
Abstract
Objective:
The SARS-CoV-2 pandemic and related lockdown periods generated an increase in the use of virtual care for mental health (MH). This study aimed to assess patient satisfaction with Telemental Health services (TMH) during first lockdown and factors related to their willingness to continue using this service.
Methods:
We conducted a cross-sectional survey of 364 MH outpatients from 9 centers in the Barcelona region (Spain), who received TMH between April 20 and May 22, 2020. We assessed sociodemographic and clinical characteristics, prior experience, and familiarity with technologies and satisfaction with TMH. Willingness to receive TMH after the lockdown was measured separately for telephone and videoconferencing. We performed descriptive statistics and bivariate and multivariate regression models to predict TMH willingness.
Results:
From 450 patients contacted, 364 were interviewed. Satisfaction with TMH was high (mean 9.24, standard deviation 0.07); 2.47% preferred only TMH visits after lockdown, 23.08% preferred mostly TMH visits, 50.82% accepted some TMH visits, and 23.63% would prefer in-person consultations. Female patients and those having received TMH during lockdown showed higher odds of willingness to receive TMH in the future, while patients unfamiliar with technologies showed lower odds. Concerning TMH through telephone, willingness was more likely in patients living with more persons. Videoconferencing willingness was more likely for people living with depression.
Conclusions:
TMH was well accepted during the first lockdown and patients were willing to maintain it after lockdown. Low familiarity with new technologies is an important barrier to TMH willingness, which needs to be addressed for appropriate implementation going forward.
Introduction
The SARS-CoV-2 pandemic represented a global and unprecedented challenge that tested national health systems. 1 –3 Telemental Health (TMH) was one of the measures implemented to continue delivering mental health (MH) services during lockdown periods. This represented a unique opportunity to test the deployment of TMH in a setting where it was weakly implemented before the pandemic, despite evidence indicating it was comparable with in-person visits in terms of assessment outcomes, cost-effectiveness, and patients' satisfaction. 4 –7
Since the challenges of early response to the SARS-CoV-2 pandemic gave way to a continuous adaptation to the long-run changes and effects of the virus on population health and social dynamics, in this context, research conducted at the start of the pandemic on the emergency implementation of TMH offers valuable insight into how it could contribute to pandemic preparedness and its role in improving efficiency and reach of services in routine care. In Catalonia, Spain, and Europe more broadly, some issues have been raised about inequities in access to specialized MH services in rural or remote areas. Telemedicine could be a solution if well accepted by professionals and patients.
Patients' satisfaction with TMH and willingness to receive MH services through this technological mode of delivery are essential for implementing TMH, in both emergency response and in routine practice. Evidence shows that during the pandemic, TMH patient satisfaction was high 8 –10 and comparable 11,12 with prepandemic outcomes, for programs previously delivered in-person and converted to TMH, 13 and for TMH-delivered programs. 14 There is an increasing body of evidence on patients' willingness to continue TMH after the pandemic. In previous studies, 25–50% of patients reported they had attended consultations at least partially through TMH, 15,16 and patients' willingness to maintain TMH attention was found to be unrelated to patients' sociodemographic and clinical characteristics. 12,16 To implement TMH adequately in the future, it is essential to understand whether health care users would be willing to maintain TMH and who would benefit most from this means of health care delivery.
In Catalonia, Spain, the first and subsequent lockdowns posed outstanding organizational challenges for health care providers due to social distancing measures. This study aimed to understand patients' satisfaction with TMH during the early pandemic lockdown measures in Catalonia, as well as their willingness to maintain TMH after pandemic, and sociodemographic and associated clinical factors. This knowledge would provide insight into whether health service users are open to wider implementation of TMH, and which user groups might benefit most from this mode of delivery.
Methods
STUDY DESIGN, SETTING, AND PARTICIPANTS
A cross-sectional study was conducted at Parc Sanitari San Joan de Déu (PSSJD), a health care organization that provides mental and physical health services to 1.5M people in the southern area of the Barcelona region (Catalonia, Spain). Ambulatory care is provided in nine mental health centers (MHC) in the area affiliated with PSSJD, most of them located near to Primary Care (PC) services. These MHC provide treatment for severe mental disorders or other disorders that are resistant to PC treatments. Every MHC has a team of psychiatrists, psychologists, nurses, social workers, and administrative staff. Ambulatory care also includes Community Mental Health Rehabilitation Services, linked to MHC, provided by staff trained in social education, social work, and psychology.
