
Abstract
Introduction:
The COVID-19 pandemic brought unprecedented change to the health care industry, including a large and rapid shift to providing care through telehealth technologies. Although the expansion of telehealth services was successful in continuing to provide patients with care while preventing the spread of disease, it is less clear how patient sociodemographic characteristics influenced telehealth use during this time. This study aims to systematically review the published literature on demographic differences in telehealth access, utilization, and health outcomes among a variety of adult patient types in the United States.
Methods:
Litcovid, PubMed, Web of Science, and MEDLINE databases were searched, resulting in a final sample of n = 32 studies.
Results:
Results found that studies could be categorized as addressing at least one of eight different areas of inquiry: sociodemographic differences in telehealth use (1) during and (2) before the pandemic, telehealth use versus nonuse (3) during and (4) before the pandemic, (5) telehealth modality, (6) satisfaction with telehealth, (7) outcomes associated with telehealth use, and (8) perceived or actual access to telehealth services.
Discussion:
Findings are robust across included studies with respect to racial, age, and socioeconomic differences in telehealth utilization and health outcomes, reflecting sociodemographic differences in health care access, utilization, and outcomes more broadly that persist despite this expansion of telehealth services owing to COVID-19. Additional findings across studies are summarized and areas for future research are discussed.
Introduction
Following the onset of the COVID-19 pandemic in the United States in March 2020, many health care systems and providers rapidly transitioned to telehealth, or the delivery and/or receipt of health care services through telephone, video-conferencing, or other remote patient-monitoring technologies. 1,2 Although this transition may have been successful in continuing to provide patients with access to care and prevent the spread of the coronavirus disease, 3 –6 it is less clear how this transition to a new modality of health care delivery impacted access, utilization, and health outcomes among a wide population of health care users. It is likely that patients' sociodemographic characteristics, 7 health behaviors, 8 preexisting health conditions, or other predisposing, enabling, or needs factors 9 –12 affect access to, utilization of, and subsequent outcomes associated with telehealth services.
However, much of the research conducted on disparities in expanded telehealth utilization is from the early months of the pandemic or relied on small, specific samples and therefore is not generalizable to the larger U.S. population. Furthermore, although several structured reviews have been conducted on telehealth during the pandemic, many were performed quickly or within the early days of the global health emergency, 6 focused on the application 4 or implementation 13 of telehealth rather than rates of utilization, or limited the review to telehealth use within a distinct specialty care area. 14
To synthesize this growing area of research and to better understand how sociodemographic factors influence telehealth utilization, access, and potential health outcomes during the COVID-19 pandemic, an updated systematic review focusing on studies measuring demographic disparities or inequalities in telehealth use is needed. The disproportionate impacts of COVID-19 on socially and/or economically marginalized populations, 15 as with past global pandemics, 16 highlight the need to better understand how historically underserved groups are accessing—or face barriers in accessing—health care services during public health crises. Furthermore, as society continues into the digital age, it is important to understand how telehealth technologies are being used, and who is using them, to prevent a widening gap in access or outcome disparities.
This review will address the following research question: How did the expansion of telehealth services during the COVID-19 pandemic affect health care utilization and/or access? Sub-questions include the following: Were some sociodemographic groups more likely to access telehealth services than others? Did the expansion of telehealth services affect health care access and utilization disparities? Did the expansion of telehealth services influence inequalities in health outcomes? To review studies that address these questions, Litcovid, PubMed, Web of Science, and MEDLINE on EBSCOhost databases will be searched. This systematic review will follow the steps in the PRISMA-P checklist 17 and, relying on the help of a second reviewer, will present inter-rater reliability at both the initial screening and data extraction phases.
Methods
This systematic review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses protocol (PRISMA-P) and 27-item checklist published in the PRISMA 2020 statement.
