
Abstract
Background:
After-hours telemedicine services for emergency care are thought to offer a solution for patients who live at a distance from traditional face-to-face emergency services. This study evaluates such a service in a Health Maintenance Organization, focusing on the differences between central and peripheral populations.
Methods:
In this cross-sectional database study, we collected data regarding the encounter and patient characteristics, including prescriptions, referrals for further evaluation in a traditional emergency department (ED), and the distance from a traditional ED. Other outcome measures included health care utilization after the encounter such as primary care physician (PCP) encounters, additional telemedicine encounters, ED visits, and hospitalization.
Results:
In total, 45,411 patient visits were analyzed. Medication was prescribed in 25% of the encounters, and a referral to an ED was given in 22%. In total, 17.7% of the patients visited an ED within 24 h of the index encounter. In total, 64.8% of patients visited a PCP in the following 30 days. No further care was needed in 32.4% of the encounters. In multivariable logistic regression, the odds of using the service were lower for low socio-economic status groups and inhabitants of the periphery than the central areas. A weak reverse correlation was observed in Jewish sectors regarding distance from traditional ED, whereas no correlation was found in the Arab sector.
Conclusion:
It is commonly believed that telemedicine overcomes geographical barriers. The results of this research do not support this hypothesis.
Introduction
Telemedicine experienced a pronounced increase in utilization during the COVID-19 pandemic, partially owing to social distancing guidelines and a fear of infection. In the United States, there was a threefold increase in telemedicine consultations in the month following the official declaration of the pandemic in March 2020. 1 This surge encompassed all modalities of telehealth services, such as video consultations, telephone encounters, and secure electronic messaging. 2 As telemedicine became recognized as a useful tool for efficient and safe health care communication, there was an increase in “after-hours telemedicine” services that offered to treat patients who required care that they felt could not be deferred until the next day. 3 –5
Israeli Health Maintenance Organizations have established such after-hours services following the pandemic. 6 These services offered an on-call nurse or physician who consulted via phone or video, assessed the patient’s condition and sent a prescription, directed them to a traditional emergency department (ED), or advised a follow-up with their primary care provider upon clinic reopening. These new services catered to a growing need for accessible medical advice during nontraditional hours, potentially mitigating the pressure on physical health care facilities and EDs. 7
During the pandemic, patients who were already familiar with telemedicine and many first-time users embraced the technology and have continued to use telemedicine for primary care encounters ever since. 8 Many doctors seem unenthusiastic about telemedicine 9 and there’s an ongoing debate about who benefits more from the convenience of telemedicine, doctors or patients. 10 Despite the expanded provision and coverage of these services, there are still documented disparities in their utilization. 11,12 Numerous factors, including age, socioeconomic status, geographic location, ethnic background, lack of digital access, and limited technological literacy, have been recognized as influencing the use of telemedicine. 13 –16 In Israel, the populations that are prone to disparities in telemedicine utilization are vulnerable populations, such as some Arab communities, those living in the periphery, and individuals with low technological literacy. 17
Meuhedet Health Services (MHS) is the third largest Health Maintenance Organization in Israel, responsible for the care of 1.3 million individuals across all regions of Israel. MHS introduced a telemedicine service designated for urgent care in 2020, offering after-hours consultations with primary care physicians (PCPs) through phone and video. Hereafter, this service will be known as “Tele-ED.” Although research data is available on pediatric after-hours telemedicine, 3,5,18 similar information for adult patients is scarce.
The operational framework of the MHS Tele-ED which is provided free of charge was strategically designed to address health care accessibility challenges, particularly for residents in peripheral areas. This contrasts with traditional ED visits, where a fee is charged unless the visit is a result of a physician’s referral. On weekdays, the Tele-ED operates from 19:00 h until 7:00 in the next morning. During weekends and public holidays, it transitions to a continuous 24-h service. The objectives of this study were to evaluate the Tele-ED service, by analyzing the demographic and clinical characteristics of the patients and to examine the nature of their encounters, with a special focus on the differences between central and peripheral populations.
