
Abstract
Introduction:
Preanesthesia teleconsultation helps reduce availability constraints as well as direct and indirect expenses. The TELECAM trial was performed to assess the quality of preanesthesia teleconsultation in terms of clinical parameters evaluation, feasibility, patient satisfaction and preoperative anxiety, and anesthesiologist satisfaction.
Methods:
TELECAM was an investigator-initiated, prospective, single-center, randomized, controlled, parallel group, evaluator-blinded, open-label study. Patients with a scheduled ambulatory surgery (orthopedic or hand surgery) were randomized into the in-person preanesthesia consultation group or the preanesthesia teleconsultation (conducted at the patient's home or workplace) group. The quality of the teleconsultation was evaluated through agreement on intubation difficulty, predictable mask ventilation difficulty, and American Society of Anesthesiologists (ASA) scores between the preanesthesia consultation and the preanesthesia in-person visit.
Results:
A total of 241 patients were included, and 208 were considered in the analyses. The feasibility of teleconsultation was high, with a feasibility ratio of 87.5%. The quality of the preanesthesia consultation regarding the evaluation of predictable intubation, mask ventilation difficulties, and ASA score, did not differ between the two groups (p = 0.23, 0.29, and 0.06, respectively). The preoperative satisfaction was higher for patients who had a preanesthesia teleconsultation (p = 0.04). Patients' preoperative anxiety did not differ between the two groups (p = 0.90). The median satisfaction of the anesthesiologists who performed the teleconsultation reached a maximum of 10 (IQR: 8.0; 10.0).
Conclusion:
This study showed positive results for the quality of preanesthesia teleconsultation on the evaluation of clinical parameters, with high feasibility and satisfaction of the patients and anesthesiologists. The trial was registered in ClinicalTrials (NCT03470896).
Introduction
According to French legislation, a preanesthesia consultation and a preanesthesia visit are mandatory before any surgery with anesthesia. 1 The preanesthesia consultation is generally carried out by an anesthesiologist from the institution where the surgery is scheduled and must be conducted 48 h to 3 months before the elective surgery. The preanesthesia visit must be carried out at the hospital entrance, the day before or the morning of the surgery (for ambulatory surgery), at the institution where the surgery is performed. The combination of a preanesthesia consultation and visit guarantees the patient's perioperative safety. The preanesthesia consultation traditionally requires the patient to travel to the hospital in which the surgery will be performed and entails availability constraints, as well as direct (travel costs) and indirect expenses (taking time off).
In this context, a 2001 French Society of Anesthesia, Critical Care and perioperative Medicine (SFAR) committee stated that “the anesthesia consultation may be carried out in a different establishment so that the patient may avoid having to make repeated journeys.” 2 Considering advances in communication technology over the past decade and to further reduce travel constraints, telemedicine could be an interesting tool for preanesthesia consultation.
Since 2009, telemedicine has had a legal and regulatory framework in France. 3 In 2017, the government's Investment Plan 2018–2022 funded the creation of a digital health ecosystem in France. 4 Digitizing the health system and broadband internet access throughout the country would help telemedicine develop in routine practice. Telemedical procedures include teleconsultations, which are intended to enable a medical professional to give a remote consultation to a patient.