17
Using the population, intervention, comparison, and outcome (PICO) framework, the PICO components that guide this study are as follows: - Population: U.S. adults receiving health care services between 2020 and October 2022 - Intervention: Expansion of telehealth services due to and during the COVID-19 pandemic - Comparison: Rates between sociodemographic groups - Outcome: Telehealth utilization, access and/or outcomes during COVID-19
SEARCH PROCESS
The following databases were searched for studies on expanded telehealth utilization during the COVID-19 pandemic: Litcovid, PubMed, Web of Science, and MEDLINE on EBSCOhost. Results were saved and managed in Zotero reference manager version 6.0.10. Records were saved to separate folders for each database, within the same reference library, which allowed for identification and removal of duplicate results across databases. Duplicates were removed, prioritizing keeping versions with full-text, and/or full abstracts imported to Zotero.
In each database, the following search terms and Boolean operators were used:
(((TS = (pandemic OR COVID-19 OR coronavirus OR “SARS-CoV-2” OR 2019-nCoV)) AND AB = (adult)) AND TS = (telehealth OR telemedicine OR teleconsult*)) AND AB = ((sex OR sexual* OR race OR gender OR age OR socioeconomic) AND (demographic OR disparit* OR inequal*) AND (use OR utilization OR access))).
When searching in Litcovid, the COVID-related search terms were omitted as the database is only home to COVID-related studies and therefore these filters are not needed. Across all databases, additional filters were manually applied including location or geography (United States), English language, and publication date after March 1, 2020. Supplementary Appendix SA1 outlines search terms, dates searched, filters that were applied and number of studies retrieved from each database.
INCLUSION/EXCLUSION CRITERIA
Only original, peer-reviewed studies were included for this review including qualitative studies, those using secondary data, survey data, or data collected from electronic medical records (EMRs) or billing codes. Per the PICO framework, only studies on adult patients, or any U.S. adult receiving health care services, were included. Those that included adults but also had a pediatric sample were dropped. Although examination of pediatric telehealth usage during and following the COVID-19 pandemic may be an important indicator of access to and use of these expanded services, inclusion of pediatric telehealth use is beyond the scope of this review and should be explored in future research. Furthermore, this review only included studies in which telehealth or telemedicine was the primary mode of health care delivery, or those that compared telehealth recipients with non-telehealth recipients.
Studies that were not conducted in the United States, were in a language other than English, had subjects other than U.S. adults (i.e., pediatric samples), and did not focus on the access to, receipt, or utilization of telehealth services were not included in this review. In addition, this review did not include other systematic reviews, meta-analyses, or literature reviews on telehealth utilization. Conference abstracts, presentations, case study reports, and reports on procedural guidelines for telehealth delivery, or studies using adult caregiver reports of children's telehealth use were also not included.
SCREENING PROCESS
Before screening each study, duplicates were removed from the total list of records across databases. Of the n = 129 studies saved to Zotero in the initial search, n = 45 duplicates were removed. Each abstract was screened for eligibility based on the PICO components. A total of n = 84 abstracts were reviewed. This screening phase was completed by two reviewers, with an inter-rater agreement of 76%.
After screening abstracts, n = 47 studies were included in the retrieval step. A total of n = 2 studies did not have full-text available, and therefore were not retrieved. A final screened sample of n = 45 reports was assessed for eligibility by reading the full text of the study (Fig. 1).