Methods
For this cross-sectional study, we used information extracted from MHS central databases that store medical and demographic information for all MHS patients, ensuring patient confidentiality and compliance with ethical standards. The information included visit diagnoses, laboratory test results, medications prescribed and dispensed, results of imaging studies, ED visits, and hospital admissions. Participants had access to telemedicine through their phones or computers with internet connectivity. The telemedicine platform supported phone calls and video calls.
STUDY DESIGN AND POPULATION
We identified all Tele-ED encounters conducted via telephone or video between March 2021 and December 2021, a year after the Tele-ED service was launched. We included the first encounter for each patient (the index encounter) who was insured by MHS throughout the entire study period.
We extracted the following variables from the database: age, sex, ethnicity, or sector (Arabs, non-Orthodox Jews, ultra-Orthodox Jews), socio-economic status (SES), the geographic region in Israel (northern, central, southern regions, and Jerusalem, including its adjacent areas), and the patient’s primary care clinic. The cities in Israel with a mixed Jewish–Arab demographic, classified by the Israel Central Bureau of Statistics as locales where both “Arabs” and “Jews” each constitute over 10% of the population, were categorized under the non-Orthodox Jewish segment for this analysis. Clinical data included chronic medical conditions: asthma, cerebrovascular accident, chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), congestive heart failure, diabetes mellitus (DM), hypertension, ischemic heart disease, and oncological conditions. DM and oncological conditions were identified using relevant registries, CKD was defined as an estimated glomerular filtration rate of below 60 mL/min/1.73 m2 calculated using the MDRD study equation. The other chronic conditions were identified from the diagnosis field in the patients’ charts.
Index encounter characteristics
We extracted data regarding the Tele-ED index encounter characteristics: date and time, number of prescriptions given and purchased within 14 days, referrals to an ED, and ED visits within 24 h of the index Tele-ED encounter.
Health care services utilization before and after the Tele-ED encounter
To understand the patterns of primary care utilization before the Tele-ED encounter, we extracted the number of face-to-face, telemedicine encounters and online requests with PCPs during the three months preceding the Tele-ED encounter.
The outcome measures were health care services utilization after the Tele-ED encounter: the number of PCP encounters, additional Tele-ED encounters, prescriptions that were prescribed, ED referrals, and hospitalizations. These variables were extracted for three different periods: the first 30 days following the Tele-ED encounter, from day 31 to day 60, and from day 61 to day 90 after the Tele-ED encounter.
STATISTICAL ANALYSIS
We described patients’ characteristics using proportions for all categorical variables and used the chi-square test to examine the association between two categorical variables. We used medians and interquartile range (IQR) to describe the distribution of nonnormally distributed parameters.
The encounter hour was categorized as: “morning” if the encounter took place from 7:00 to 12:59, “afternoon” for 13:00–18:59, “evening” for 19:00–0:59, and “night” for 1:00–6:59.
Age was categorized into five groups: 0–6, 7–18, 19–45, 46–65, and 66 and older.
“Completion of care” was defined as no additional encounters with the Tele-ED, or a PCP, and no admissions to an ED within 30 days following the index encounter.
We defined the patients’ distance from the nearest ED as the air distance between the patient’s primary care clinic and the nearest ED. We used Spearman’s rank correlation to assess the correlation between distance and Tele-ED use.
We used binary logistic regressions for multivariable analysis that calculated the association between the different demographic factors and the odds of using the Tele-ED service.
We used R version 4.1.0 (R Foundation for Statistical Computing) for all statistical analyses. Two-tailed p values are reported with α = 0.05.
The study was approved by MHS’ Institutional Review Board (number 07-18-08-21).
Results
THE ENCOUNTERS AND THE PATIENTS
Between March 2021 and December 2021, at least one Tele-ED encounter was recorded for 45,411 patients. Men constituted 45.3% (20,586) of the patients. The median age was 25 (IQR 6–41). The most prevalent chronic condition was asthma (17.9%), followed by hypertension (12.2%).