The World Health Organization (WHO) officially declared the SARS-CoV-2 pandemic on March 11, 2020. In Spain, the first confirmed case was on January 31 and a complete lockdown for the entire population was implemented on March 14, with 5,753 infections and an incidence of 123 cases per 100,000 inhabitants. Only essential workers were allowed to leave their homes to work. The general population was allowed to leave their homes only exceptionally (e.g., to buy food and essential items or to attend to people in need of care). The first lockdown was initially planned for 2 weeks, but ultimately lasted until June 21.
Adult patients (≥18 years old) diagnosed with any mental disorder and being treated through TMH at one of the nine MHC at PSSJD during the first lockdown were interviewed by administrative staff at the PSSJD's Customer Service by telephone between April 20 and May 22, 2020. We consecutively selected, from the appointment schedule of all nine MHC, 50 patients who had consulted within the week before the start of the study. In case of nonresponse to a first telephone contact, no replacement was done. We followed Strengthening the Reporting of Observational studies in Epidemiology (STROBE) checklist for reporting observational studies. The study was approved by the Ethics Board of Sant Joan de Déu Research Institute (C.I. PIC-105-20).
VARIABLES
Patients were asked about sociodemographic and clinical characteristics (gender, age, education years, number of persons in household, time since diagnosis, and diagnosis), access to new technologies (access to mobile phone, tablet, and laptop or desktop computer with or without internet connection), familiarity with new technologies on a 4-point scale with verbal anchors, from very unfamiliar to very familiar, and use of TMH care services during lockdown (phone calls, videoconference, and WhatsApp).
Participants who had received TMH during lockdown rated their global satisfaction with TMH on a 10-point scale. They also rated their satisfaction in relation to each staff group (psychiatrists, psychologists, nurses, social workers, and social educators) by rating the service received on 7-point scales (with extreme values labeled as very bad to very well). After that, they were asked to rate their satisfaction of services received in comparison with before lockdown, if applicable and if care received, on a 5-point scale with verbal anchors (much worse, worse, equal, better, or much better).They also rated the services received on numeric 10-point scales by type of actions (listening, counseling, follow-up, and answering patient queries) and type of activities (physical, cultural, artistic, and play).
Participants were asked for their opinion about TMH implementation beyond lockdown first as a general question (“When the lockdown will end, would you be willing to a) only do consultation using telehealth, b) do most consultations using telehealth, c) do some visits using telehealth, or d) go back to only do consultations in person?”). This question was scored on 4-point scale from 0 (only in person) to 3 (only telehealth). Willingness to receive TMH was subsequently measured in relation to each staff group mentioned above (7-point scales from impossible to very possible), type of visits (requesting clinical reports, urgent situations, renewal of electronic prescriptions, and other), and way of delivery (e-mail, WhatsApp, “La meva salut” i.e., a regional shared electronic patient records platform, and other). The survey was designed specifically for this study (Supplementary Data).
STATISTICAL ANALYSES
Descriptive analyses were conducted to characterize the study sample and the main outcome variables: satisfaction with TMH during lockdown and willingness to receive TMH after lockdown. These analyses included proportions and frequencies for categorical variables, and mean and standard deviation (SD) or median and interquartile range (IQR) for continuous variables, depending on distribution characteristics. Bivariate ordered logistic regression models were fitted to examine the factors related to willingness to receive TMH (general question, and separately through phone and videoconference) after lockdown. Those variables that predicted the outcome in the bivariate analysis (p < 0.20) 17 were introduced into multivariate ordered logistic regression models. Odds ratios (ORs) and 95% confidence intervals (CIs) were reported in each model. We used an alpha level of 0.05 for all statistical tests. All analyses were performed using Stata version 13 for Windows 18 (SE version 13, College Station, TX).
