
Abstract
Background:
The COVID-19 pandemic accelerated telehealth adoption, but its effects on care quality and costs remain unclear. This study evaluates a remote patient monitoring device's impact on utilization and spending.
Methods:
A large insurer launched a pilot program involving 2,880 households, representing 6,731 members in three states. Administrative claims data compared participant households to a matched group lacking necessary contact information for participation.
Results:
Participants had a 0.19 per member (p = 0.03) increase in telehealth visits and a 0.19 per member (p = 0.08) decrease in outpatient in-person visits relative to nonparticipants during the post 6-month period. No significant differences were observed in total outpatient and emergency department visits or total spending. Subgroup analyses revealed a significant reduction in telehealth visits followed by in-person outpatient visits in households with younger children (−9.1%; p < 0.05).
Conclusion:
This evaluation suggests that remote devices may boost telehealth utilization without increasing costs.
Introduction
The COVID-19 pandemic accelerated telehealth use and significantly expanded patient access to virtual medical care. 1,2 However, without the ability to conduct a hands-on physical examination, the findings are mixed on the extent to which physicians can accurately diagnose and treat patients virtually. 3 –5 Concerns exist about the effectiveness, accuracy, and efficiency of telehealth, including the possible need for additional in-person follow-up care. 6 –8
A growing topic of interest, remote patient monitoring (RPM) technologies may have the potential to improve aspects of virtual care. RPM leverages connected electronic tools (stethoscope, temperature sensor, camera/scope) to noninvasively record and wirelessly transmit common physiological parameters to health care providers. 9,10 Emblematic of RPM technology, we evaluated a U.S. Food and Drug Administration-cleared, handheld electronic device (including stethoscope and camera with scope for throat and ear exam) that facilitates physical exams of the heart, lungs, skin, ears, throat, abdomen, and body temperature via live video chat with a clinician. 11 RPM devices have the potential to change the telehealth landscape; however, because these tools are a relatively new care option, published literature on the real-world impact of RPM is lacking. The primary objective of this study is to evaluate the impact of the RPM technology program on health care use and spending.
Methods
In December 2020, a large health plan launched a pilot program for a subset of commercially insured members in three states. The program targeted households with children younger than 12 years, chronic conditions (e.g., asthma, heart disease), and high emergency department (ED) use. Members were invited to participate via a short message service text message or e-mail. The pilot participants were shipped a complimentary RPM device. Members could schedule an RPM-enabled visit via LiveHealth Online (LHO), a complimentary 24/7 virtual visit platform that was offered to all health plan members regardless of RPM device receipt during the COVID-19 pandemic.
This retrospective cohort study used data from participant households compared to a nearest neighbor 1:1 propensity score matched group of households who were eligible for participation but did not have the required contact information (nonparticipants). Using an intent-to-treat approach, medical and pharmacy utilization and spending were compared between participants and nonparticipants. Medical utilization included outpatient visits; outpatient by category of in-person, telehealth, and primary care; ED visits; ED visits by category of severity; and proportion of telehealth visits with an in-person outpatient or ED visit for the same diagnosis within 10 days. Medical and pharmacy spending was operationalized as the total allowed amount. The follow-up period for all outcome measures was 6 months.
Change score models explored the association of the RPM pilot with health care use. Using generalized linear models with a normal distribution, 6-month change scores were regressed on baseline characteristics and a group indicator. Positive group indicator values indicated a greater increase or smaller reduction in utilization or spending among participants compared to nonparticipants, whereas negative values indicated a greater reduction or smaller increase from baseline to follow-up. All regression models included baseline characteristics such as household size, median age, percent female insurance subscriber, geographic regions, Elixhauser comorbidity index, and common chronic conditions. 12 To prevent extreme cost outlier influence, cost data were winsorized at the 99th percentile. Subanalyses assessed treatment heterogeneity for households with children younger than 7 years, no prior telehealth use, chronic conditions, and baseline ED use. Lastly, we assessed outcomes among the subpopulation of participant households that used the device during the follow-up period.