Several studies and recent literature reviews have highlighted the positive benefits of telemedicine in preanesthesia evaluation, resulting in high patient and physician satisfaction and significant time and cost savings, while not increasing the surgery cancellation rate compared to in-person evaluation. 5 –17 However, such publications have focused on the feasibility of telemedicine for preanesthesia evaluation, patients' and caregivers' experience, and burden and/or costs. Notably, a pilot survey conducted in our center in 2015 showed that 85.4% of the 382 patients considered owned equipment that was compatible with carrying out a teleconsultation at home and 84.3% were fit for this type of consultation according to the anesthesiologists' opinion. 15 Nevertheless, studies investigating the quality of preanesthesia teleconsultation are much less numerous. 18 –21
Quality might be assessed through a process evaluation focusing on practical, technical, and/or organizational criteria of the teleconsultation. For example, in their recent observational noncontrolled study, Quemeneur et al. showed that among the 503 files of patients requiring a teleconsultation in anesthesia, 95% met the quality criteria defined by the High Authority of Health (e.g., test of the teleconsultation equipment, place where the teleconsultation was conducted, authentication of the physician, communication, organization of the teleconsultation). 21 Quality of the preanesthesia teleconsultation might also be assessed in terms of clinical parameters evaluation, that is, the ability to accurately assess clinical parameters at risk for anesthesia. Only the Applegate et al. study was a randomized controlled trial comparing the quality of preanesthesia evaluations by telemedicine and in-person consultations for 155 adults undergoing surgery in the United States (U.S.). 20
For the telemedicine group, the preanesthesia evaluation was performed at the surgery clinic (where telemedicine equipment was installed specifically for this trial) on the same day as the presurgery appointment. Their outcomes were surgical delay or cancellation, prediction of difficult airway management and concordance of the physical examinations. All results showed an equivalence between telemedicine and in-person evaluations, with high patient and physician satisfaction.
However, to the best of our knowledge, no high-quality study has assessed the quality on clinical parameters evaluation of preanesthesia teleconsultation conducted outside a medical place with dedicated technical equipment (i.e., patient's home or workplace). Thus, in their recent scoping review of alternatives to the in-person anesthesiologist-led preoperative evaluation in adults, Jonker et al. identified the need for high-quality research using high-level evidence designs. 22
In this context, the present study was performed using a randomized controlled design to evaluate the quality of preanesthesia teleconsultation on clinical parameters evaluation, and the feasibility of conducting this consultation at the patient's home or workplace, for French patients undergoing ambulatory surgery.
Objectives
Our primary objective was to assess the quality of preanesthesia teleconsultation on the evaluation of the predictable endotracheal intubation difficulty of patients with scheduled ambulatory orthopedic or hand surgery.
Our secondary objectives were to assess the quality of preanesthesia teleconsultation on the evaluation of predictable mask ventilation difficulty and the American Society of Anesthesiologists (ASA) score, as well as the preoperative anxiety and satisfaction of patients. The satisfaction of the anesthesiologist who conducted the preanesthesia teleconsultation and the feasibility of the teleconsultation were also evaluated.
Methods
This study complies with the Consolidated Standards of Reporting Trials (CONSORT) reporting guidelines (Supplementary Table S1). 23
Study design and oversight
The TELECAM trial was an investigator-initiated, prospective, single-center, randomized, controlled, parallel group, evaluator-blinded, open-label study. The intervention group consisted of patients who attended a preanesthesia teleconsultation, and the control group consisted of patients who attended an in-person preanesthesia consultation, as routinely conducted. The sponsor was the University Hospital of Nancy. A steering committee was responsible for the design and oversight of the trial and vouched for the accuracy and completeness of data as well as for the fidelity of the trial to the protocol and the statistical analysis plan. The trial was conducted in accordance with the principles of the Declaration of Helsinki and the Good Clinical Practice guidelines of the International Council for Harmonization and was approved by the appropriate French Ethics Committee (Comité de Protection des Personnes Du Sud-Ouest et Outre-Mer IV, acceptance on January 26, 2018, reference: CPP17-085a/2017-A03084-49).
Participants and follow-up
Patients were informed by the surgeon during the preoperative consultation for their scheduled ambulatory surgery (orthopedic or hand surgery) at the Emile Gallé surgical center (EGSC) of the University Hospital of Nancy. Patients were eligible to participate in the TELECAM trial if they were adults, in possession of technology equipment compatible with the video-conference platform (i.e., smartphone, computer, internet connection, webcam, microphone, and printer), and affiliated with the French Health Insurance program. Patients were excluded if they were pregnant, receiving psychiatric care, subject to a legal protection measure or deprived of liberty, or if they refused teleconsultation. All eligible patients who agreed to participate provided written informed consent between the preoperative and preanesthesia consultations and were followed until the day of the preanesthesia visit. Figure 1 summarizes the study process.