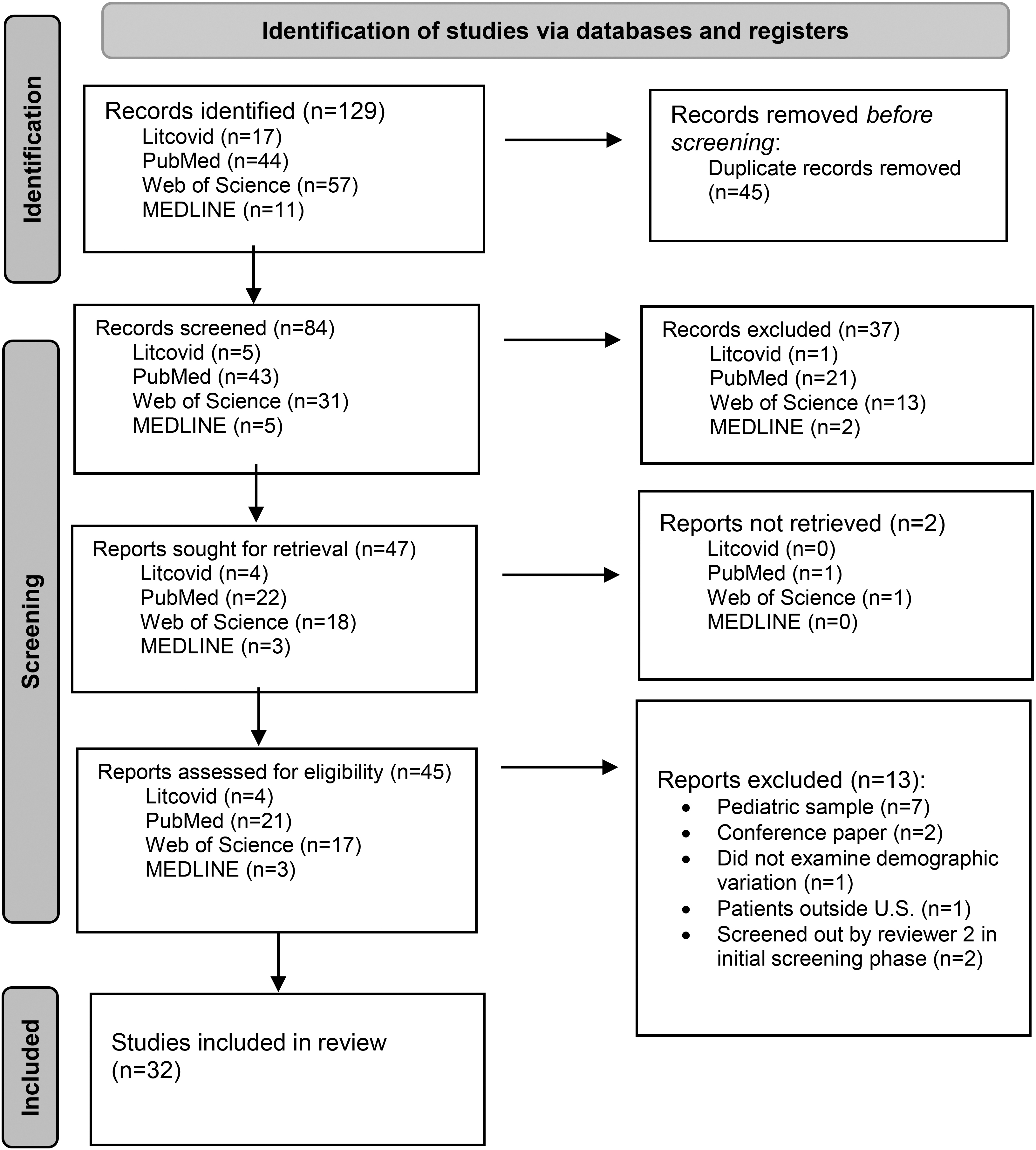
From: Page et al. 17
ANALYTIC PLAN
The full-text version of each study included in this review was read, and data were extracted into a customized data extraction form in Excel (Supplementary Appendix SB2 for example form). The following information was extracted: the date of data extraction, the reference citation, publication type (i.e., journal article), the study type, sample size, participant type, population (P), type of intervention (I), type of comparison (C), type of outcome (O), aim of study, study design, date(s) study conducted, setting, results, and which database the study was obtained from.
Results
CHARACTERISTICS OF INCLUDED STUDIES
The final sample of studies included in this review was n = 32. The included studies were published across 3 years: 2020 (n = 3), 2021 (n = 14), and 2022 (n = 15). Studies were published in 26 different academic journals. The studies covered a wide range of medical specialties and patient populations. All studies used adult populations such as Medicare beneficiaries, low income or un/underinsured adults, and veteran populations. Two studies relied on data from nationally representative surveys; however, the majority were retrospective cohort studies using EMR data.
