibit technophobia, negative aging attitudes, low self-efficacy, poor web search skills, limited internet usage duration, and low educational levels. They are high-risk populations with low levels of e-Health literacy.
Footnotes
Acknowledgment
The authors thank all patients who participated in this study.
Authors' Contributions
Y.J. designed the research protocol; organized the experimentation and recruitment; performed experimentation, data collection, and interjudge reliability; analyzed data; and wrote the article. J.G. organized the experimentation and recruitment; performed experimentation, data collection, and interjudge reliability; analyzed the data; and wrote the article. P.S. designed the research protocol; organized the experimentation and recruitment; performed experimentation, data collection; and wrote the article. J.N. performed experimentation, data collection, and interjudge reliability. X.Z. performed experimentation, data collection, and interjudge reliability. M.S. supervised the experiment and reviewed the article. X.S. supervised the experiment.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grants from the National Natural Science Foundation of China (No. 72274080).
Supplementary Material
Supplementary Notes S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.