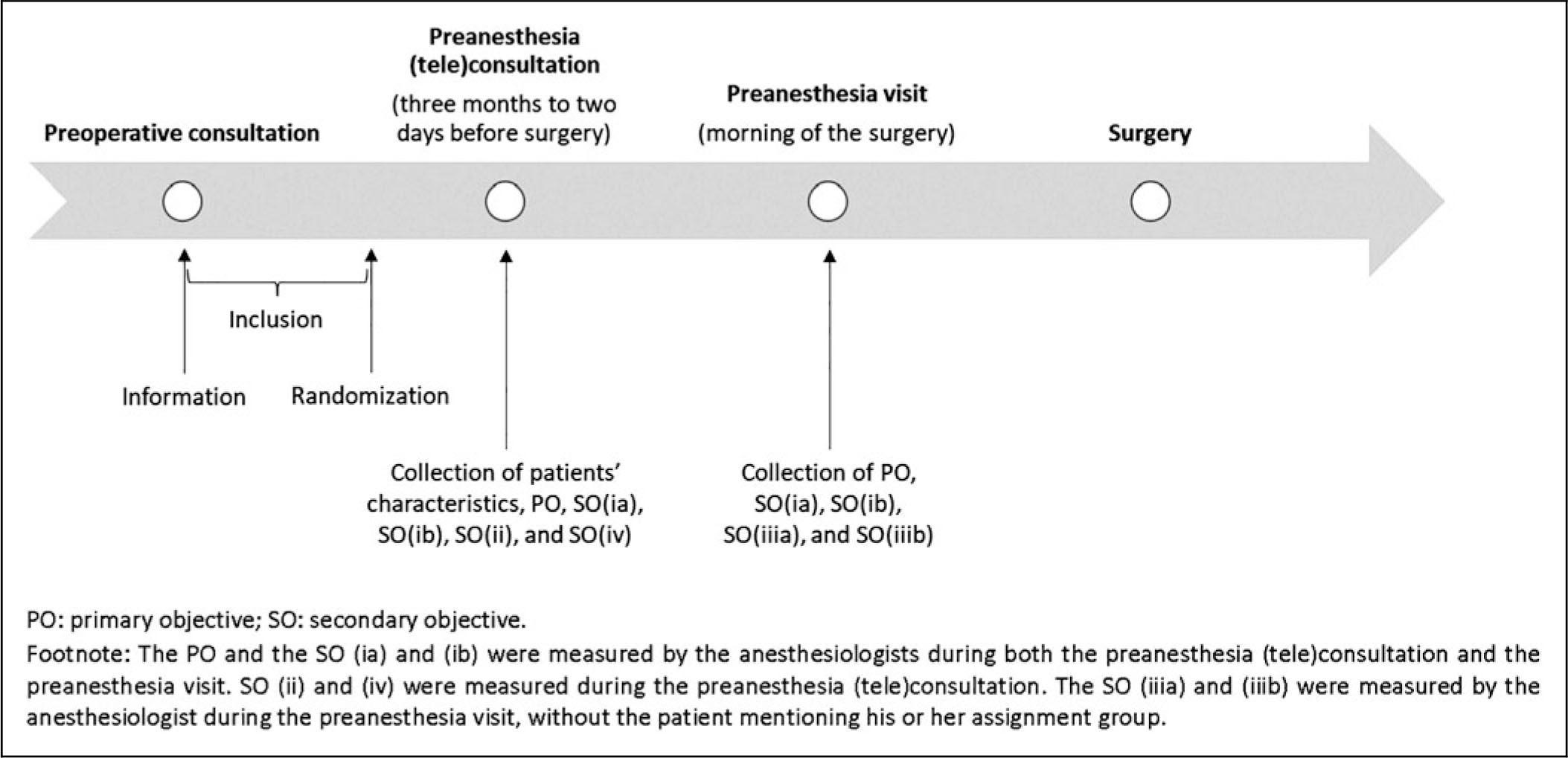
Description of the study process and outcome collection.
