
Abstract
Introduction:
Structured and standardized follow-up care for preterm and high-risk infants enables an early detection of developmental deficits. The aim is to adapt the in-person follow-up to video consultation. Developmental delays can thus be identified at an early stage, independently of in-person contact.
Methods:
The adaptation of these follow-up to video consultation is presented descriptively, compared with the in-person consultation (similarities, differences, challenges, and limitations). Professionals's experiences with the adaption are described.
Results:
The experience of n = 267 video consultations for follow-up of children up to 6 years shows that an adaptation of the in-person consultation is necessary and possible. Prerequisite is a digital medium with a stable internet connection on both sides: the professional and the family, as well as a portal for video consultations with certified, encrypted data transmission. Among infants, testing is almost entirely parent guided. For older children, testing procedures have been adapted. A neurological examination is largely possible, while a general pediatric examination is omitted. A survey on professionals' (n = 7) experiences with video- and in-person consultations found that the rate of complete follow-up visits and the resources required for taking medical histories, personnel, and time remained constant for both approaches. All reported that the video consultation is generally suitable for identifying developmental delays in children up to an age of 6 years comparable with in-person consultations. One professional stated that the physical examination of children aged ≥1 year is impossible.
Discussion:
Video consultation is an alternative despite some limitations when an in-person consultation is impossible. Developmental delays can be identified, and therapies recommended.
Introduction
Worldwide, 3.4 million babies were born preterm in 2020, which is equivalent to >1 in 10 infants. 1 In Germany, every eleventh child (8%) was born too early in 2020. 2 Preterm infants, thus, represent the largest pediatric patient group. 3 The risk of severe neurological complications (e.g., intraventricular hemorrhage, periventricular leukomalacia) has decreased in preterm infants over the past 20 years. 4,5 However, the prevalence of mild impairments such as developmental delays, mild motor and/or cognitive impairment as well as behavioral difficulties remains constant. 6 Even in the absence of severe neurological complications detectable by imaging, child development can be impaired by preterm birth. 7 Structured and standardized follow-up care enables an early identification of developmental delays. Appropriate early support or therapy can thus be initiated. 8
The COVID-19 pandemic posed challenges to the health care system that affected not only inpatient treatments but also outpatient care, including electively scheduled appointments. Digital patient care has significantly advanced under the new requirements. The benefits independent of a pandemic situation have been demonstrated. 9,10 The question is whether it is possible to adapt neurodevelopmental neurological follow-up visits to video consultation.
In Germany, the (Model) Professional Code of Conduct for Physicians (Musterberufsordnung für Ärzte) did not allow exclusive treatment by means of video- or telemedicine in Section 7(4) until 2018. Physicians are not allowed to offer individual medical treatment, exclusively through print and communication media. 11 Now, an exclusive consultation or treatment through communication media is permitted in individual cases.
The consultation must be medically justifiable, and the necessary medical care must be maintained, particularly through the manner of diagnosis, consultation, treatment, and documentation. The patient must be informed about the specifics of exclusive consultation and treatment through communication media. 12 The new regulation has now been implemented by the medical associations.
Regardless of the COVID-19 pandemic, national and international medical professional groups and associations increasingly view telemedicine as a potential valuable medium in patient care. 13 Because of infection control for patients and medical staff video- and telemedicine is an alternative. Parents of preterm and high-risk newborns with a potentially weakened immune system and reduced lung function were more likely to have avoided contact with others and therefore, benefitted from a video consultation. 14 In addition, telemedicine appears to be useful for patients who live far from the follow-up site, or who have significant time and effort requirements due to complex care needs (e.g., home noninvasive/mechanical ventilation).
There are a very few studies reporting telemedicine after discharge from the neonatal intensive care unit. 15 –17 Parents report feeling confident in dealing with their own child. 15 They view telemedicine as a good supplement but not as a complete substitute for in-person care. 18 DeMauro et al. dealt with a follow-up care program in Philadelphia, the United States. 19 In Germany, there is a lack of adaption of follow-up visits for video consultation.
