
Abstract
Background:
The COVID-19 pandemic significantly increased telehealth adoption. Rural communities experience challenges relating to telehealth, including a shortage of clinicians, low health literacy, mistrust of medicine, and limited technology access, yet rural perceptions have not been a subject of robust study. The setting of this study was a rural Midwestern family medicine clinic within an academic health system.
Methods:
Surveys were given to all patients of age 18 or older visiting the clinic over a one-week period. Those who expressed interest were contacted for a semistructured interview. Descriptive statistics and chi-square testing were used to analyze survey results for significant relationships, while interview transcripts were analyzed for themes.
Results:
Of respondents, 27% indicated prior telehealth use and were more likely to prefer telehealth visits (p = 0.03). Perceptions of telehealth were sorted into themes, including scope of care, convenience, and technology. Telehealth was preferred for discussing test results or mental health. Barriers such as travel time and transportation access favored telehealth. Although more convenient, telehealth was found to be less effective for relationship building. The absence of physical examination during phone visits was a concern. Phone visits were more prevalent due to failure of video-based technology.
Conclusions:
Despite the potential to address these unique challenges in rural communities, telehealth acceptance is poor. Barriers such as accessibility of technology can be improved through governmental and health systemwide measures. Future work can help develop interventions that counter negative perceptions of telehealth while increasing interest and uptake in rural communities.
Introduction
The COVID-19 pandemic drastically altered the health care landscape, causing profound changes in care delivery. Health care organizations, grappling with uncertainties surrounding viral transmission and the need to isolate patients, embraced telehealth as they sought to provide care while maintaining financial stability. 1 In response to the early pandemic, the Centers for Medicare and Medicaid Services provided support for rapid implementation of telehealth service coverage. Notably, in 2016, 88.2% of primary care practitioners did not provide any telehealth services. 2 Within 2 months of the COVID pandemic, this percentage of nonusers was lowered to 9%, marking a substantial transformation in telehealth adoption. 3 Reports indicate that there was a 78-fold increase in telehealth-based outpatient visits from February 2020 to April 2020. 4 Among older adults, the number of telehealth users grew over fourfold compared with prepandemic numbers. 5 After this initial surge, telehealth utilization has subsequently declined, although there remains variation across communities and health systems. 6
As clinicians and facilities are gradually adapting to the postpandemic world, there is a need to understand the role of telehealth in the health care ecosystem. Interest in telehealth has grown rapidly due to its many benefits, including increased flexibility for care delivery, reductions in travel time to the clinic, better long-term care management outcomes in certain cases such as anticoagulation management, and nutrition and rehabilitation consultations. 7
Clinicians report that patients using telehealth tend to show increased patient engagement, higher follow-up appointment adherence, and improved treatment plan adherence. 3 Furthermore, some reviews have suggested that telehealth utilization may lead to reduced health care system costs in the short to medium term, although cost-effectiveness analyses vary across different studies, with some indicating potential cost increases. 8
Despite these advantages, many have expressed concern over some of the drawbacks, including the inability to perform a traditional physical examination and lack of face-to-face contact contributing to a less robust therapeutic relationship between the clinician and patient. 9 Common chronic conditions requiring laboratories and biometrics such as blood pressure and cholesterol testing create additional logistical hurdles. 2 This leads to questions about telehealth's current viability in primary care.
Rural populations face distinct health disparities, with rural Americans facing a life expectancy that is on average 2 years shorter than their urban counterparts. 10 These disparities arise due to obstacles to care in rural communities. These obstacles include geographic distance to access care, limited access to needed care, poor care coordination, economic hardship, costs, and cultural barriers associated with seeking care. 11
Additionally, common obstacles to telehealth uptake include a lack of clinicians, low health literacy levels, a lack of trust in medicine, and limited access to technology and infrastructure required for telehealth services. 12 –14 While telehealth holds significant promise in addressing these disparities by reducing access barriers to health care and health services, 15 its implementation in rural primary care settings has proven to be particularly challenging. 16
Previous studies have presented conflicting results on patient preferences for telehealth. 17,18 However, our experience with rapidly declining telehealth rates following the pandemic supports the challenges associated with its uptake. This variability underscores the complexity of integrating telehealth into rural health care systems.