A medication was prescribed in only 25% (11,367) of the encounters. Completion of care was achieved in 32.4% of the encounters (14,719). A referral to the ED was given in 22% of the encounters (9,993). An ED visit within 24 h of the index encounter occurred in 17.7% of the patients (8,030), with or without a referral. In the following 30 days, 29,422 of the patients (64.8%) visited a PCP and 37,911 patients (83.5%) visited a PCP during 90 days after the index encounter (Table 1).
Patient Characteristics by Tele-ED Shift
Missing information for 669 patients.
Missing information for 24,134 patients.
CHF, congestive heart failure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident; DM, diabetes mellitus; ED, emergency department; ISD, ischemic heart disease; IQR, interquartile range; PCP, primary care physician; SES, socio-economic status.
DEMOGRAPHIC AND GEOGRAPHIC DISTRIBUTION OF THE PATIENTS
The proportion of patients who used the Tele-ED service during the study period differed by gender, age group, sector, SES, and geography.
In multivariable logistic regression, the odds for using Tele-ED service during the study period were smaller for males, for all age groups compared with young children, and for habitants of all the geographic regions in Israel compared with the central part of the country. The odds were higher for the higher SES groups and for Jews compared with Arabs (Table 2).
Tele-ED Utilization Proportions and Adjusted a Odds Ratios for Using the Service by Patient Characteristics
Results of binary logistic regression controlled for the presented variables.
CI, confidence interval.
Fig.1 presents the correlation between the distance of the primary care clinic from the nearest ED and the proportion of the clinic’s patients who used the Tele-ED service at least once during the study period: there was a weak reverse correlation in non-Orthodox and ultra-Orthodox Jewish sectors (Spearman’s r −0.22 and −0.27, respectively) and no correlation in the Arab sector.
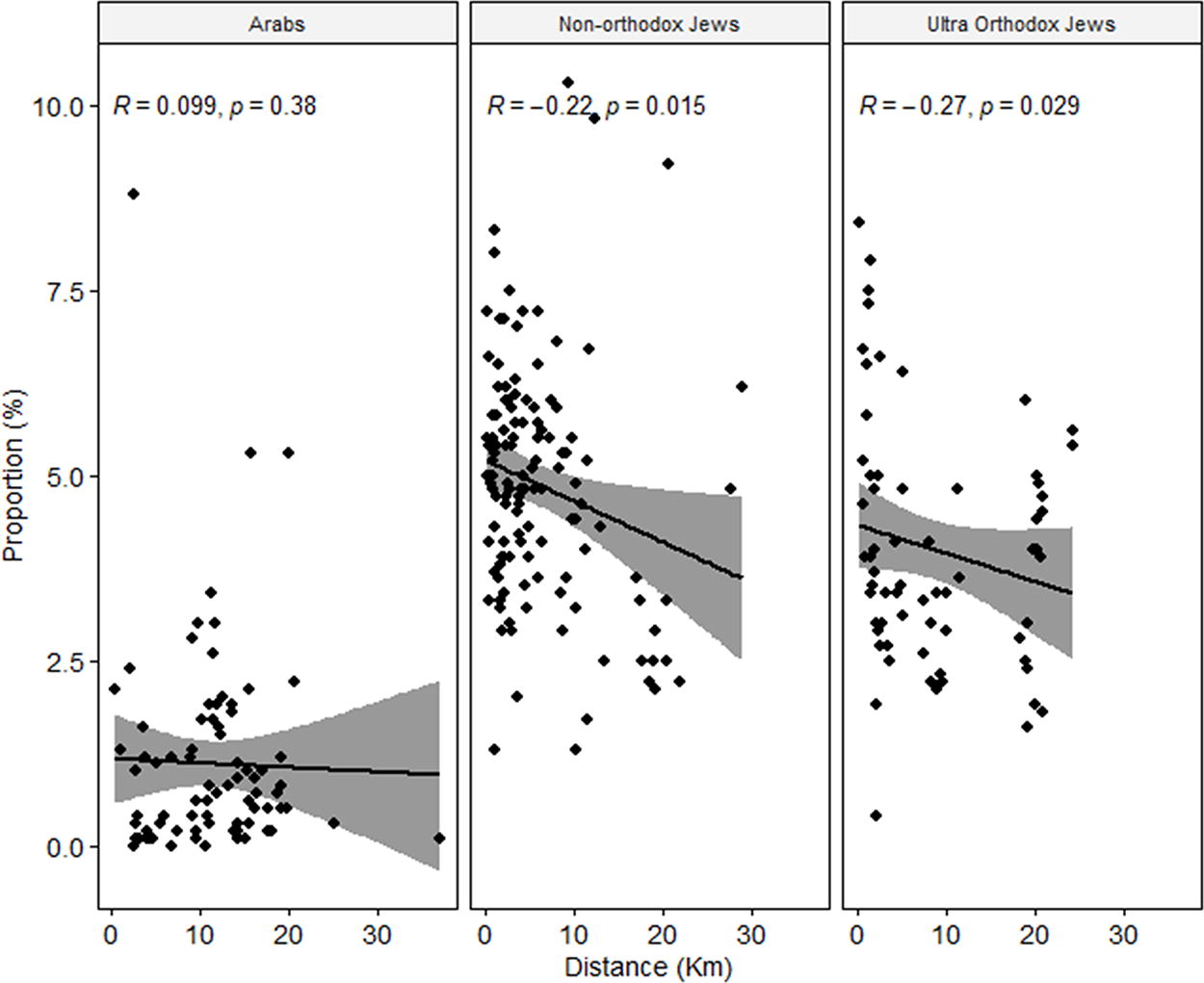