FINDINGS ON SOCIODEMOGRAPHIC DIFFERENCES IN TELEHEALTH TRENDS DURING COVID-19 PANDEMIC
Each study included in this review addressed the role of patient demographics and characteristics in at least one of eight identified areas of inquiry: telehealth utilization or outcomes by modality (video vs. telephone) during COVID-19 (n = 9), telehealth utilization versus nonutilization during COVID-19 period (n = 9), telehealth utilization during COVID-19 period versus in-person health care utilization pre-COVID-19 (n = 5), telehealth versus in-person utilization during COVID-19 period (n = 6), perceived or reported telehealth access during COVID-19 (n = 6), satisfaction with telehealth during COVID-19 (n = 4), telehealth utilization and health outcomes during COVID-19 (n = 3), and telehealth utilization versus nonutilization during and before COVID-19 period (n = 1).
TELEHEALTH ACCESS AND UTILIZATION DURING COVID-19 PANDEMIC
Sociodemographic differences were revealed when comparing those who used any telehealth during the COVID-19 pandemic versus those who did not. However, findings were inconsistent; although some found no significant racial or ethnic differences in multivariate analyses predicting telehealth use, 18,19 racial/ethnic differences were noted with respect to virtual care use among older Medicare patients, 20 –22 adults diagnosed with COVID-19, 23 and adult cancer patients. 24 Results showed that Hispanic 23 and non-English–speaking patients 24 had a decreased odds of telehealth utilization during the pandemic, whereas other analyses found that Hispanic Medicare beneficiaries had a higher odds of telehealth utilization after controlling for technology access. 20 Meanwhile, non-Hispanic Black patients were more likely to use virtual primary care, 23 had a higher prevalence of telehealth to replace regularly scheduled visits, 21 and were more likely to use telehealth when offered 22 compared with non-Hispanic Whites and other race/ethnicities.
Among studies specifically comparing rates of telehealth to in-person health care utilization during the COVID-19 pandemic, findings again showed mixed results regarding racial and ethnic differences in utilization. Although one study found that Black adults were more likely to report preference for in-person care than other races, 25 another found that older Black adults both represented a higher proportion of those using virtual primary care and had a higher odds of utilization compared with younger White patients. 26 And, although race/ethnicity significantly differed between telehealth and in-person patients seeking care at a safety-net hospital, there were no demographic differences in whether a telehealth visit was missed or attended among those who sought telehealth care. 27
Using a nationally representative sample of U.S. adults, Narcisse et al. 18 found that other demographic factors, including gender, marital status, education, rurality, and income predicted telehealth utilization during the pandemic. Age, income, and education were again found as a significant predictor of telehealth versus in-person health care utilization by Predmore et al. 25 in a separate nationally representative sample of U.S. adults.
TELEHEALTH UTILIZATION BY MODALITY
Several studies examined how rates of telehealth utilization differed by visit modality and the likelihood of utilizing each modality by patient demographics and other factors. There were significant age, racial/ethnic, and gender differences with respect to telehealth modality. Findings across studies consistently showed that age was a significant predictor of video telehealth utilization, where older age was negatively associated with video telehealth use compared with telephone-only. 28 –33
Included studies also highlight racial and ethnic differences in telehealth use by modality. When compared with White patients, Black patients were more likely to have an incomplete (“no-show”) or “failed” video visit 28 ; non-White and Hispanic individuals were less likely to use telemedicine in general 29 and less likely to use video compared with Whites and non-Hispanics 32,33 ; and Black patients were more likely to have failed video visits or convert to audio-only, compared with Whites. 30
Gender differences in telehealth utilization by modality were also analyzed. One study of patients receiving virtual intensive outpatient treatment for substance use disorder found that women were more likely to participate in an internet-only program compared with men who favored hybrid in-person and internet programming. 34 Men were less likely to use video for a rheumatology visit during the pandemic. 32 However, Shah et al. 30 and Wegermann et al. 33 found that sex did not predict visit modality.