Results
Sociodemographic and clinical characteristics are described in Table 1. Figures 2 and 3 show satisfaction with TMH per staff group, during lockdown and compared with prelockdown. Table 2 shows results regarding TMH willingness postlockdown, whereas Table 3 shows factors related to global telematic, phone call, and videoconference assistance predispositions after lockdown.
Sociodemographic and Clinical Characteristics (n = 364)
SD, standard deviation; TMH, Telemental health services.
Willingness to Receive Telemental Health After Lockdown (n = 364)
Willingness to Receive Telemental Health After Lockdown per Type of Technology (n = 364)
IQR, interquartile range.
SAMPLE CHARACTERISTICS
From the 450 patients initially contacted, 364 patients were interviewed, representing between 38 and 43 patients per center. Participants had average age of 47.8 years (SD 14.52), and an average of 10.39 years of education (SD 3.16); 197 (54.12%) were women, and 269 (73.90%) lived with at least another person. The average time since diagnosis was 9.45 years (SD 8.66). Regarding the main diagnoses, 99 (27.19%) participants suffered from depression and 92 (25.27%) suffered from depression and anxiety; 67 (18.40%) were diagnosed of psychosis and 7 (1.92%) with psychosis and other comorbidities; and 34 (9.34%) suffered from bipolar disorder, 49 (13.46%) had anxiety, and 6 (1.65%) had personality disorder.
Concerning access to new technologies, 299 (82.14%) participants had a device with internet connection (mobile, laptop, tablet, or personal computer) and 66 (18.13%) had no device or only a mobile phone without internet connection. Most had used WhatsApp chat (276, 75.82%) and 229 (62.91%) had