Structured follow-up programs are required at least up to an age of 6 years for children born preterm and at risk to detect developmental delays or impairments as early as possible to initiate interventions. 8,20 Therefore, the aim is to present an adaptation of a follow-up program for video consultation and to determine differences to the in-person visits. Furthermore a survey evaluates the professionals' view on video consultation.
Methods
Since March 2020, 267 children participated in video consultations for developmental neurological follow-up visits for preterm born and high-risk infants at the University Hospital Essen, Germany. The platform used was www.Sprechstunde.Online.de (Zava Sprechstunde Online GmbH, Essen, Germany) with end-to-end encryption.
To conduct the video consultation, practitioners utilized a computer/laptop, a webcam, a microphone, and a loudspeaker, while patients employed laptops, smartphones, or tablets with an integrated camera. They participated in a peer-to-peer connection, enabling a direct data exchange between the devices used, rather than through a central server. Health care professionals worked from clinic or home office, while the families attended the appointments from their homes. To ensure the highest quality, Zava Sprechstunde Online GmbH automatically adjusts the bandwidth.
A high-quality session involving two participants or devices requires a bandwidth of 600 kilobits per second (Kbps) (upload/download). Optimal performance can be achieved with a bandwidth of 800 Kbps or 1.0 megabits per second (upload/download) when using three or more subscribers or devices. 21
The patient population included the following: Preterm infants ≤35 + 0 GA or <1,500 g birth weight, Preterm infants <37 + 0 GA with birth weight <3rd percentile, Neonates after perinatal asphyxia with/without hypothermia treatment, and Neonates with potentially neurological sequelae (e.g., neonatal abstinence syndrome, hypoglycemia <25 mg/dL, meningitis, cerebral hemorrhage).
Parents were offered video consultation visits under the following circumstances:
Willingness/explicit wish of the parents to participate in video consultation,
Infection/quarantine of the child or parents (no in-person consultation possible due to infection protection reasons),
Families residing far from care site,
Dependence on medical equipment (respiratory support, dialysis),
No language barrier (communication in German/English),
Technical requirements (internet connection, digital medium) were met
Assessment of muscle tone/spasticity by palpation by physician/therapist was not mandatory.
The patients undergo a medical examination as well as standardized test procedures from various professional groups (e.g., psychologists, physiotherapists, occupational therapists) for developmental assessment (Table 1). This structured program served as the basis for adapting the follow-up visits for video consultation. A descriptive analysis of the adaption, similarities, differences, and limitations of video consultations compared with in-person consultations was conducted.
Excerpt from the Structured Follow-Up Program in In-Person Consultation at Our Center
BSID III, Bayley Scales of Infant Development Third Edition; FEW-2, Frostigs Entwicklungstest der visuellen Wahrnehmung 2 (German Version of Developmental Test of Visual Perception, Second Edition); GMA, General Movements Assessment; HINE, Hammersmith Infant Neurological Examination; M-ABC 2, Movement Assessment Battery for Children Second Edition; WPPSI-IV, Wechsler Preschool and Primary Scale of Intelligence Fourth Edition.
The experiences of health care professionals with video- and in-person consultations were recorded in a survey and presented descriptively. A statistical comparison between the groups was not planned due to the small number of professionals in this specific area of work and the survey in a single center.
ETHICAL APPROVAL
No ethical approval was required for the description of the adaptation of video consultation. The evaluation of health care professionals with video- and in-person consultations was approved by the local ethics committee (20-9319-BO). The evaluation of family satisfaction with video- and in-person consultation was published by Albayrak et al. 10
Results
REQUIREMENTS AND PREPARATION
Video consultation requires an adaptation of the follow-up program in several points (Fig. 1). No traveling to the outpatient clinic is required for parents and, if applicable, for staff. The same amount of staff and time is necessary for the interdisciplinary consultation (physician and at least one therapist). The prerequisite for a video consultation is a digital medium with a stable internet connection as well as a portal for video consultations with certified, encrypted data transmission. The family is identified at the beginning of the video consultation by means of an identification document.