HEALTH OUTCOMES AND PATIENT SATISFACTION
Several studies sought to examine how patient characteristics were associated with health outcomes and patient satisfaction of telehealth during the COVID-19 pandemic. Although reported satisfaction with telehealth was generally high, there were some differences by participant sociodemographics. Among older adults in a Massachusetts health system, non-White patients reported significantly lower satisfaction scores than White patients, as well as patients with comorbidities compared with those without. 35 Although there were no age or race differences with reported satisfaction among patients of an urban HIV clinic, women reported greater concern with telehealth than men. 36 Another study found that there was a significant interaction between age and “tech-savviness,” where tech-savviness had more effect on satisfaction among younger patients. 37
When analyzing patient outcomes associated with telehealth utilization, studies again found demographic differences. For example, Ryskina et al. 26 found that both older and Black patients who used telehealth had a higher risk of hospitalization within 14 days of their virtual visit compared with younger and White patients. Another found that male and Black patients had a higher risk of death following virtual urgent care visit compared with female and White patients. 38 Additional research found that, among patients diagnosed with COVID-19, being male, older, and having higher comorbidities were associated with a greater odds of intensive care unit admission following virtual hospitalization. 39 Black patients also had a higher odds of virtual hospitalization and inpatient admission following COVID-19 diagnosis and virtual urgent care observation when compared with Whites. 39
ACCESS TO TELEHEALTH SERVICES DURING COVID-19
Another important line of inquiry among the selected studies was perceived or reported access to telehealth services during the pandemic. In two studies, access was measured by whether older Medicare beneficiaries' health care provider–offered telehealth services. 21,22 Younger beneficiaries were more likely to report that their health care provider offered telehealth services, as were those living in metro areas compared with rural areas, and those living in U.S. regions other than the South. 22 Men had a decreased odds of their provider offering telehealth compared with women. 22 The second study had similar results, finding younger, higher income, urban patients, with access to internet, technology device, or with previous videoconferencing experience, as more likely to report their health care provider offered telehealth during the COVID-19 pandemic. 21
Similarly, in a study among veterans living in a southern rural state, Padala et al. 40 found that internet access and willingness to utilize telehealth was lower among rural veterans when compared with those living in nonrural areas. Education also significantly influenced access to telehealth services. In another study that assessed perceived difficulty in access to telehealth for contraception services, those living as food and housing insecure had a higher odds of reporting difficulty in access when compared with food and housing secure participants. 41
TELEHEALTH DURING COVID-19 PERIOD VERSUS PRE-COVID-19 HEALTH CARE UTILIZATION
Several studies sought to compare telehealth service utilization during the pandemic with health care utilization in prepandemic study periods, when in-person health care was the primary mode of health care delivery. Using nationally representative health claims data, Jaffe et al. 42 compared the composition of patients using telehealth in March 2020 with patients receiving in-person care in March 2019. Sociodemographic factors predicted telehealth utilization in 2020 in multivariate analyses. 42 When comparing male sexual health patients using video telehealth in April 2020 with patients' utilization of in-person services in April 2019, race/ethnicity and public insurance status did not significantly differ between the two cohorts. 43
However, older patients were significantly less likely than younger patients to have a telehealth visit in 2020, as were those who lived a further driving distance from the health clinic. 43 When examining “MyChart” activation among rheumatology patients, Sun et al. 44 found that although there were demographic differences in utilization within prepandemic and pandemic study periods, demographic trends in MyChart use were similar across both cohorts. Thomason et al., 32 however, did find differences in patient composition between pre- and during pandemic rheumatology telehealth use. Compared with the prepandemic study period, those who had a visit during the pandemic were more likely to be established patients, have used the patient portal in the past, identify as Native Hawaiian or Pacific Islander, prefer Spanish language, or have self-pay insurance. 32 Wegermann et al. 33 also found a statistically significant difference in patient composition between those who had visits between January 1 and February 29, 2020 versus those who completed a telehealth visit between April 1 and May 31, 2020.