Randomization and masking
Eligible patients were randomly assigned in a 1:1 ratio to receive either a preanesthesia teleconsultation or an in-person consultation. The randomization was performed using a computer-generated allocation sequence, with permuted blocks of variable sizes. The group assignment was realized in a chronologic order after the signing of the consent form and during the booking of the appointment for the preanesthesia consultation by the anesthetic secretaries, who opened a sealed envelope that corresponded to the patient's inclusion number. Both the patient and the anesthesiologist who conducted the preanesthesia consultation knew the assigned group.
However, the outcomes (evaluation of intubation and ventilation difficulties, and ASA score) were assessed during the preanesthesia visit, which was performed by another anesthesiologist who was unaware of the group assignment, and medical records of the preanesthesia consultation were standardized and made similar between the two groups for blinded evaluation. Patients were asked not to specify the type of preanesthesia consultation to the anesthesiologist who conducted the preanesthesia visit.
Intervention
Patients who were assigned to the preanesthesia teleconsultation received this consultation in the form of a video conference with the anesthesiologist through the COVOTEM platform. The COVOTEM platform (COVALIA Interactive S.A.), is approved as a health data-hosting provider and guarantees the respect and protection of personal health data. Patients had to attend the teleconsultation in a quiet area, at home or at their workplace, that would allow confidential medical contact.
Before the preanesthesia teleconsultation, instructions for the video conference were given to the patients, and online technical assistance was offered (i.e., a website link to test their equipment). If the technical intervention was not successful, the preanesthesia teleconsultation was then cancelled, and an in-person consultation was scheduled. To measure the mouth opening and the thyromental distance during a teleconsultation, the anesthesiologist asked the patient to place his or her health insurance card next to his or her face in front of the camera. Knowing the standard length of a health insurance card, the anesthesiologist was then able to evaluate these parameters with sufficient accuracy.
For patients who were assigned to the in-person preanesthesia consultation, both the patient and the anesthesiologist were in a consultation room of the EGSC.
Outcomes and data collected
The primary outcome was the quality of intubation difficulty evaluation during the preanesthesia (tele)consultation.
The secondary outcomes were the following: - (ia) Quality of the mask ventilation difficulty evaluation during the preanesthesia (tele)consultation; - (ib) Good evaluation of the ASA score during the preanesthesia (tele)consultation; - (ii) Feasibility ratio of the preanesthesia teleconsultation; - (iiia) Patient's preoperative anxiety; - (iiib and iv) Patient's and anesthesiologist's satisfaction.
Figure 1 summarizes the outcome collection, and Table 1 describes details on each outcome.
Description of the Secondary Outcomes and Their Calculation
PO, primary outcome; SO, secondary outcome.
Statistical methods
The agreement on the predictable intubation difficulty between the preanesthesia consultation and visit was estimated to be 80% for the in-person consultation. We considered an equivalence of the two groups on this outcome if the agreement was between 72% and 88% for the teleconsultation. With an alpha error of 5% and 90% power, the sample size calculated was 107 patients per group. To consider potential loss to follow-up and withdrawal of consent, we planned to include 120 patients per group, that is, a total of 240 patients.
Categorical variables are described as numbers and percentages, and continuous variables as the means and standard deviations or medians and interquartile ranges (IQR), according to the distribution. We first compared baseline characteristics between the included patients and the patients excluded after randomization to ensure the absence of selection bias. Then, we presented baseline characteristics for the two groups to ensure their balance, without statistical comparisons according to the ICH E9 guidelines. 24
Agreement between the preanesthesia (tele)consultation and the preanesthesia visit of each item of predictable intubation difficulty, predictable mask ventilation difficulty, and ASA score were calculated for each group and compared between the two groups using chi-square tests. Patients' preoperative anxiety was compared between the two groups using the Wilcoxon test. The preoperative satisfaction of patients was categorized into three classes (0 to 6; 7 or 8; 9 or 10) and compared using a chi-square test. Main analyses were conducted following the intention-to-treat principle, that is, patients were analyzed in the group to which they were randomized (even if a switch to an in-person consultation occurred). Secondary per-protocol analyses were performed as sensitivity analyses, excluding patients for whom the teleconsultation failed. A p-value <0.05 was considered to indicate significance. All analyses were performed with SAS V.9.4 (SAS Institute, Cary, NC).