Correlation between aerial distance to the nearest traditional ED and Tele-ED utilization by ethnic group. The figure shows scatter plots depicting the correlation between the distance of the primary care clinics to the nearest traditional ED and the proportion of Tele-ED utilization among the clinic’s patients, in three ethnic groups: Arabs, non-Orthodox Jews, and ultra-Orthodox Jews. Each point represents a primary care clinic. The x-axis measures the distance in kilometers, whereas the y-axis represents the proportion of Tele-ED utilization among the clinic’s patients expressed as a percentage. The line of best fit is accompanied by a shaded area, indicating the 95% confidence interval. Spearman’s correlation coefficients
THE CHARACTERISTICS OF NIGHT SHIFT ENCOUNTERS
Most (62%, 28,158) of the encounters occurred during the evening and the afternoon (20%, 9,099), whereas 5,527 (12%) of the encounters happened during the night shift (1:00–7:00). The patients who used the Tele-ED during the night shift had fewer chronic conditions.
Thirty four percent of the night encounters resulted in referrals to the ED compared with 20% during the rest of the day (p < 0.001), 25% of the night shift patients visited the ED on the following day compared with 17% of the patients who used the Tele-ED in other shifts (p < 0.001). Fewer prescriptions were provided in night shift encounters (14% vs. 27% in the other encounters, p < 0.001). The patients who used the Tele-ED during the night shift had fewer visits to their PCPs during the 7 days that followed compared with patients who had evening and afternoon Tele-ER encounters (37% vs. 43%, p < 0.001) (Table 1).
PATIENTS WHO HAD ADDITIONAL TELE-ED ENCOUNTERS DURING THE 90 DAYS THAT FOLLOWED THE INDEX ENCOUNTER
Within the 90 days following the index encounter, 6,621 patients had 1–2 additional Tele-ED encounters, and 696 patients had 3 or more additional encounters. These patients were children aged 0–6 (34%, 33%, vs. 24% for patients who had 3+ encounters, 1–2 encounters, and none, respectively) and young adults aged 19–45 (42%, 40%, vs. 39% for patients who had 3+ encounters, 1–2 encounters, and none, respectively). Their distance to the closest ED was lower (median distance: 2.50 km [1.50, 5.22], 2.85 km [1.50, 6.76], and 3.11 km [1.61, 7.92] for patients who had 3+ encounters, 1–2 encounters, and none, respectively, p < 0.001). More of them visited a PCP during the 7 days that followed the index encounter (53%, 49%, vs. 41%, p < 0.001) (Table 3).