All study measures evaluated enrollment data and medical and pharmacy claims from June 2020 to June 2021. Statistical significance was set at 0.05. Researchers accessed a limited dataset with full compliance to the Health Insurance Portability and Accountability Act. This study was nonexperimental and was exempt from investigational review board approval.
Results
There were 2,880 participating and 69,709 nonparticipating households, representing 6,731 and 134,714 members, respectively. During the first 6 months of the program, 299 participating households received 399 RPM-enabled visits. After propensity score matching, the 2,754 participating and 2,754 nonparticipating households were similar in household size, number of children, age distribution, metropolitan status, Agency for Healthcare Research and Quality socioeconomic index, chronic conditions, and baseline ED and telehealth use (Table 1). Participating households experienced a 0.19 per member (p = 0.03) increase in telehealth visits, a 0.02 per member (p < 0.01) increase in LHO visits, and a 0.19 per member (p = 0.08) decrease in outpatient in-person visits relative to nonparticipants (Fig. 1). However, there were no statistically significant differences in total outpatient visits, outpatient primary care provider visits, total ED visits, ED visits by category of severity, proportion of telehealth visits with an in-person follow-up visit, or medical and pharmacy spending (Table 2).
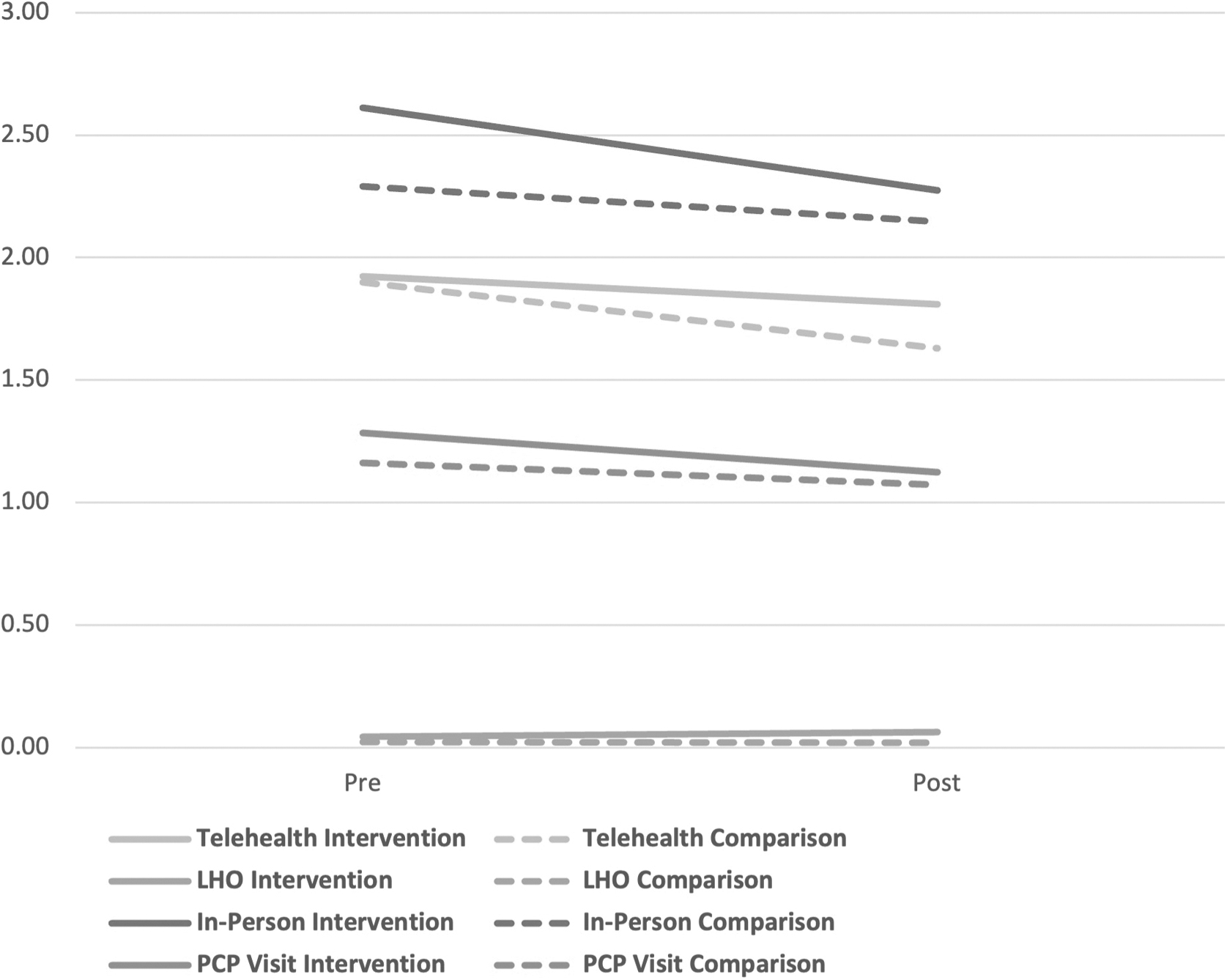
Average number of outpatient visits per member during 6-month pre- and postintervention periods, by type of outpatient visits. LHO, LiveHealth Online; PCP, primary care provider.
Six-Month Baseline Characteristics: Preremote Patient Monitoring Pilot Enrollment
Higher scores indicate higher risk for ED visits in next 3 months.
COPD, chronic obstructive pulmonary disease; ED, emergency department; LHO, LiveHealth Online; LIER, a proprietary machine learning model which predicts likelihood that a member will visit the ED in next 3 months; SD, standard deviation; SES, socioeconomic status; Std Diff, standardized difference.
Unadjusted and Adjusted Utilization Outcomes
p < 0.05, ** p < 0.10.
PCP, primary care provider.