Results
Participant flow
Overall, 241 patients were included and randomized from June 12, 2018, to September 20, 2021. Thirty-three were excluded after randomization. Therefore, 208 patients were included in the intention-to-treat analyses: 96 in the teleconsultation group and 112 in the in-person consultation group (Fig. 2). Among the 96 patients from the teleconsultation group, teleconsultation failed for 12 of them who ultimately benefited from an in-person consultation. Six patients had a failure of the technical intervention offered before the teleconsultation (i.e., 90 of the 96 patients (93.8%) had a successful technical intervention), and six patients who had a successful technical intervention had a technical failure during the teleconsultation (i.e., 84 of the 90 patients who had a successful technical intervention (93.3%) had a successful teleconsultation). The feasibility ratio was then 87.5%. No serious adverse event was reported during the study.

Flow diagram of participants' inclusion, allocation, and data analysis.
Baseline characteristics
Among the 241 randomized patients, the baseline characteristics (i.e., age, sex, randomization group, surgery type, and medication intake) did not differ between patients included in the intention-to-treat analyses (N = 208) and patients excluded after randomization (N = 33).
Table 2 presents the characteristics of the 208 patients at the preanesthesia (tele)consultation. The two groups were broadly comparable at baseline, notably in terms of predictable intubation and mask ventilation difficulties and ASA score.
Demographic, Clinical, and Therapeutic Characteristics of Patients Attending the Preanesthesia (tele)Consultation (N = 208)
Results are presented as the means (standard deviations) or numbers (percentages).
Orthopedic surgery: knee arthroscopy, shoulder arthroscopy, ankle surgery, forefoot surgery, material removal, other.
Hand surgery: wrist arthroscopy, carpal tunnel, Dupuytren contracture, cystectomy, material removal, benign tumor resection, other.
ASA score, score of the American Society of Anesthesiologists; BMI, body mass index.
Quality of the preanesthesia (tele)consultation on the evaluation of predictable intubation difficulty
Table 3 presents descriptive results for the agreement on items of predictable intubation difficulty between the preanesthesia (tele)consultation and the visit for both groups. Disagreements in the number of item(s) of predictable intubation difficulty identified (n = 23) and/or in the type of item(s) (n = 5) identified were observed.
Description of the Agreement on Items of Predictable Intubation Difficulty Between the Preanesthesia (tele)Consultation and the Preanesthesia Visit in the Two Groups (N = 208)
The results are presented as numbers (percentages).
Agreements on items of predictable intubation difficulty did not differ (p = 0.23) between the two groups: 83.9% (94 patients) in the in-person preanesthesia consultation group versus 89.6% (86 patients) in the preanesthesia teleconsultation group (Table 4).
Comparison of the Agreement on Items of Predictable Intubation Difficulty, Predictable Mask Ventilation Difficulty, and ASA Score Between the Preanesthesia (tele)Consultation and the Preanesthesia Visit Between the Two Groups
The results are presented as numbers (percentages).
Quality of the preanesthesia (tele)consultation on other clinical parameters evaluations
Agreements on predictable mask ventilation difficulty (presence of ≥2 items) and ASA score did not differ between the two groups (p = 0.29 and 0.06, respectively) (Table 4).
Preoperative satisfaction and anxiety of patients
Figure 3 presents the patients' satisfaction for both groups. The preoperative satisfaction of patients was higher in the preanesthesia teleconsultation group (p = 0.04). Table 5 presents the preoperative anxiety of patients for both groups. It was adapted to the situation (i.e., APAIS global score <11) and did not differ between the two groups (p = 0.90).