Patients’ Characteristics and Tele-ED Encounter Outcomes by Number of Additional Tele-ED Encounters
Missing information for 669 patients.
Missing information for 24,134 patients.
In multivariable logistic regression, using variables that were significant in univariable analysis, the odds for additional Tele-ED encounters during the study period were higher for non-Orthodox and ultra-Orthodox Jews compared with Arabs (odds ratio [OR] = 1.42 and confidence interval [CI] 1.23–1.65, OR = 1.21 and CI 1.05–1.41, respectively), and for patients with asthma (OR = 1.23, CI 1.15–1.31), COPD (OR = 1.28, CI 1.13–1.45), or hypertension (OR = 1.24, CI 1.12–1.37). A minor but statistically significant inverse relationship was observed concerning the distance from the primary care clinic to the ED (OR = 0.985, CI 0.98–0.990).
Out of the 7,317 patients with at least one additional Tele-ED encounter, 592 (8%) had no visits to PCPs during this period. Among these 592 patients, a significant proportion (58%) was young adults aged 19–45 compared with 39% among those who had additional Tele-ED encounters and visited a PCP. They were healthier; however, they received more prescriptions in the index Tele-ED encounter (36% vs. 28%, p < 0.001), and fewer of them were hospitalized (4% vs. 8%, p < 0.001) (Table 4).
Comparison of Health Care Outcomes Based on Primary Care Physician Visits Post-Tele-ED Encounter
Missing information for 669 patients.
Missing information for 24,134 patients.
Discussion
The utilization patterns of the Tele-ED service reveals insights into patient behavior and the effectiveness of telemedicine in addressing after-hours health care needs. The service was used more by younger, healthier, and higher SES individuals, aligning with existing telemedicine literature. 13
Other racial and ethnic minorities have shown lower rates of video-based telemedicine during COVID-19. 19,20 In a comprehensive study conducted in Israel, examining telemedicine use in primary care clinics during the pandemic, ethnicity was the most discriminative variable associated with using telemedicine, with 85% of users among the Jewish population compared with only 52% among the Arab population. 16 Our data showed that a lower proportion of the Arab population used Tele-ED compared with the Jewish population. A study from 2007 presented differences in health care utilization patterns among Arabs and Jews, with Arabs’ preference toward visiting family physicians whereas Jews visited more specialists. 21 Interactions with Tele-ED physicians similarly to those with specialists typically occur without any prior acquaintance between the patient and the physician. This lack of a pre-existing relationship along with cultural differences, and lower health literacy, may contribute to the reduced frequency of Tele-ED service utilization among the Arab population.
Differences in socioeconomic status, geographic location, and technological literacy appear to contribute to the disparities observed in telemedicine utilization. For example, low SES groups and those living in peripheral areas had lower odds of using the Tele-ED service compared with higher SES groups and those in central areas. This suggests that socio-economic and geographical disparities impact usage of telemedicine services. In our study, the Arab population, which predominantly resides in peripheral areas with lower SES, 22 demonstrated lower utilization rates of the Tele-ED service. The ultra-Orthodox Jewish population, another significant group within our study, also exhibited lower rates of Tele-ED service utilization. The latter group often faces unique barriers, including lower rates of internet usage and technological literacy. 23 However, since the Tele-ED service was also offered via phone calls which are available in all geographic regions and population groups in Israel, differences in technological literacy and internet availability may not fully explain these observed differences. Future studies should be directed at understanding the root causes of these differences. Efforts should be directed toward improving telemedicine services’ accessibility and culturally appropriateness for all population groups, as well as improving health literacy and enhancement of technological infrastructure.