used WhatsApp videoconference before the pandemic. In contrast, 74 (20.33%) had previous experience with Skype, and 76 (20.88%) with other videoconference software. Regarding familiarity with technology, 253 (69.51%) of the patients reported to be at ease or very much at ease with new technologies.
Most participants (88.46%) reported having received TMH during lockdown, 11.26% reported not having received any TMH, and 0.27% reported an in-person visit at the MHC. From those who received TMH during lockdown, at least 87.64% received it by phone, 2.75% by videoconference, and 0.55% by WhatsApp chat (Table 1).
SATISFACTION WITH TMH PROVISION DURING LOCKDOWN
Participants who declared receiving TMH during the lockdown rated global satisfaction on average 9.24 (SD = 1.22) on a 1–10 scale (median [IQR] = 10 [1]). Figures 1 and 2 show satisfaction ratings per staff group during lockdown and compared to prelockdown, respectively. Figure 3 shows satisfaction ratings during lockdown by actions and activities.
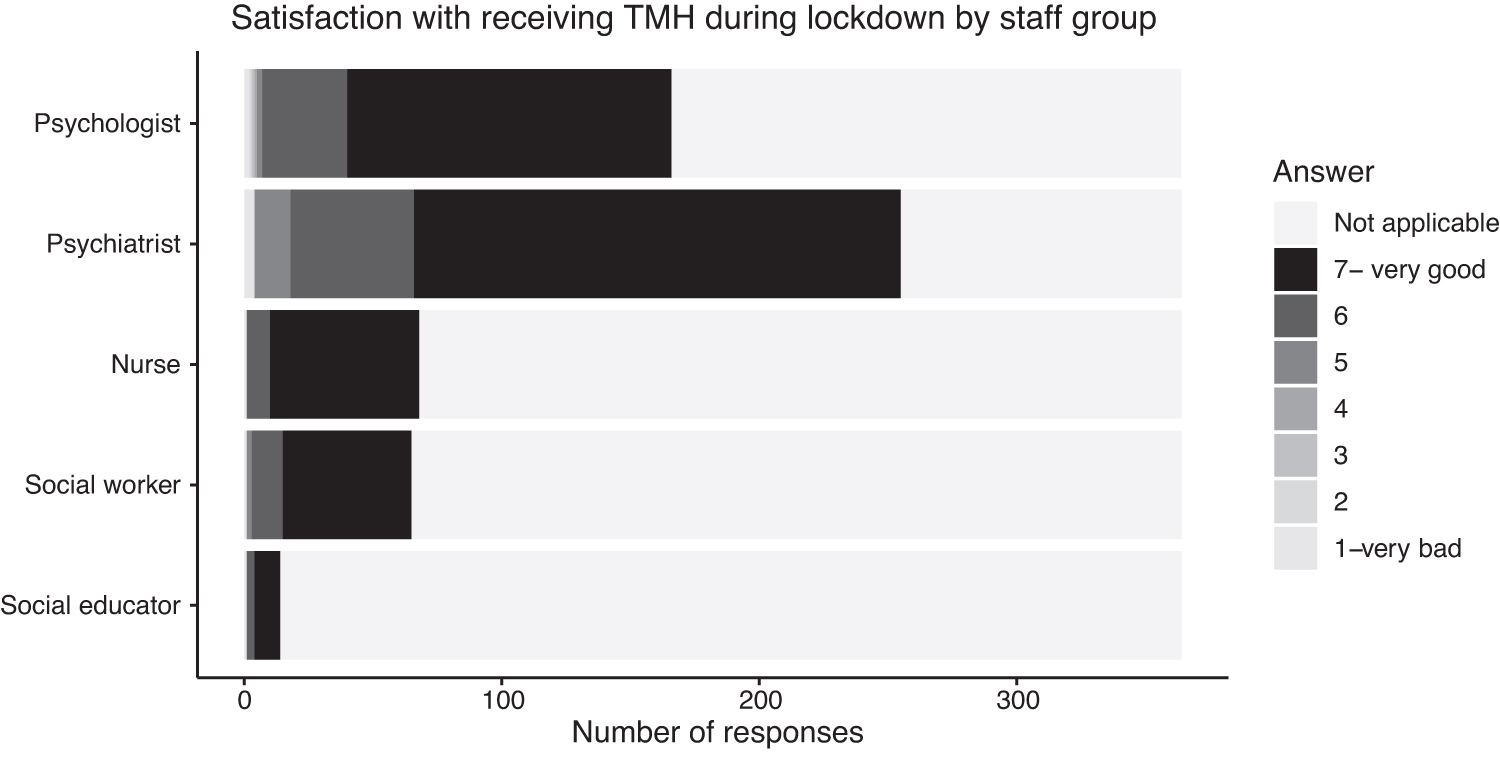
Satisfaction with receiving TMH during lockdown by staff group. TMH, Telemental Health.
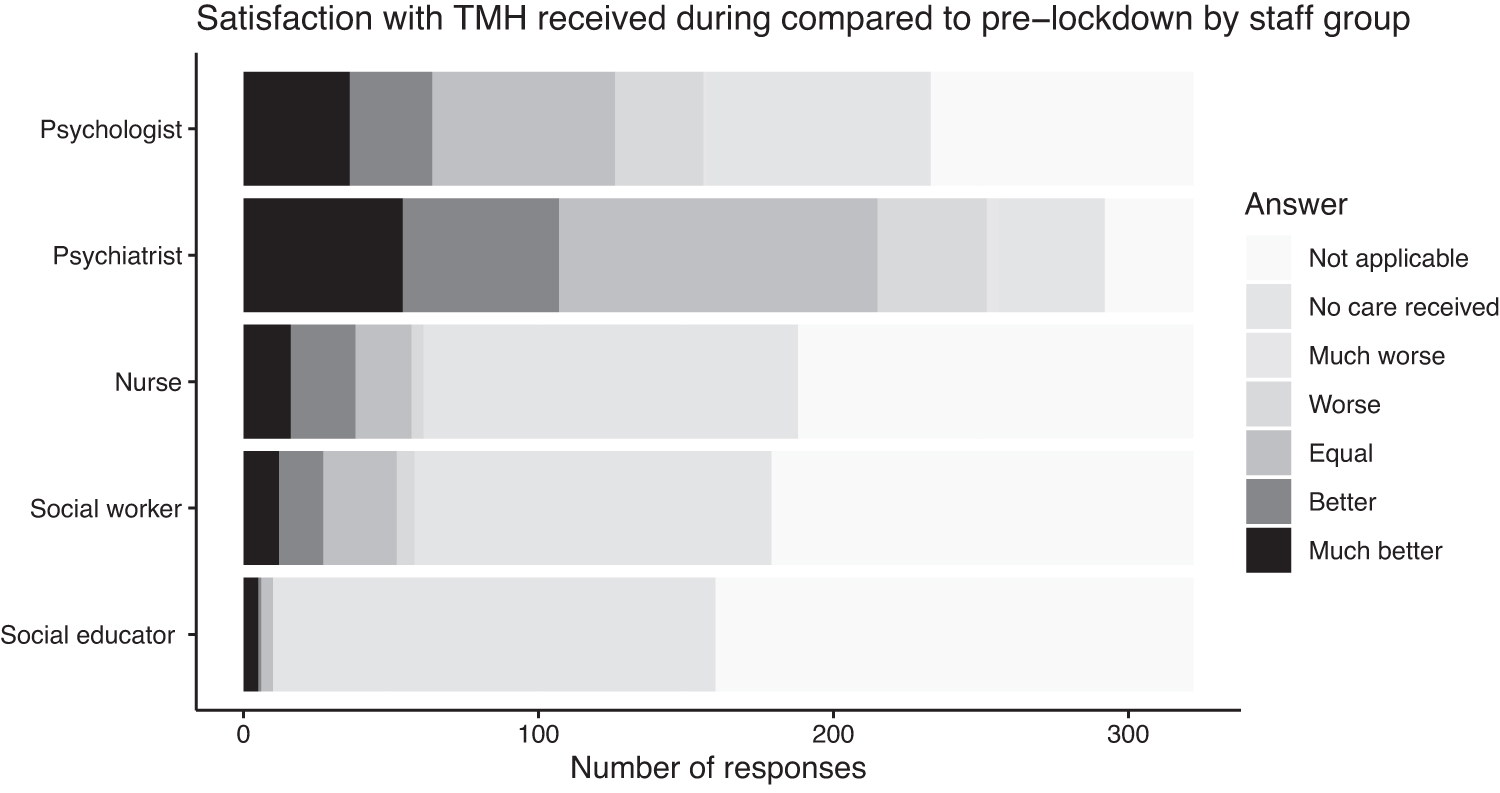
Satisfaction with TMH received during lockdown compared to prelockdown by staff group.

Satisfaction with TMH received during lockdown by actions and activities.
WILLINGNESS TO CONTINUE TMH AFTER LOCKDOWN
Regarding TMH after lockdown, 2.47% of participants stated they preferred only TMH visits, 23.08% stated that they would agree to receive most of their visits through TMH, 50.82% that they would agree doing some TMH visits, and 23.63% that they would rely only on in-person consultations. Participants reported they