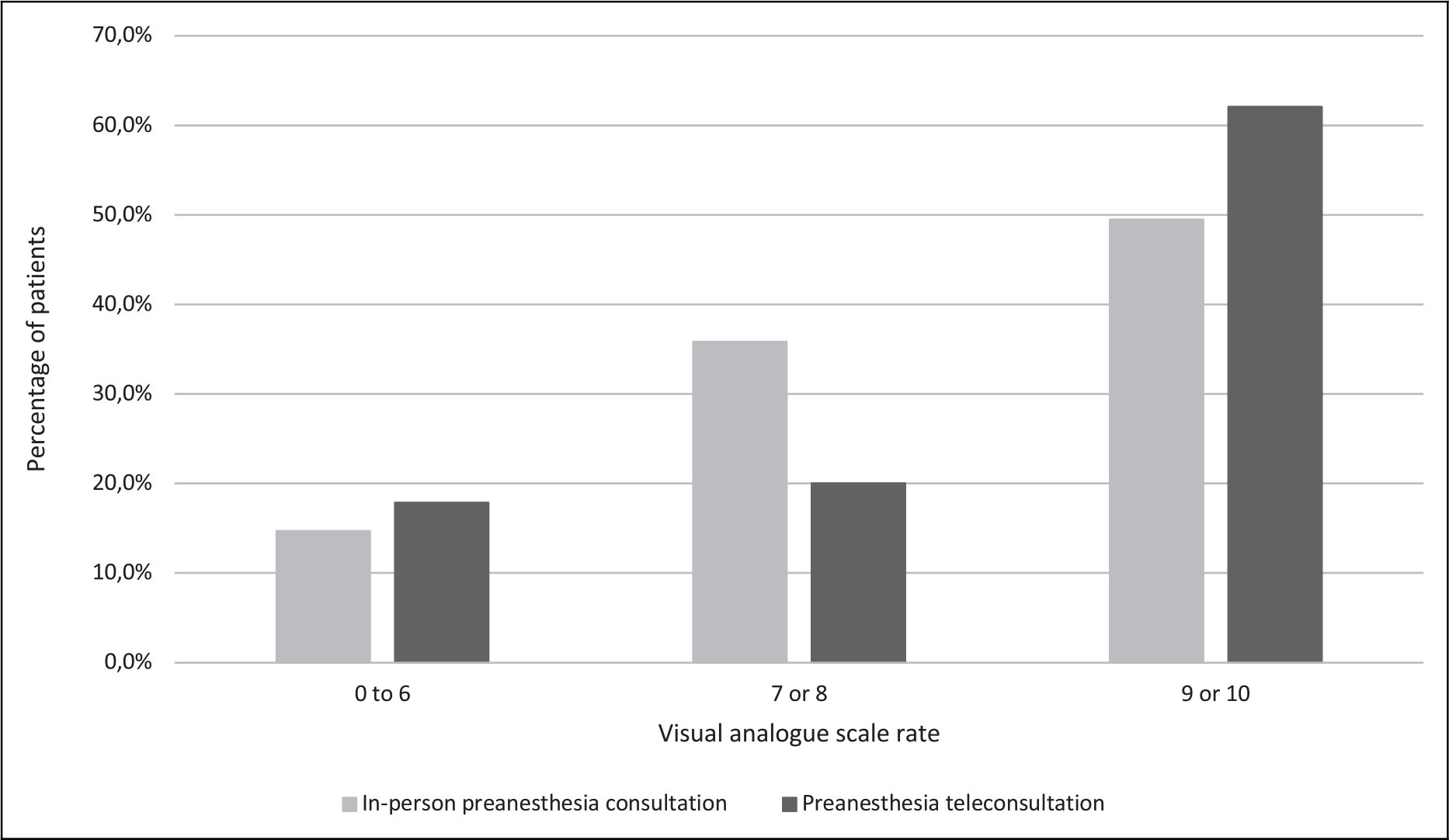
Comparison of patients' preoperative satisfaction between the two groups.
Comparison of Patients' Preoperative Anxiety Between the Two Groups
Results are presented as median and interquartile range in parenthesis.
Satisfaction of the anesthesiologists who conducted the teleconsultation
The median satisfaction of the anesthesiologists who conducted the teleconsultation was 10 out of 10 (IQR: 8.0; 10.0), even though we assigned a satisfaction rate of zero to anesthesiologists who held an unsuccessful teleconsultation.