While current literature has focused on health care systems' and clinicians' perspectives on telehealth utilization, there is a scarcity of work evaluating patient preferences that underpin the adoption and viability of telehealth in rural areas. 9 Recent work investigating the patient experiences of telehealth shows that expectations about appropriate use are varied. 19 While this study was an important step in understanding patient perspectives, it does not capture the specific challenges and needs of a rural primary care population.
Understanding these perspectives is critical to health care systems as they seek to effectively cater to the needs of rural patient populations. Therefore, this study sought to elicit patient perspectives on telehealth in a rural primary care clinic associated with an academic health system. Our work aims to extract insights that could further refine telehealth care and align it more closely with rural populations' preferences, perspectives, and needs.
Methods
SUBJECTS AND TESTING
The setting is a rural primary care clinic associated with an academic health system. The clinic is located in a micropolitan community (rural-urban commuting area 4), but the catchment area extends to the surrounding county, encompassing a diverse range of rurality levels ranging from RUCA 2 to RUCA 10.
Eligible participants were identified as patients being seen for a visit between February 14 and February 18, 2022. On-site patients were given a telehealth survey by check-in staff before the rooming process. Telehealth patients were given a link and a QR code in their visit summary by the medical assistant performing the remote rooming process. The survey asked participants about their utilization and perspectives on telehealth and demographic information. If they were willing to participate in a telephone interview, contact information was also collected.
A total of 138 of 348 patients seen in the clinic that week completed the survey. Of those 348 visits, 319 were on-site visits (137 patients completed the surveys) and 29 were telehealth visits (1 patient completed the survey). Of patients who completed surveys, 24 indicated a willingness to be contacted for a structured interview and 15 of those patients ultimately were reachable and completed the interview (Fig. 1).
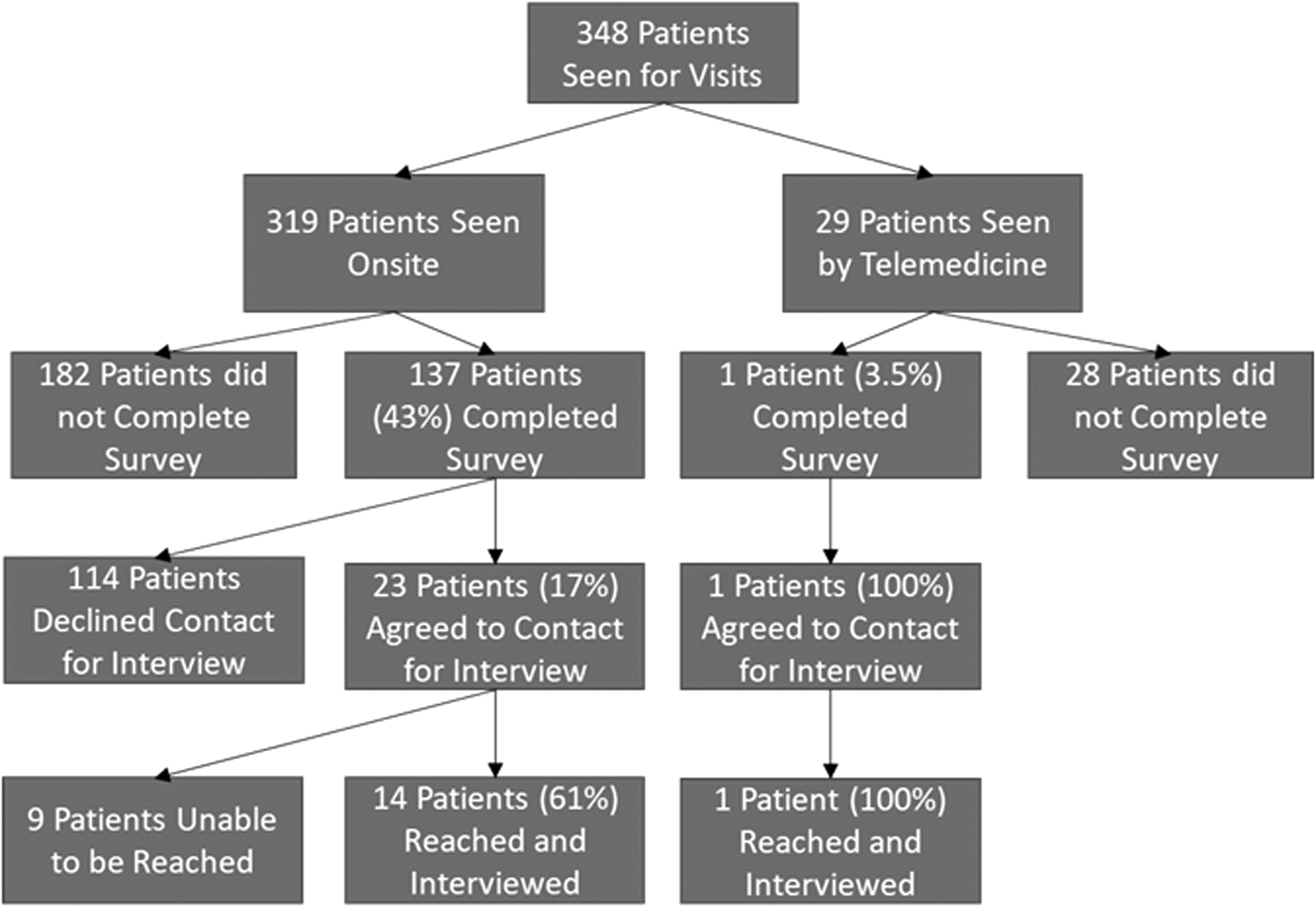
Recruitment summary.