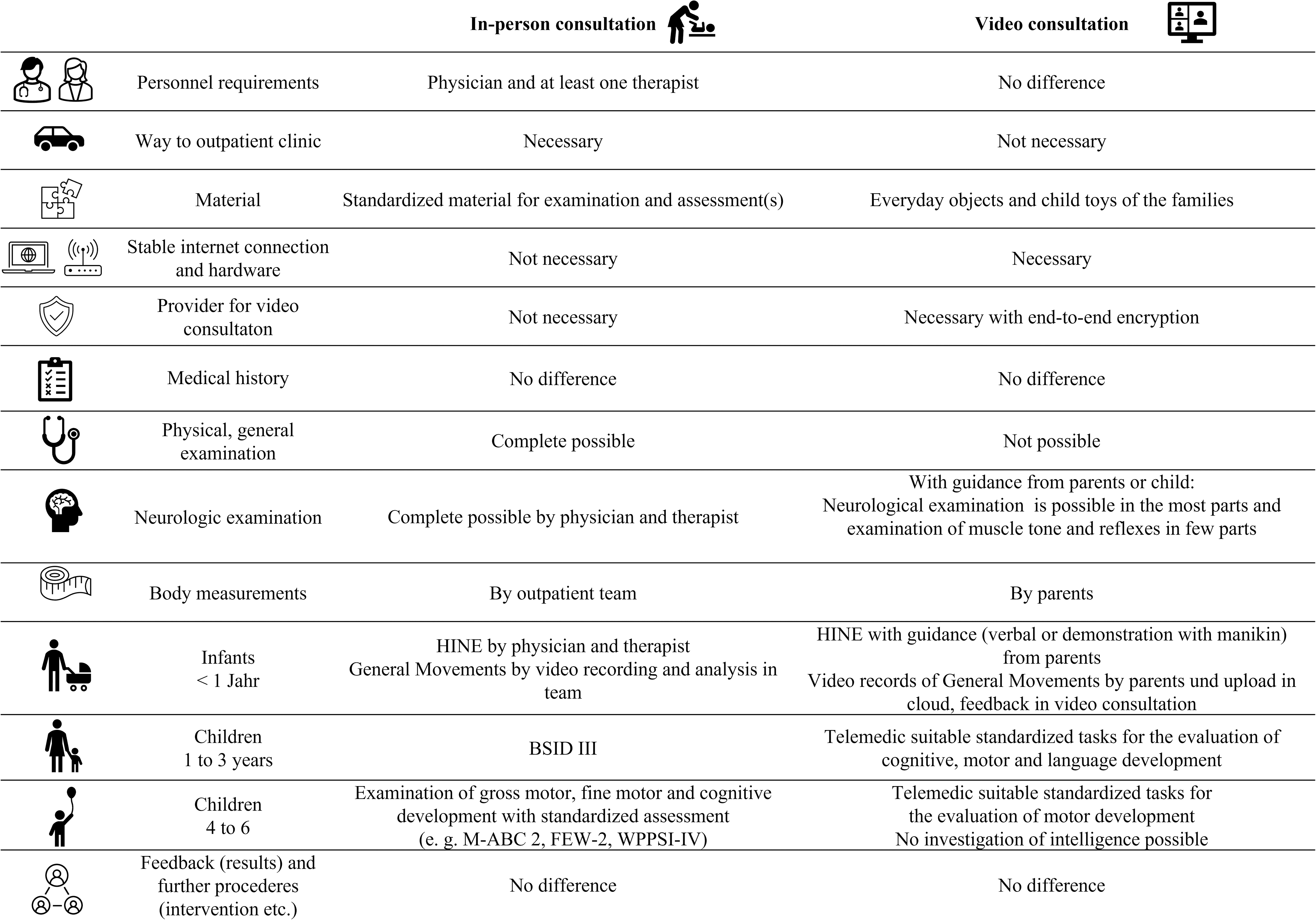
Overview of similarities, differences, and adaptations of an in-person and video consultation in developmental neurological follow-up visits of children born preterm and at high risk. BSID III, Bayley Scales of Infant Development Third Edition; FEW-2, German Version of Developmental Test of Visual Perception 2; M-ABC-2, Movement Assessment Battery for Children Second Edition; WPPSI-IV, Wechsler Preschool and Primary Scale of Intelligence Fourth Edition.