Sensitivity analyses
The per-protocol analyses showed essentially the same results as the intention-to-treat analyses regarding the characteristics of patients in both groups and the agreements between the preanesthesia (tele)consultation and the visit on items of predictable intubation difficulty (83.9% vs. 88.1%, p = 0.41), predictable mask ventilation difficulty (82.1% vs. 89.3%%, p = 0.16), and ASA scores (100.0% vs. 96.4%, p = 0.08). The patient satisfaction was also higher in the preanesthesia teleconsultation group (p = 0.009), and patient anxiety did not differ between the two groups (p = 0.97).
Discussion
Main results
The TELECAM study aimed to compare the quality of preanesthesia teleconsultations and in-person consultations on clinical parameters evaluation. The results did not show any difference in the quality of the evaluation of predictable intubation, mask ventilation difficulties, and ASA score (p = 0.23, 0.29, and 0.06 respectively) between the two types of consultations. Regarding the patients' anxiety, our hypothesis was that teleconsultation could have increased it, as the consultation is remotely conducted, without a physical examination and face-to-face contact with the anesthesiologist.
However, our results were positive as we did not show any difference in the patients' anxiety, neither related to the anesthesia nor the surgery, between the two groups (p = 0.90). The preoperative satisfaction was higher for patients who had a teleconsultation (p = 0.04) and the satisfaction of the anesthesiologists who conducted the teleconsultation reached a maximum of 10. Finally, the feasibility of the preanesthesia teleconsultation was high, with a feasibility ratio of 87.5%.
Performance of the study
The TELECAM study was conducted between June 2018 and September 2021 and has since been impacted by the COVID-19 pandemic. Several patients were excluded after randomization (33 patients, 13.7%), mostly related to the COVID-19 pandemic (withdrawal of consent or cancellation of surgery). However, the pandemic also had a positive impact. Before the pandemic, physicians were reluctant to include patients because they were concerned about the quality of remote consultation. At the beginning of the study, only two preanesthesia teleconsultations per week were conducted, and by only two practitioners. COVID-19 forced physicians to modify their practices and has accelerated the implementation of telemedicine to prevent transmission of the virus. It resulted in an improved acceptability of preanesthesia teleconsultation by physicians and therefore an increase in inclusion in the TELECAM study. As a result, at the end of the study, all EGSC practitioners performed teleconsultations, and ∼15 preanesthesia teleconsultations per week were conducted.
Comparison with the literature
As mentioned, only a few studies aimed at evaluating the quality of preanesthesia teleconsultation on the evaluation of clinical parameters, only one on predictable endotracheal intubation difficulty, and none on predictable mask ventilation difficulty was found. Our results are in line with the study by Applegate et al., which revealed an equivalent prediction of difficult airway management between telemedicine and in-person preanesthesia evaluations. 20 We also found that the patients' preoperative anxiety did not differ between the two types of consultation, which is consistent with the Gibas et al. study conducted in 130 patients. 17 The very high satisfaction of patients undergoing teleconsultation had also been shown in many previous studies with satisfaction scores higher than 95%. 11,14,16,21
Satisfaction of the anesthesiologists was also high, as in Kern et al.'s study, which resulted in a 91% rate of anesthesiologist satisfaction with the medical aspects and a 64% rate of satisfaction with the technical aspects of the teleconsultation. 16 Regarding feasibility, we obtained a feasibility ratio of 87.5%, which is concordant with other studies: Kern et al. showed an 82% rate of successful anesthesia teleconsultations (failure was mostly caused by technical issues), 16 and Le Saché et al. showed that 90% of patients had successful teleconsultations. 11
Implications
Preanesthesia teleconsultation might result in an important reduction in constraints (reduced travel and wait time) and financial costs for patients, 5,12,21,25,26 while the quality of clinical parameters' evaluation is maintained and the satisfaction of both patients and anesthesiologists is high. These benefits are especially important for patients who are geographically distant from the consultation center, as these individuals could avoid days taken off work, travel time and costs, and parking fees.
