
Abstract
Before the Covid-19 pandemic, human-centered design work in San Francisco found video visits promising for Medicaid-insured pregnant individuals. They were deemed likely better than phone at addressing concerns about remoteness. We describe our experience with introducing video visits within a safety net clinic that had rapidly adopted phone visits as the standard telemedicine option early in the pandemic. By utilizing Kotter’s change framework, providing an equity-focused vision, and supporting the implementation with a skilled, on-the-ground project manager, temporary uptake of offering video visits was achieved. However, competing priorities, staffing structure, and institutional culture were barriers to creating sustained change once grant funding ended, even after improvement of digital infrastructure. Efforts to increase video visit uptake in systems where telephone visits are the norm—as is in many safety net systems—may have limited success without leadership-driven prioritization and culture change at all levels.
Introduction
Medicaid-insured individuals face barriers including transportation to accessing prenatal care. 1 Thus, in 2017–2018, we conducted a human centered design process with pregnant residents of San Francisco and identified telemedicine as a promising intervention. 2 Concerns about trust with the clinician were raised, particularly for people of color. 3 In 2019, we aimed to pilot remote visits, hoping video would mitigate the risk of visits feeling “too impersonal”. Prior to pilot implementation, the COVID-19 pandemic accelerated telemedicine adoption and telephone visits became the standard in our clinic. In this report, we describe our use of Kotter’s Change Model 4 for our video visit implementation process, our results and learnings. Our goals included: (1) screening and offering eligible patients a video visit, (2) successful completion of video visit, and (3) development of sustainable workflows for offering and conducting video visits.
Pilot implementation took place in our high-risk obstetrics (HROB) clinic. HROB clinic is held in the Obstetrics, Midwifery & Gynecology clinic (OMG) within the San Francisco Department of Public Health (SFDPH)-operated safety net hospital.
Implementation Plan
We assembled an implementation team that held the positions and expertise to reach all stakeholders: medical providers, medical assistants (MAs), nurses, schedulers, and health system leadership. We used Kotter’s 8 Step Process for Leading Change, based on its “bottom-up” approach 4 and executed the implementation over a 24-month period (Fig. 1).
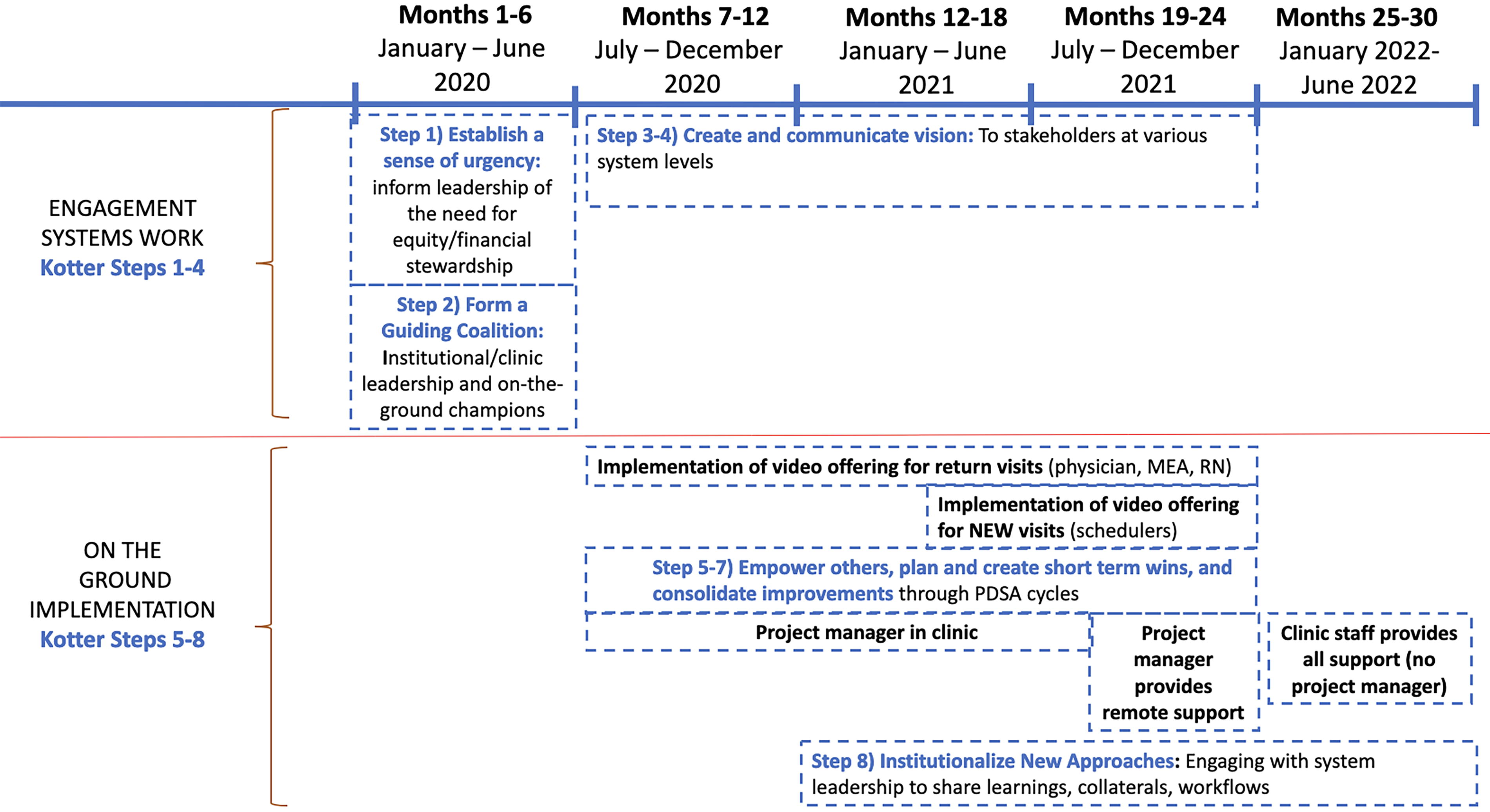
Implementation Timeline.
STEP 1: CREATE A SENSE OF URGENCY
Our SFDPH-run safety-net system (San Francisco Health Network, or SFHN) prioritizes high-quality care, and both equity and financial stewardship are in our True North goals. 5 To underscore the urgency for offering video visits we highlighted: (1) design findings indicating Medicaid-insured pregnant individuals’ concerns about impersonal telemedicine, (2) national standard of video visits in telemedicine, routinely offered to privately-insured patients in San Francisco; and (3) the risk that payors would not reimburse for phone visits beyond the public health emergency. In short, offering telephone-only telemedicine represented a care inequity between Medicaid- and privately-insured patients, and may not be financially sustainable.