Discussion
This systematic review sought to identify, categorize, and synthesize the findings of studies addressing demographic disparities in telehealth access, utilization, and/or outcomes following the expansion of these services owing to the COVID-19 pandemic. This study adds to the growing body of literature in this area by providing an updated description of the current state of research, synthesizing the findings of 32 peer-reviewed research articles, and identifying areas for future research.
Included studies were published over the course of 3 years, in over two-dozen academic journals focusing on several specialty care areas. Although two relied on data from nationally representative surveys, most were retrospective cohort studies using EMR data. The wide range of journals and specialties included in this review demonstrate the far-reaching impact of the COVID-19 pandemic and subsequent expansion of telehealth services on the health care industry in the United States.
Studies were categorized as focusing on at least one of the eight different areas of inquiry: (1) telehealth versus in-person use during the pandemic, (2) telehealth versus nonuse during the pandemic, (3) telehealth using during the pandemic versus in-person use before the pandemic, (4) telehealth versus nonuse before the pandemic, (5) telehealth modality, (6) satisfaction with telehealth, (7) access to telehealth, and (8) outcomes associated with telehealth utilization. Findings from the included studies revealed sociodemographic disparities within each area of inquiry, which will be discussed hereunder.
SYNTHESIS OF STUDY FINDINGS
Sociodemographic differences were widely noted with respect to each of the different areas of inquiry identified in this review. However, although some findings were robust, appearing repeatedly across studies, others were less consistent. For example, studies did not reach consensus on how rates of telehealth utilization compared between Hispanics and non-Hispanics. 20,23,24 It is possible that these inconsistencies are, in part, owing to differences in study populations. For example, although Choi et al. 20 used nationally representative Medicare data, other studies measured primary care visits within a regional health care network or use by adult cancer patients of an academic health center.
Similarly, it was unclear how gender predicted telehealth utilization or modality preference. 32,34 Women's tendency to use internet-only programs rather than a hybrid or in-person model may reflect women's behaviors during the pandemic; research from early in the pandemic found that women were more likely than men to believe that the pandemic was a serious health problem and were more willing to adhere to social-distancing restrictions and guidelines. 45 In addition, men and women may have different levels of health and/or digital literacy, contributing to differences in help-seeking as well as comfort with modality of care. 46 –48 However, the role of both social-distancing behaviors and/or digital health literacy in the association between gender and telehealth utilization remains underexplored and is an area for future research.
Although not necessarily a robust finding throughout this review, it is worth noting that studies that included health outcomes following telehealth utilization as a study outcome found that men had worse health outcomes than women. 38,39 Research on men's help-seeking shows that men seek help for psychological and medical health services later and at lower rates than women and report low rates of attending regular health check-ups, which may contribute to poorer health outcomes when they do seek care services. 49,50 Men's help seeking behaviors are often explained in the context of traditional gender roles and masculinity; men are socialized to be self-reliant and independent—traits that are inconsistent with seeking help for physical or psychological health concerns. 51,52 Although it is unclear whether past research findings are indicative of gender disparities in telehealth utilization and related health outcomes, it seems likely that additional research will reveal gender gaps in how adults access, use, and experience telehealth services.