In our subanalyses, LHO visits increased significantly across all household types (Table 3). In addition, we find a significant reduction in the proportion of telehealth visits with an in-person outpatient follow-up visit among participant households with younger children (−9.1%; p < 0.05). We also find a trend that decreases in outpatient in-person visits are concentrated among households with chronic conditions (−0.25 per member; p < 0.10). The smaller subsample of participant households that used the RPM device experienced a significant increase in LHO visits with no detectable differences in other outcomes.
Subgroup Analysis of Health Care Utilization and Costs
All outcomes are shown as the adjusted increase or decrease in the pilot participants group relative to the comparison group (reference). Out of 299 households which received RPM visits, we were able to match 230 with a comparison household.
p < 0.05, ** p < 0.10.
RPM, remote patient monitoring.
Discussion
While use of telemedicine in the United States was minimal before COVID-19, interest in and implementation of telemedicine expanded rapidly during the crisis. However, the impact of telehealth on quality and cost of care is an uncertain and evolving topic. This evaluation suggests that remote devices may increase uptake of telehealth without increasing costs. However, in interpreting these results, one must consider the effect of the actual device versus intervention-related communication in promoting LHO use.
Due to small sample sizes, the impact of the RPM device on visit quality requires additional analysis. Our subanalyses suggest that RPM devices may be most efficiently and effectively used within targeted populations, such as younger children and patients with chronic disease. Further research should examine the impact of the RPM device on patient satisfaction and disparities in care access.
Footnotes
Acknowledgments
The authors would like to acknowledge Shani Fargun for assisting with pilot specifics and data, and Elizabeth Marks for assisting with editing and formatting of the research letter.
Authors' Contributions
A.O. and M.R.: Conceptualization, methodology, investigation, formal analysis, and writing. Y.C.: Conceptualization, methodology, investigation, formal analysis, visualization, and writing. M.R.: W.C.: Conceptualization, methodology, investigation, writing–review, and editing.
Disclosure Statement
None disclosed.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.