were willing to continue receiving TMH after lockdown through phone call and videoconference with an average of 5.80 and 4.71, respectively, on a 1–10 scale. Patients were willing to use TMH care for asking for medical reports (77.75) and reissuing electronic prescriptions (73.36%). For those situations, they preferred to use WhatsApp chat (53.85%), e-mail (36.54%), a web-based official platform called “La meva salut” (9.34%), or others not specified (25.55%) (Table 2).
Regarding the type of visits they would accept by TMH through phone calls, 312 (85.71%) participants expressed preference for maintaining this mode of delivery for answering queries about medication, 251 (68.95%) for urgent situations, 109 (29.94%) for follow-up visits, and 3 (0.82%) for a first visit. Concerning videoconference assistance after lockdown, 177 (48.63%) participants were willing to do so to answer queries about medication, 72 (19.78%) to receive emergency care, 44 (12.09%) for follow-up visits, and none for being attended as first visit (Table 3).
FACTORS RELATED TO WILLINGNESS TO RECEIVE TMH AFTER LOCKDOWN
Willingness to receive TMH after lockdown in general (4-point scale)
Female patients and those having received TMH during lockdown showed higher odds of willingness to receive TMH after lockdown compared to male patients (OR = 1.54 [95% CI = 1.00–2.52]). Patients who had received TMH care during lockdown showed higher odds of willingness to receive TMH after lockdown compared to those who had not (OR = 2.69 [95% CI = 1.39–5.18]). Patients very unfamiliar with technologies showed lower odds of TMH willingness compared to those with high familiarity (OR = 0.30 [95% CI = 0.12–0.79]) (Table 4).