Inconsistencies across studies may also point to the dynamic nature of telehealth technology and demonstrate how trends in access, utilization, and outcomes are rapidly changing. Studies included in this review were published across 3 years – 2020, 2021, 2022—during which there were significant shifts in policies related to guidelines and accessibility for telehealth service use. For example, although a national emergency order was issued, stay-at-home and disaster or public health emergency orders and declarations varied considerably by state. As of February 2023, only five states (CO, GA, IL, NM, and TX) continued to have emergency declarations in place and each was slated to end by May 2023. 53 These emergency orders allow for changes in spending and definitions associated with health care delivery. States have considerable control over telehealth reimbursement policies—another area that continuously and rapidly evolved during the pandemic 54 and that plays an important role in telehealth utilization. 55 –60
Broader state- or institutional-level factors that affect telehealth utilization were not widely incorporated in studies in this review (see Figueroa et al. 2021, which adjusts for Medicaid expansion status, and Predmore et al., which adjusts for out-of-pocket costs, for exceptions). There are several moving parts with respect to regulations surrounding telehealth access and utilization. It is possible that a lack of consensus across study findings reflects these broader forces and the differential impact they have on certain patient populations, yet they remain underexplored. Additional research in this area should seek to measure the role of state-level telehealth policies in the relationship between individual-level factors and telehealth access, utilization, and/or outcomes.
Study findings were more robust with respect to racial, socioeconomic, rurality, and age disparities in telehealth outcomes. Findings are consistent with past research showing well-documented and persistent racial differences in general health care utilization and outcomes. 61 –63 Racial minorities more often receive inadequate care 64 and, as seen during the COVID-19 pandemic, have poorer health outcomes including higher COVID-19 incidence and age-adjusted death rates. 15
Other sociodemographic predictors, including rurality, age, and socioeconomic status (SES) also contributed to differences in telehealth utilization and access. Rural areas in the country are often designated as health professional shortage areas, meaning they lack enough providers—especially specialty care providers—to adequately treat rural patients. 65 In addition, the “digital divide” disadvantages rural residents who face structural barriers, like lack of access to high-speed broadband internet access, preventing them from having widespread access to telehealth services. 66,67 Consistent with research on rural health care access and utilization, the studies included in this review found lower levels of telehealth access and utilization by rural adults compared with more urban patients. Although expanded telehealth has the potential to close the health care access gap between rural and urban adults, findings in this review suggest that there are still significant barriers to access in rural areas.
Included studies also pointed to barriers to access faced by older adults and low SES patients. These findings may speak to digital literacy deficiencies among older adults, thus limiting their ability to use telehealth technologies. Future research should continue to consider how age—in conjunction with digital and/or health literacy—impacts access to telehealth services as the United States continue to move forward with virtual health technologies in the digital age. SES, measured by education and income, also has a strong effect, historically, on health care access and outcomes. 68 Across included studies, SES was found to be a predictor of access to telehealth services with low-SES adults less likely to report their provider offered telehealth. Additional research in the area of expanded telehealth access should continue to monitor how SES impacts access and utilization rates among different populations, to best inform health care policy decisions.
Findings that are more robust across studies may reflect enduring sociodemographic differences in health care access, utilization, and outcomes more broadly—supporting a fundamental cause perspective. 68 –70 Racial differences in health care access, utilization, and outcomes are often explained in the context of structural racism; residential racial segregation can impact healthy behaviors, reduce access to medical care, and increase exposure to environmental conditions. 61 Net of SES and other demographic predictors, race and racism are fundamental causes of health inequalities in that race and/or racism influences multiple disease outcomes, affects disease outcomes through multiple risk factors, influences access to flexible resources that can be used to avoid risks or minimize consequence of disease, and these associations are reproduced over time. 68 –70
Fundamental causes of inequality persist net of advances in medical technology; for example, the gap in cancer survival rates for racial and ethnic minority groups widen when cancer is one that is more “treatable” because race affects access to resources (i.e., treatment). 71 This may explain why, although studies found Black patients to have a higher odds of telehealth utilization, their health outcomes following use of these services were poorer than their White counterparts. Despite advances in medical technology (i.e., telehealth) that, ideally, expand access to care to more individuals, racial differences in access to flexible resources—money, power, prestige, knowledge, and social connections 70,72 —influence differential use of (for example, lower rates of video-enabled telehealth among minority groups) and outcomes associated with these technologies. Different rates of access and use by SES can also be explained using fundamental cause theory.