Interested parties were contacted by phone for a 15-min semistructured interview utilizing seven questions about the participant's experience with telehealth (Table 1). The rate of telehealth visits during the recruitment week (8.3%) was consistent with telehealth volumes at that time. Despite high levels of telehealth earlier in the pandemic, these rates dropped considerably in the following years.
Qualitative Interview Questions and Probes
The study was confirmed to be exempt by the University of Wisconsin Madison School of Medicine and Public Health Institutional Review Board. Due to the minimal risk, consent forms were not required. However, verbal consent was received from interviewed patients before the structured interview.
PROCEDURES
Interviews were conducted by a 4th-year medical student who was trained in the structured interview process. The student called interested participants and conducted semistructured interviews, focusing on telehealth, its benefits, and its limitations. With the consent of these participants, the student recorded these audio conversations with the iPhone application, Rev, or macOS's Voice Memos application and transcribed them into text using Microsoft Word 365 transcription software.
Transcripts were reviewed and edited for accuracy immediately after the conclusion of the interview. A total of 15 semistructured interviews were conducted with open-ended questions to foster discussion (Table 1).
DATA ANALYSIS
Quantitative survey data were evaluated using descriptive statistics and chi-squared analysis. Qualitative data from transcribed interviews were reviewed by both authors independently for thematic analysis. 20 Each author independently reviewed the transcripts, identifying specific utterances and developing themes. Themes were progressively developed throughout the course of analysis.
After independent review of the transcripts, the authors subsequently met to compare and reconcile themes. Themes were iteratively amended to account for any new trends identified. Inconsistencies between authors were resolved through discussion and consensus.
Results
Surveys were received from a total of 138 of 348 eligible patients (Table 2). Of the patients surveyed, 27% reported having had a telehealth visit and over half of those indicated that they had completed two or more telehealth visits. Sixty percent of patients reported that they preferred on-site visits. Patients who have had a telehealth visit were significantly more likely (p = 0.03) to indicate that they preferred telehealth.
Patient Survey Demographics
People reported the top benefits of telehealth visits to be no travel (77.9% of respondents), convenience (75% of respondents), and less time off work (39.4% of respondents). Top barriers to considering a telehealth visit included a preference for face-to-face visits (73.7% of respondents), quality of care (36.4% of respondents), and lack of training (15.2% of respondents), as shown in Table 3.
Patient Survey Results
A total of 15 semistructured phone interviews were conducted, transcribed, and analyzed. Identified themes and the corresponding utterances are listed in Table 4. Themes that were most frequently identified included scope of care, convenience, technology, physical examination, therapeutic relationship, patient preference, cost of care, access, and modality.
Identified Themes
The themes of scope of care, convenience, and technology were further divided into subthemes. Scope of care was divided into mental health, results, and unspecified. Convenience was broken down into time, location, comfort, work, and unspecified. Technology was divided into themes of effectiveness, tools, training, and comfort.
Discussion
Themes surrounding the scope of care, convenience, and technology were the most common among rural patients' perspectives. Scope of care specifically included discussion regarding the appropriateness of using telehealth for mental health and follow-up visits. While there was a consensus that telehealth visits were suitable for reviewing previous test results, opinions diverged when it came to mental health appointments.