Early communications uncovered leaders’ and clinicians’ doubts regarding our safety-net patients’ technology, internet access and interest in video visits. In response, we conducted a 2-week study which demonstrated that almost 70% of our patients had no barriers to video visits and wanted to be given this option. 6 This data supported the integration of video visits for patient-centered, equitable care.
STEP 2. Form A POWERFUL GUIDING COALITION
Engaging leaders and on-the-ground champions led to building a guiding coalition with diverse expertise and strategic positions. Notably, because of parallel leadership and staffing structures within OMG, where staff (MAs, nurses and schedulers) are employed by SFDPH and physicians by the partnering academic institution (University of California San Francisco-UCSF), leaders from both institutions were critical; they included the OMG clinic manager and Patient Access Supervisor (both SFDPH) who oversee the clinic staff, and the OMG medical director (UCSF) who oversees the physicians. In addition, we engaged the SFHN Assistant Chief Medical Officer for Specialty Care, recognizing that sustainability would be more likely if SFDPH leadership viewed the pilot as an opportunity to inform expansion to their other clinics. On-the-ground champions for various team members (MAs, nurses, schedulers, and clinicians) were critical in identifying implementation barriers and solutions, and encouraging colleagues to adopt the change. Our Project Manager (PM) was initially anticipated to have an operational role, but became a vital coalition member. She sought champions who were enthusiastic, dedicated to the goal, and recognized as “influencers” by colleagues. She also developed relationships with on-the-ground staff and clinic leaders leading to transparent feedback; engaged in real-time problem-solving; and consistently followed-up with those struggling with change. These skillsets were critical given she did not have preexisting clinic relationships and was implementing a change that was not an institutional priority.
STEPS 3–4: CREATE AND COMMUNICATE A VISION
We had two primary goals: (1) convey urgency aligned with our clinic community’s mission and (2) engage all care team members in practice change. Using diverse communication methods (email, infographics, 1-on-1 interactions, huddles, and team meetings) we consistently delivered the vision and assured support.
STEPS 5–7: REMOVE OBSTACLES; GENERATE SHORT-TERM WINS; AND SUSTAIN ACCELERATION TO PRODUCE MORE CHANGE
These steps relied on our PM’s continuous engagement with front-line staff/clinicians, understanding challenges, collaboratively problem-solving, and supporting the adoption of new processes. Problem-solving often involved PDSA (Plan-Do-Study-Act) cycles and/or group engagement for understanding challenges and identifying solutions. An example of an obstacle that arose during implementation included schedulers feeling that offering video visits required additional patient support and, thus, time. This was addressed by implementing a “telemedicine support referral pool” through the EHR, which could provide additional support to patients and was sustained through volunteers.