Families were contacted by email before their video consultation (Supplementary Fig. S1). They were provided with print templates (presented in Fig. 2) and a list of specific household items suitable for children (e.g., paper clips, building blocks). This should stimulate certain play activities and tasks of daily life to observe the child's behavior, and to be able to draw conclusions about the development.
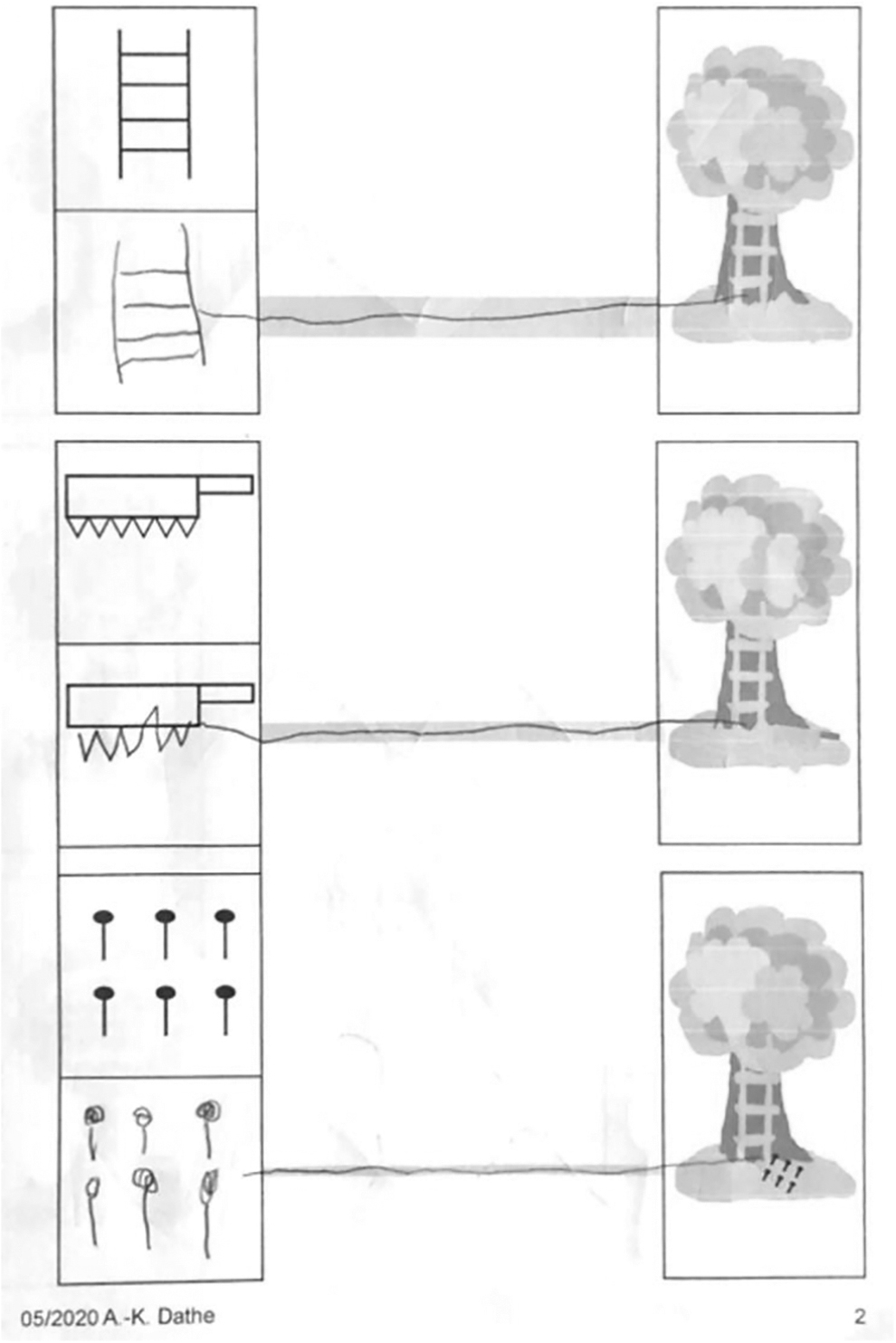
Excerpt from print templates filled in by a 5-year–old preterm child.