Some patients felt safer and more comfortable discussing sensitive topics from the security of their own homes, while others believed that technological barriers hindered the development of essential therapeutic relationships required for such discussions. This divergence is particularly noteworthy given that rural populations historically engage less frequently in psychotherapy compared with their urban counterparts. In fact, over half of the U.S. counties are without a local psychiatrist. 4
Although previous research suggests that integrating mental health care into primary care through virtual means can positively influence rural patient perspectives, many respondents emphasized that in-person visits fostered stronger therapeutic connections with their clinicians compared with virtual interactions. 21 Further investigation into therapeutic relationships between rural patients and their clinicians may be warranted.
Overall, there was a consensus that telehealth was best suited for lower acuity visits. Participants expressed concerns that the absence of a physical examination compromised the quality of care they received. Vital signs such as blood pressure and physical examination maneuvers such as lung auscultation were highly regarded for diagnostic purposes. While the potential use of remote patient monitoring devices could address this issue, there remained a discrepancy between patient perception of the value of a physical examination and its true diagnostic contribution in various types of visits.
Cost was a factor mentioned in the interviews. Telehealth visits tend to be less expensive for health systems than in-person visits due to reduced staffing and infrastructure needs, which is appealing in value-based care environments. 22 One study estimated that patients saved up to $126 in missed opportunity costs per telehealth appointment. 23 Despite this fact, current billing systems typically do not distinguish the patient-facing cost between on-site and telehealth visits, leading patients to feel that they were receiving lower quality care at equivalent cost.
With the increase in telehealth use due to the COVID-19 pandemic, these visits are becoming a commonplace option in health care delivery. Although the rates of telehealth visits have declined from early pandemic highs, they continue to be an important part of the ecosystem of care. Patients indicate that access to care, especially specialty care, has improved with telehealth. 24,25
It is vital to understand both the opportunities and limitations of telehealth from patient and clinician perspectives. To appropriately address these factors, changes in the health care delivery system are needed. For example, there needs to be a concerted effort from both private and public entities to increase access to sufficient technology for all populations, regardless of geography and socioeconomic status.
In low-resource areas, telehealth kiosks built into clinics or public spaces such as libraries could be a plausible approach to improving access. Continued efforts to increase broadband access are essential to support patient preference for telehealth offered in the home when compared with a clinic or other sites. 24 Patients in rural areas may be less frequently exposed to newer technologies, so in these scenarios, clear instructions and even staff assistance with navigating the telehealth connection may be needed to improve comfort and increase adoption.
Additionally, when addressing the debate about the quality of audio-only care, it is important to consider the needs of rural populations who may be most familiar with and have most consistent access to a telephone. Finally, there may be different opportunities for the provision of primary and specialty care, with the latter perhaps benefitting more from telehealth options in rural communities due to relative rarity and increased travel time needed for access to some specialties.
Unfortunately, the unique relationship-driven nature of primary care may not lend itself well toward telehealth visits in rural communities given the perceived issues with developing therapeutic relationships over telehealth.
LIMITATIONS
While informative, this study has some limitations. The patients interviewed were from one clinic in a Midwestern county, which may limit the generalizability of the findings. In addition, this county is rated as RUCA code 4.0 in rurality and may not be directly comparable with areas with greater rurality. The absence of demographic data for the patients participating in interviews presents another limitation as it may lower the generalizability of these findings as diverse rural populations exist with varying needs and expectations.
This clinic is also part of a large, academic health system, which may further differentiate it from other rural health care environments. Although this study's sample size is relatively small, including only 15 interviews, we achieved saturation, as evidenced by the absence of new emergent themes in the analysis process.
Finally, only one of the interviews was sourced from a patient who was receiving a telehealth visit, which could bias the responses; however, a large proportion of the sample had previous experience with telehealth visits.
Conclusions
Rural patients have different needs and considerations for utilization of telehealth. Understanding these unique needs is critical to development of approaches that support telehealth utilization and recognize these differences. Telehealth options can truly benefit rural populations by providing convenient, timely, and comfortable patient care if they are implemented in a way that respects the unique context and perspectives of these populations.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This was an unfunded study with minimal resource support provided by the University of Wisconsin Department of Family Medicine and Community Health.