STEP 8: INSTITUTIONALIZE NEW APPROACHES
To solidify video visits as routine practice, we collaborated with OMG leadership to train all staff. We created training materials and “standard work” with approval from SFDPH for official employee use. Throughout our pilot, we engaged operational leaders in creating sustainable processes, including trainings and patient-facing technical support extending beyond grant-sustainable processes, including trainings and patient-facing technical support extending beyond grant-supported initiatives.
Learnings
IMPLEMENTATION UPTAKE
Key metric insight: During our pilot, the offering rate for video visits was 70% when the PM was in clinic (1/2021–9/2021). Post-PM departure, in the sustainability phase (10/2021–6/2022), the overall offering rate decreased to 37%, aligning with a lower percentage of video visits (Fig. 2).

Video visits as a percentage of total telehealth visits.
The correlation of PM presence with higher rates of HROB video visits contrasted with SFDPH’s Behavioral Health Services (BHS) program, which implemented video visits concurrently to OMG without dedicated project management. BHS serves a similar marginalized patient population of SF residents but is under separate leadership from the SFHN Ambulatory Care system in which OMG is housed. In 2021 and 2022, ∼30% of telemedicine visits at BHS were conducted via video; in contrast at OMG, the video visits were never > 10% of telemedicine visits. (Fig. 2: Video visits as a percentage of total telehealth visits within OMG HROB clinic (pilot site), OMG, and BHS. Data for pilot site only available during the time of the pilot (1/2021–6/2022)).
Challenges
Despite local leadership support in the OMG clinic, several factors presented challenges to implementation. As an SFDPH-run system with unionized staff members, implementing new workflows is challenging without system-wide mandate across the SFHN. Within BHS, the director made video implementation a system priority and by April 2020, 400+ behavioral health clinicians were mandated to attended trainings, clinician licenses for video-visit software were provided, and all clinics were furnished with video devices by early 2021. In contrast, SFHN Ambulatory System leadership did not put these changes in place, hindering the OMG’s leadership team’s ability to push the practice change. In addition, the clinic’s parallel staffing and management structure, and their system of rotating resident physicians every 4–6 weeks, made it challenging to deliver coordinated and universal messaging and support around the practice change.
Nine months post-pilot, SFHN invested into video-enabled devices (e.g., tablets) for the clinics and implemented a new electronic health record (EHR)-embedded video visit platform (September 2022). This provided significant provider and patient-facing conveniences compared with the prior EHR; however, there was no leadership messaging, training, or metrics to encourage usage. As Fig. 2 demonstrates, the percentage of visits done via video remained lower than at BHS during this time, and lower than the rates achieved in HROB when the PM was providing on-the-ground support.
Discussion
The Covid-19 pandemic highlighted the importance of remote medical care and established telemedicine as a standard. While video-enabled visits are widely adopted across the United States, safety net systems—serving largely Medicaid and/or uninsured patients—predominantly utilize telephone visits. Although this modality may not be inferior to video-enabled telemedicine, 7,8 providing both options to patients is important to ensure equitable access and experience.
Our report highlights unique barriers in safety net settings, including more limited resources, competing organizational priorities, and biases that patients cannot or want to engage in video visits. In our setting, local data was critical in demonstrating the interest and ability of our patients, many of whom rely on smartphones for various types of communication, helping create motivation around implementation. Despite this data, on-the-ground support, and dedicated clinic leadership, video implementation was not an institutional priority at the time of our project, affecting sustainability. Serving a similar population, our SFDPH behavioral health clinics achieved higher and sustained rates of video-enabled telemedicine visits; we believe that differences in organizational prioritization played a major role in this noted outcome.
Clinics can successfully implement video-enabled visits without institutional support if there is dedicated on-the-ground support. We recommend employing a dedicated project manager with a skillset that will enable fostering relationships, addressing issues in real-time, and engaging quality improvement strategies to optimize workflows and success. Continuing to advocate for institutional prioritization and infrastructure support is also critical, as evidenced by uptake rates declining postwithdrawal of in-person support. Nationwide, for safety-net patients to access video-enabled telemedicine equitably, additional data on its benefits from both patient and provider perspectives is crucial. This information will enable safety-net system leaders to prioritize video visit implementation.
Footnotes
Acknowledgments
This work was supported by
Disclosure Statement
The authors disclose no conflicts of interest.
Funding Information
No funding was received for this article.