MEDICAL HISTORY AND EXAMINATION
During both the in-person and the video consultation, a detailed medical history (pregnancy, birth, family, social, development) is taken. A physical, general pediatric examination is impossible during the video consultation, while metric data (e.g., height, weight, head circumference) can be collected from parents. Much of the neurological examination can be performed under the guidance of the parent or the child. The examination of reflexes and muscle tone is limited.
SCREENING FOR DEVELOPMENTAL DELAYS
The follow-up program is characterized by a standardized testing of developmental or specific skills. These were adapted as screening for video consultation.
At the age of corrected 3 months, a General Movements Assessment (GMA) 22 is performed. Within the in-person consultation a video recording of spontaneous movements of the child is made, while in the video consultation parents upload a self-recorded video through a data protection compliant cloud of the University Hospital. The GMA is performed interdisciplinary, with prompt feedback to the parents.
At the corrected ages of 3 and 6 months, the Hammersmith Infant Neurological Examination (HINE) 23 is performed. This examination was entirely performed by the parents who were provided with instructions and demonstrations of each item with the aid of a manikin. Detailed explanations of the items allowed parents to better understand the physiology of movement development, and they found the procedure pleasant. 10 Only reflexes cannot be examined; hence the total score was adapted to 75 points instead of a maximum of 78.
The Bayley Scales of Infant and Toddler Development Third Edition 24,25 could not be used in video consultation due to the number of materials, instructions, and a lack of validation for telemedicine. To detect developmental delays in cognitive, motor, and language skills among children at the age of 1–3 years, telemedicine suitable tasks were developed by our group. Tables 2 and 3 show an excerpt of tasks and materials for children aged 24 months and possible observations.
Excerpt from the Adapted Tasks for Recording Developmental Delays at the Age of 2 Years
Excerpt from Materials and Possible Observations in Children at the Age of 2 Years
The performance requirement was chosen, so that age-appropriate children would complete all tasks. Thus, it was possible to identify a need for intervention using the adapted tests as a screening of cognitive, motor, and language development. A survey of the development quotient was not conducted, and a comprehensive evaluation of the development status was impossible.
At ages 4–6 years, adapted testing of the children's visual motor skills, visual perception, and fine motor skills was evaluated. 28 The children were instructed to copy a given figure into a box, and then draw a line connecting the box to the tree (Fig. 2). These tasks enable the evaluation of pen handling, drawing precision, wrist dynamics, and finger muscle tone during drawing. Fine motor skills were conducted based on everyday objects, a playful story about building a tree house, Frostig's Developmental Test of Visual Perception, 2,26,27 Developmental Test of Visual-Motor Integration, 27 and the Movement Assessment Battery for Children Second Edition. 29,30
Tasks included drawing/coloring (to assess pencil posture and use of force), cutting, folding, and placing paper clips in a small box. Assessment characteristics included time measurement for a task, observation of precision, and tone regulation. In in-person consultations, an assessment of intelligence (using a Wechsler intelligence test) and concentration ability was also included as part of the behavioral observation, which was impossible during video consultation.