Ordinal Regression Models of Factors Associated to the Willingness to Receive TMHC After Lockdown in General, Phone Call or Videoconference
p < .05; ** p < .01; *** p < .001.
CI, confidence interval; OR, odds ratio.
Willingness to receive TMH after lockdown by phone call or videoconference
Concerning TMH through telephone, willingness odds were higher in patients living with one, or three or more persons, compared to those living alone (OR = 2.16 [95% CI = 1.30–3.59] and OR = 1.95 [95% CI = 1.09–3.50]), and in those having received TMH care during lockdown compared to no TMH care (OR = 2.35 [95% CI = 1.31–4.23]), and lower in those feeling unfamiliar with technologies compared to those reporting high familiarity (OR = 0.49 [95% CI = 0.31–0.80]) (Table 4).
For videoconferencing, odds of TMH willingness were lower in patients feeling unfamiliar with technologies (OR = 0.24 [95% CI = 0.14–0.41]) and very unfamiliar with technologies (OR = 0.05 [95% CI = 0.01–0.23]), compared to those reporting high familiarity, and higher in patients with depression diagnosis compared to psychosis (OR = 2.23 [95% CI = 1.18–4.22]) (Table 4).
Discussion
High levels of satisfaction with TMH during lockdown were found in patients receiving MH services in Catalonia, Spain, in the early phase of the SARS-CoV2 pandemic. Moreover, we found high willingness to continue with TMH after lockdown measures were relaxed. This suggests that health service users were ready for upscaling implementation of TMH in emergency care, as well as routine care, and thus our findings are supportive of TMH as a mode of health care delivery. This study highlighted important facilitators and barriers, for example, having received TMH previously or unfamiliarity with technology.
The findings highlight the importance of supporting patients in their initial contact with TMH, especially for dealing with technical aspects, and also tailoring the mode of delivery (remotely versus in-person) based on patients' familiarity with technology. Our findings point to specific user groups likely to be most open to TMH (women, people in larger households, and people living with depression). This suggests that health care providers could prioritize TMH services for these groups of patients.
The high levels of TMH satisfaction during lockdown found in our Catalan population are consistent with previous studies. In a survey during the first pandemic wave in New York City, 11 participants declared high TMH satisfaction, and most of them considered both phone calls and videocalls as equally good compared to in-person visits. In a cross-sectional cohort survey in an Adult Transition Program, also during lockdown in the United States, 13 the majority of patients reported high satisfaction with the TMH format and most patients declared they would recommend this service format to a friend or family member.
In patients receiving care in an outpatient setting in Macedonia, 8 also during the early phase of the SARS-CoV-2 pandemic, TMH received high scores on accessibility and convenience by most patients, irrespective of gender, age, or place of living. Similarly, the vast majority of patients in King Khalid University Hospital of Riyadh reported a sense of overall satisfaction with TMH services. 10 Our study confirms findings from different geographical areas and populations and suggests that TMH can be, should a new emergency occur, used with confidence that service users would be globally satisfied. Moreover, the comparison with prelockdown shows that special consideration should be given to maintaining quality of care.
In the urban environment of the survey conducted in Riyadh, over half of the patients agreed or strongly agreed to use TMH after pandemic. 10 Similar results were shown in both mentioned surveys in an outpatient clinic in Ann Arbor, Michigan, where a pilot TMH program was tried without success in September 201919 and in the United States Adult Transition program. 13 Our study found high levels of willingness to maintain TMH after lockdown in patients living in Catalonia, which surpass levels found in other comparable settings in terms of urban population, age, access to technology, and health care system technological level.
Participants preferred the use of TMH after the pandemic in queries about medication, reissuing electronic prescriptions and emergency care. We may argue that noticing some new symptom or perceived adverse effect and being aware of electronic prescriptions that expire soon are situations of relative urgency that patients are keen to solve promptly. As far as we know, no study explored in more detail patients' perceptions of the type of situations qualifying as emergency care from their perspective, opening a key question to explore in future studies, which may help implement TMH appropriately.