These findings may point to enduring differences in access, use, and health care outcomes that persist despite the expansion of telehealth services during the COVID-19 pandemic. It is important that additional research looks to confirm trends in sociodemographic differences in a range of health outcomes associated with telehealth so health policymakers and health care providers can take steps to better serve under-resourced and medically underserved populations.
AREAS FOR FUTURE RESEARCH
The studies included in this review provide a comprehensive snapshot of the research on telehealth access, utilization, and outcomes in the wake of expansion during the COVID-19 pandemic. There are, however, research areas left unexplored. First, only a small number of studies included in this review used nationally representative survey data to assess trends in telehealth use. Although the use of an EMR or other clinical data provides an insight on health care utilization among patients receiving specialty care or within a particular health care system, these data may not capture those who do not have a regular health care provider.
Using data from the Medical Expenditure Panel Survey, Levine et al. 73 found that receipt of primary care significantly decreased between the years 2002 and 2015 for those aged 30–59 years. In 2015, ∼75% of American adults reported a source of primary care and, those who were male, Latino, Black, Asian, uninsured, or lived in the southern United States were significantly less likely to report having a primary care visit during the calendar year. 73 Using nationally representative survey data, such as the National Health Interview Study 74 or the Household Pulse Survey, 75 may better capture data on telehealth utilization among those who are uninsured or do not belong to a health care system. Future research on telehealth access, utilization, and health outcomes during and following the COVID-19 pandemic should incorporate nationally representative samples to better capture a wider range of adults in the United States.
Second, the studies included in this review each address sociodemographic factors associated with telehealth use individually. Although useful to help understand group-level differences in telehealth utilization, individuals occupy more than one social status and therefore may not experience access, utilization, and outcomes universally. Less attention has been paid to how sociodemographic factors may interact to influence telehealth access or utilization. Intersectionality, or the theoretical framework used to conceptualize how multiple oppressive social identities (e.g., race, gender) intersect to reproduce injustices, 76 –78 is important to incorporate into research on health care access, utilization, and outcomes.
The few studies that did include interactions between sociodemographic predictors found significant interactions between race and telehealth utilization when examining risk of hospitalization, 26 race and insurance type when predicting telehealth utilization, 39 and age and “tech-savviness” when predicting satisfaction with telehealth. 37 These findings suggest that incorporating an intersectional framework to test for theoretically meaningful interactions from the start—rather than as an afterthought—may reveal disparities in how telehealth is accessed, used, and experienced by those with multiple, overlapping, oppressive social identities.
Conclusion
The onset of the COVID-19 pandemic prompted a large-scale, rapid shift to telehealth services as a means to continue to provide patients with care and prevent the spread of disease. This review sought to synthesize the growing area of research on telehealth utilization and specifically understand how sociodemographic factors influenced telehealth access, utilization, and health outcomes during the COVID-19 pandemic. Results from the studies point to racial/ethnic, gender, age, residential location, and socioeconomic disparities in several aspects related to expanded telehealth services.
Although some findings were inconsistent and call for additional research, others were more robust pointing to enduring sociodemographic differences in access, use, and health outcomes more broadly that persist despite expanded access to telehealth services during the COVID-19 pandemic. Although the included studies utilized a wide range of samples to assess telehealth use, few relied on nationally representative datasets or took an intersectional approach to examine how multiple or overlapping identities may uniquely predict telehealth-related outcomes. Future research should continue to investigate sociodemographic differences in access to, use of, and health outcomes associated with telehealth to help reduce barriers to care, improve health outcomes, and inform health policy.
Footnotes
Acknowledgments
The author acknowledges the efforts of Adrienne R. Brown, PhD, who served as a second reviewer for this study. The author also acknowledges Heather A. Turner, PhD for her guidance during this study.
Disclosure Statement
No conflicts of interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix Table SA1
Supplementary Appendix Table SA2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.