Examination components not shown in the video consultation for various reasons could be videotaped by the parents later and made available to the treatment team through the privacy-compliant cloud.
FEEDBACK AND FURTHER PROCEDURE
The consultations were always followed by an interdisciplinary discussion of the findings, including possible therapy recommendations. New appointments were made at the regular follow-up visit intervals where families were given the choice between another video- and in-person consultation. In case of suspicion of complex symptoms (e.g., autism spectrum disorder or severe muscle tone regulation disorders) or medical indications, an in-person consultation with standardized testing was arranged in a timely manner.
HEALTH CARE PROFESSIONALs' EXPERIENCES WITH VIDEO- AND IN-PERSON CONSULTATIONS
Seven health care professionals (physicians, physiotherapist, occupational therapist, psychologist) with >25 video consultations were surveyed about their experiences with video- in contrast to in-person consultations. The descriptive analysis excluded some responses due to incomplete or invalid data or specialist expertise. Participants reported that between 1% and 10% of the video consultations were incomplete, mainly due to incomplete medical history (mean 5.4%), examination (8.3%), or screening for developmental delay (10.0%).
Incomplete video consultations are often disrupted due to an unstable internet connection, which accounts for 50–80% of cases. Lack of cooperation was named as a reason for the child in 5–30% or the parents in 5–15% of cases. Exhausted time resources or other unspecified reasons were also given from individual respondents. Professionals reported that the missing parts could be made up in 65% (mean) of cases. The completion options were as follows: home videos through cloud (mean 33.6%), telephone call (31.1%), in-person consultation (24.3%), and video consultation (10.0%).
Health care professionals reported incomplete medical history (mean 9.3%), examination (11.5%), or screening for developmental delays (10.0%) in 1–25% of in-person consultations. The reasons for incomplete testing were varied, including lack of cooperation from the child (in 50–100% of cases), the parents (in 5–50% of cases), or time constraints for the examiner (in 0–15% of cases). The health care professionals (n = 6) stated that the missing parts could be made up in 67.5% (mean) of cases. The options given for completion were (n = 7) as follows: home videos through cloud (mean 6.4%), telephone call (3.6%), in-person consultation (55.7%), and video consultation (6.4%).
Health care professionals stated that the time required for the video- and in-person consultations is the same for children up to the corrected age of 12 months. From a corrected age of 24 months to school entry, the video consultation took less time because the adapted screening for developmental delay required less time than the standardized on-site assessment (60–90 min vs. 120 min).
All participants indicated that the video consultation is generally suitable for identifying developmental delays in this group. One participant limited the suitability with regard to the physical examination of children aged ≥1 year.
Discussion
This study presented an adaptation of developmental neurological follow-up visits for children born preterm and high risk for video- compared with in-person consultations. It is feasible to adapt the in-person to a video consultation with the aim of recognizing developmental delays in a standardized manner and to initiate interventions. Active participation of parents in examinations and test situations allows a better insight into their child's development.
A survey on the health care professionals' experiences with video- and in-person consultations found that the rate of incomplete follow-up visits and resources for medical history, personnel, and time remained constant. All participants stated that the video consultation is generally suitable for identifying developmental delays in children up to an age of 6 years with one exception.
The tests adapted for video consultation do not represent reliable and valid assessments for cognitive, motor, and language development. As the implementation of telemedicine progresses, there is a need to develop and evaluate objectified and standardized tests. Until these are available, the expertise of the investigators is of particular importance. 9 According to Bain et al., it is not possible to assess children <1 year of age through telemedicine. 31
In the follow-up visits of our center, children are routinely examined before their first birthday at corrected 3 and 6 months, so these conceptions had to be adapted. The HINE could be performed effectively with parental guidance, except for reflexes. In our cohort, especially children up to an age of 1 year could be examined without significant complications by their caregivers. Even muscle tone could be assessed by predetermined items.