In our study, feeling uncomfortable with technology was a strong barrier to accepting TMH. This finding is consistent with the association reported in a meta-analysis of 29 studies 7 between high satisfaction with TMH and minimization of technology-related concerns, and the need of technical support reported in a sample of young adults with a first episode of psychosis in Canada. 20 This result points to a technological gap in our sample that might be solved with previous training of eligible patients to implement TMH adequately. Our participants were more predisposed to continue with consultations through phone calls than through videoconference, likely because most of our sample had received phone calls and became more familiar with this way of TMH delivery, and due to the higher technical complexity of videoconferencing, consistent with the sense of technological gap identified in our sample.
Our findings regarding the higher willingness to continue TMH characterizing women, people who live in larger households, and depressed patients bring new information to the evidence base on this topic. Previous studies 11,16,19 found no notable difference in the willingness to continue TMH in terms of age, gender, diagnoses, number of previous visits, and TMH satisfaction and willingness to maintain TMH after the pandemic.
In a cross-sectional survey of an adult population in Arkansas, 21 participants with anxiety and depression used notably more TMH during pandemic, but the study did not specify if this was a factor that contributed to increased willingness to continue with TMH. We may argue that, due to intrinsic characteristics, depressed patients would appreciate meeting in-person with a therapist more than patients suffering from other pathologies. Growing evidence of positive effects in symptoms and quality of life of TMH in depression 22 opens the door to consider implementing this mode of delivery with depressed patients.
These results shed light on how TMH could be implemented adequately. Since patients were satisfied with TMH and mostly agreed to maintain it, future studies might explore the conditions of effective TMH implementation in terms of TMH acceptance and willingness to maintain it. Of particular relevance is the role of TMH preferences regarding queries about medication, reissuing electronic prescriptions and attending urgent situations, and differences depending on gender, living status, and diagnosis. Future studies may also explore other patient characteristics and preferences to outline concrete profiles of patients who could benefit most of TMH.
Some limitations should be considered when interpreting the results of this study. First, the sample was selected by convenience and therefore might not be representative of the population of Catalonia. Moreover, 11.54% of the respondents said that they did not attend consultations remotely during the lockdown. The reasons why some respondents did not recognize having received TMH services were not explored. We may argue that memory bias due to the difficult situation could play a role. The generalizability of results reported might be limited by the fact that the questions were specifically designed for this study and most data regarding TMH services referred to phone calls, with limited data collected about videoconferencing.
Conclusions
The results from our study show that TMH is well accepted by patients and might have an important role in global MH care complementing in-person care, especially in women, patients who are living with relatives, and depressed patients in relatively urgent situations. Characterizing patients' profiles and preferences and overcoming barriers such as the technological gap by training patients before TMH would be of capital importance to optimize its implementation.
Significant Outcomes
TMH is well-accepted by patients to maintain MH care in lockdown situations.
TMH is well-received by patients beyond lockdown periods.
Low familiarity with new technologies is an important barrier to willingness to receive TMH.
Female patients, those who have received previous TMH, those who live with another person/s in the household, and depressed patients may benefit the most from TMH.
Limitations
Our results reflect the TMH experiences of a selected patient sample in a specific geographical area and unique circumstances and thus need to be corroborated with other studies.
The use of study-specific measures, although appropriate given the context, limits comparison with other research.
Footnotes
Acknowledgments
The authors would like to thank the patient management staff for their collaboration asking survey's questions.
Authors' Contributions
V.C.: Conceptualization, methodology, supervision, writing—original draft, and writing—review and editing. M.R.-V.: Conceptualization, methodology, supervision, and writing—review and editing. J.D.A.: Methodology, data curation, formal analysis, supervision, and writing—review and editing. L.B.H.: Supervision and writing—review and editing. I.M.: Conceptualization, investigation, and methodology. J.A.T.: Supervision, methodology, and writing—review and editing. J.A.C.: Supervision and writing—review and editing. C.P.-S.: Supervision and writing—review and editing. A.L.D.: Conceptualization, investigation, methodology, data curation, formal analysis, supervision, writing—original draft, and writing—review and editing. A.S.-B.: Conceptualization, investigation, methodology, data curation, formal analysis, supervision, and writing—review and editing.
Disclosure Statement
The authors have no conflict of interest to declare.
Funding Information
A.L.D. was supported by a Miguel Servet Fellowship (No. CP21/00062) during part of this study.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.