It is commonly believed that telemedicine overcomes geographical barriers. 24,25 Our results do not support this hypothesis: in both non-Orthodox and ultra-Orthodox Jewish sectors, a weak reverse correlation was observed, whereas no correlation was found in the Arab sector. This suggests that distance from traditional ED facilities does not significantly drive the usage of Tele-ED services. We assumed that Tele-ED usage during the night shift (1:00–7:00) would be for the “truly urgent cases.” The findings revealed fewer prescriptions and more ED referrals during the night but not a corresponding increase in hospitalizations. This suggests that night shift encounters did not deal with genuinely urgent cases. The difference between the number of referrals and actual hospital admissions at night raises concerns about the criteria for referring patients to the ED. A visit to the ED without a referral that does not result in an admission must be paid by the patient, whereas a referral given in a Tele-ED encounter exempts the patient from this payment, potentially driving patients to use the Tele-ED service before going to the ED. This behavior suggests that, beyond health care needs, economic considerations significantly influence how and why patients engage with different health care access points, particularly in emergencies. 26 –28
Although our findings highlight the limitations of telemedicine in overcoming barriers in a small country such as Israel, the effectiveness of telemedicine could vary significantly in larger regions or globally. For instance, telemedicine has shown substantial benefits in countries such as Canada, where virtual care surged during the COVID-19 pandemic. In 2020, 92% of Canadians had broadband access, and virtual care visits increased from 1.6% of total ambulatory visits in 2019 to 70.6% in 2020, demonstrating significant uptake in response to the pandemic. 29
Similarly, in Australia, telemedicine played a crucial role during the pandemic, especially in rural and remote areas where access to health care is often limited. The Australian experience underscores the potential of telemedicine to bridge gaps in health care access in diverse geographic settings. 30
After the pandemic, the use of telemedicine has continued to be robust in these countries, with many health care systems adopting a hybrid model that combines in-person and virtual care. This approach has maintained high levels of patient satisfaction and access to care, particularly among populations that previously faced significant barriers to health care. 29,31
The analysis of repeat Tele-ED usage within 90 days reveals complex patterns in health care utilization. Patients with multiple Tele-ED encounters also often frequently visit PCPs, suggesting that Tele-ED may not replace but rather supplement traditional care. This trend is particularly noticeable among young children, young adults, and those living closer to traditional EDs. However, a subset of patients, primarily healthier young adults, used Tele-ED multiple times without subsequent PCP visits. This group tends to use Tele-ED as an alternative to primary care, possibly for straightforward needs such as prescriptions, as indicated by their lower hospitalization rates.
These findings imply that Tele-ED serves a dual role: as a complementary service alongside regular health care for some, and as an alternative pathway for specific health care needs for others. This underscores the need to understand Tele-ED’s integration into the broader health care system and its impact on health care delivery.
Strengths and Limitations
The major strength of this study is its large national cohort of patients. Analyzing these data provided insights regarding the patients who used Tele-ED and their usage patterns.
A key limitation of this study was the lack of access to individual medical files, which restricted in-depth analysis of health information and urgency assessment. This should be addressed in future studies.
Conclusions
This study emphasizes that Tele-ED usage is influenced by socioeconomic, cultural, and other factors, particularly evident in differing usage patterns between Jewish and Arab populations. The dual role of Tele-ED, serving both as a complement to primary care and as an alternative route for specific health care needs, highlights its complex role in health care delivery. These insights call for a more nuanced approach to its implementation, emphasizing the importance of addressing diverse demographic and cultural factors to ensure equitable health care access.
Ethical Approval
Ethical approval for this study was obtained from MHS Ethical Committee.
Footnotes
Authors’ Contributions
J.B.: Conceptualization (lead); methodology (equal); writing—original draft (lead); writing—review and editing (equal). A.D.H.: Methodology (equal); writing—original draft (supporting); writing—review and editing (equal); supervision (supporting). G.Z.: Methodology (equal); formal analysis (lead); writing—original draft (supporting); writing—review and editing (equal); supervision (lead).
Disclosure Statement
The authors of this study declare that there are no conflicts of interest related to this research.
Funding Information
The authors have not received any financial or nonfinancial support that could have influenced the design, conduct, or reporting of this study.