Teleconsultation also resulted in a positive impact on public health, with a reduction in financial costs related to preanesthesia in-person consultation management. Moreover, the reduction in patients' travel distance has been shown to have a positive impact on the environment by reducing CO2 emissions. 26
Overall, 13% of patients faced technical issues as they did not have adequate home equipment or good enough internet access for teleconsultation. Huge technological progress has been made since the TELECAM study (conducted between 2018 and 2021), greatly improving the internet connection throughout the national territory and the quality of sound and image of videoconferences, so we believe that this proportion is decreasing over time. Otherwise, teleconsultation booths have been developed in France since 2021 (e.g., in pharmacies, medical centers, city halls) to make up for difficulties in accessing health care. 27
This might be an alternative for patients who do not have adequate home equipment, as these teleconsultation booths are fitted out with high-performance information technology equipment and are well implemented throughout the territory (especially in rural areas), and then should be easily accessible for all patients. Moreover, these booths integrate several measuring devices (e.g., thermometer, stethoscope, blood pressure monitor, oximeter) allowing to perform a cardiopulmonary auscultation during the preanesthesia teleconsultation.
Strengths and limitations
To the best of our knowledge, the TELECAM trial is the first French randomized controlled study evaluating the quality of preanesthesia teleconsultation compared with traditional in-person consultation on the evaluation of multiple blinded-assessed clinical parameters. Thus, it is in line with the model for assessment of telemedicine applications (MAST), which recommends assessing telemedicine using multiple outcomes. 28 However, our study has some limitations. First, the percentage of patients excluded after randomization was not negligible and was slightly higher in the teleconsultation group (17% vs. 11%). However, all the reasons for exclusion were collected, and most of them were related to the COVID-19 pandemic. Moreover, a selection bias is unlikely, as the characteristics did not differ between patients included in the analyses and patients excluded after randomization.
Second, in view of the very low number of patients with predictable intubation difficulty, we could not use the initially planned primary outcome of the agreement on predictable intubation difficulty between the preanesthesia (tele)consultation and visit. We then modified a posteriori this outcome to the agreement on each of the four items defining intubation difficulty between the (tele)consultation and visit. Finally, one must be cautious about the generalization of our results to all preanesthesia consultations, considering that (1) TELECAM was a single-center study conducted in France, with the national specificities and constraints of the preanesthesia evaluation; and (2) it only focused on low-risk ambulatory orthopedic and hand surgeries. Actually, these results are probably not applicable to high-risk surgeries (e.g., complex nonambulatory surgeries) and/or high-risk patients (e.g., with multiple comorbidities) and studies are needed to confirm the safety of preanesthesia teleconsultations for such situations before being implemented in current practice.
Conclusion
The TELECAM randomized controlled study showed positive results for the quality of preanesthesia teleconsultation on the evaluation of clinical parameters at risk for anesthesia, for patients with a scheduled ambulatory orthopedic or hand surgery. The feasibility of teleconsultation and the satisfaction of both the patients and the anesthesiologists were high, with no increase of patients' anxiety. These results should encourage the use of teleconsultation, which is promoted in the French “Health Innovation 2030” plan. 29
Footnotes
Acknowledgments
We thank the patients who participated in the TELECAM trial as well as the TELECAM investigators (Dr. De Almeida, Dr. Calafat, Pr. Dautel, Dr. Gervais, Dr. Mekler, and Dr. Roche), and the Nancy DRCI team [Yohann Bernard, Valérie Bouaziz, Asma Cherifi, Charlotte Daguin, Nadine Petitpain, Véronique Saunier, El Mehdi Siaghy (Director)), and Corinne Roldo (Strategy department)] for their devotion to (team) work.
Authors' Contribution
Conceptualization: H.B., N.T., M.P., A.R., and F.S.; Methodology: N.T., H.B., and A.R.; Project administration: A.R. and H.B.; Formal analysis and software: I.A., M.D., M.S., and N.T.; Writing – original draft: A.R., M.S., and N.T.; Writing – review and editing: H.B., M.P., F.S., I.A., and M.D.
Disclosure Statement
The authors have no conflict of interest to declare.
Funding Information
This study was supported by internal funding from the University Hospital of Nancy. The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.