There are more limitations in the neurological examination of children from the age of 1 year, because a standardized examination of muscle tone without palpation is not possible. The Child Neurology Society also concluded that an assessment of spasms or similar is not possible. An alternative consultation, for example, due to a pandemic or other challenges, should also be available in the future. 32 The greatest limitations concern the general pediatric examination, with an assessment of the general, nutritional, and nursing status, as well as a screening for dysmorphia and deformity, as also reported by DeMauro et al. in 2021. 19
The prerequisite for video consultation is sufficient knowledge of German or English to enable communication. In the case of non-native speakers, the medical history and examination are more difficult, since in an in-person consultation the interaction is more effective thanks to the possible use of facilitating communication and gestures. Video consultation is a challenge for parents, especially if only one parent is present. During the medical history and examination, the child needs to be cared for.
In addition, parents must provide camera guidance simultaneously with the instructions of the assessments. Unpredictable interruptions to the appointment, for example, by siblings or doorbells, are perceived as disruptive. 19 Families need to provide an email address and a terminal device with appropriate image quality. Dependence on a solid internet connection and software is a fundamental issue. Problems in this regard can lead to an immediate termination of the appointment and a delay in scheduling with subsequent patients. Patients and professionals must be capable and motivated for modern communication media to be used in patient care. 15
The survey results indicate that incomplete follow-up visits and those that could be made up for are similar. Furthermore, all but one of the health care professionals stated that video consultations are generally suitable for identifying developmental difficulties. This suggests that video consultations could be a useful option for follow-up visits when in-person consultations are not possible.
The survey has limitations as it only includes a small number of health care professionals working in the specific area and with sufficient experience with video consultations. In addition, the respondents had different professional and age-related specializations, making it difficult to conduct a uniform survey and evaluate experiences.
To ensure a reliable comparison between video- and in-person consultations, prospective, multicenter studies with a larger number of cases should be conducted. This will provide a more comprehensive evaluation of the suitability and efficiency of video consultations compared with in-person consultations. Infection protection for patients and staff is ensured by the video consultation. As a result, staff from risk groups (pregnancy, pre-existing conditions) can be easily integrated into digital follow-up care.
A survey of employees who work with telemedicine indicates a high level of satisfaction at 93%. Telemedicine as a part of follow-up visits is recommended by 89% of staff at this survey 9. There was no need for the families to travel to the outpatient clinic, hence saving time and financial resources. At the same time, the integration of the visits into everyday life was facilitated.
For both parents and therapists, the video consultation offered a great deal of flexibility, as it allowed for convenient or necessary interruptions of the appointment; for example, due to sleeping times, eating, crying, etc. Children show a carefree behavior, since there was no phase of acclimatization to a foreign environment or strangers in the home environment. Thus, the usual play behavior was observed from the onset.
Parents conducted the examination of their own child in the home environment. Several examiners were able to assess the child at the same time. This was also possible from different locations, and facilitated an interdisciplinary, economical, and patient-oriented collaboration. Telemedicine can be efficient and satisfactory, shown by 2,093 contacts at pediatric neurology in Philadelphia. 8
In test theory, a valid score with many items is required to validly assess a child's performance. For multiple reasons, this is not possible in the video consultation. Further limitations were reduced language skills and technical requirements.
In summary, despite some limitations, video consultation can be considered an alternative to in-person consultation, especially if the latter is impossible. A follow-up of preterm and high-risk infants at the age of 3 months to 6 years must always be provided, regardless of specific populations or individual situations. A structured adaptation for video consultation was necessary due to the pandemic and should also be available in the future.
Footnotes
Acknowledgments
The authors thank for the technical support, especially the data protection compliant cloud of the University Hospital Essen for uploading patient videos and Zava Sprechstunde Online GmbH, Essen, Germany.
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors L.C., B.A., and B.M.H. received funding from Stiftung Universität Essen foundation, which supported video consultation as part of its COVID-19 projects (20204699123), and B.A. has received funding from the University Duisburg-Essen, Faculty of Medicine, Clinician Scientist Academy.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.