
Abstract
Introduction:
The significance of comprehensive investigations specifically addressing the characteristics and implications of nervous system injuries (NSIs) and particularly war-related spinal cord injuries (SCI) remain limited. Iraq lacks comprehensive survey studies for quality of life for people after SCI. The objective of this work was to identify the number of NSIs and mortality of those injured during the Islamic State of Iraq and Syria (ISIS) war in Iraq and analyze events specifically as sociodemographic variables to assess quality of life healthy, psychological, and social disorders from onset of injury till the involving.
Methods:
A survey-based descriptive study, and analytical retrospective at community-based of Nineveh Governorate, in Iraq. The participants were 34 survivors of ISIS war with SCIs, ages between 9 and 60 years, and 7 females (20.59%) and 27 males (79.41%) as registered in Nineveh Center of Disability Rehabilitation. Data collection was conducted using Telephone Video Interviews and respondents' health information. Protocol-specific questions and some psychological and social scales (PTSD) (DSM-IV), (TAS-20), (SWLS), and (MSPSS) were also used.
Results:
There were 2,990 NSIs with the highest rate of injuries occurring from 2017 to 2018, and the SCIs were 267 injuries (8.93%), and (70.59%) at level T the mortalities were 57 cases, all participants suffered from physical and psychological chronic complications, while the results of the PTSD, GPC, and SWLS were at a moderate level.
Conclusions:
In urban warfare, there's a rise in NSIs, notably SCIs influenced by the type of weaponry. The survivors face significant physical, psychological, social, and financial burdens. More research is crucial to understanding their situations and developing strategies to alleviate their health, social, and financial challenges.
Introduction
Wars throughout history have caused numerous victims and injuries. The recent war in Ukraine has reported a 22% prevalence of spinal cord injuries (SCI). 1 This trauma results in neurological and motor impairments, potential organ failure. 2 In addition, SCI leads to significant physical, psychological, and social complications. 3 Intensive medical care, including rehabilitation, is crucial for addressing the chronic of this injury. 4 Also, it is the importance of monitoring SCI survivors' emotional well-being. 5 Kang et al. emphasized the importance of understanding regional epidemiology to implement effective preventative measures tailored to the specific population's circumstances. 6
Iraq faced a notable occurrence of nervous system injuries (NSIs), with SCIs being particularly prevalent, largely attributed to the consequences of war. In Mosul, which was a theater of war, the health care system was ill-equipped to handle a significant rise in NSIs, especially SCIs, according to health care officials in the city. Therefore, the majority of these injuries initially received treatment in regions unaffected by conflict but operating in conditions influenced by war. Limited essential resources and infrastructure pose challenges, exacerbated by the destruction of major city hospitals during the conflict. As a result, rehabilitation services have taken a backseat compared to other health care provisions. In the middle of these challenges, imposed by the war and available medical capacities, there has been an exacerbation of complications for the affected individuals.
Moreover, rehabilitation efforts prewar in Mosul exhibit minimal priority within the health care administration were often marginalized. This led people with SCIs and their families a feeling of despair regarding their rehabilitation and return them to life with highly independent. Consequently, the present study evaluates the quality of life by telehealth approach by using a tele-assessment which offered remote assessment for these affected individuals. 7 In addition, the study reviewed assembled comprehensive data regarding NSIs, specifically SCIs, among the impacted population during the wartime period, and to shed light on their physical, psychological, and social well-being.
Synchronously, the study procedures began during the COVID-19 pandemic and the implementation of lockdown and social distancing measures, choosing a remote survey evaluation proved highly suitable for fulfilling the study's objectives. Haleem et al. found that telemedicine technologies provides a safe choice for patients who cannot go to the doctor or sit at home, especially during a pandemic. 8 Studies conducted by Yuen et al. and Lai et al. show that telemedicine plays a crucial role in managing SCI patients, especially in situations that hinder access to rehabilitation and integration into society. 7,9
Unfortunately, it is proven through tele-investigative survey a significant proportion of the casualties that comprised individuals, who residing in economically disadvantaged regions, lacked the means to access medical and rehabilitative care either within domestic private health care institutions or abroad. However, it is clear that both the acute and long-term phases of care for SCI are accompanied by life-threatening consequences. 10 Also, upon thorough investigation, no research interest or studies pertaining to the conditions of survivors of the recent ISIS war in Mosul, especially those with SCI, were found in locally and internationally published research article.
Therefore, this study seeks to share the results with relevant institutions to address the health complications, economic, and social consequences of war-related injuries on both victims and their families in future studies. Identifying injured individuals and understanding their circumstances will also help propose solutions to improve the overall well-being of victims. 11 Also, the study highlights the consequences of injuries, providing a comprehensive understanding of the impact of war-related injuries, 12 because the likelihood of challenges is positively correlated with the seriousness of the damage. 13
Methods
Study design
A survey, analytical, and descriptive design comprehensive investigation was undertaken utilizing a quantitative, analytical, and descriptive of quality-of-life retrospective approach through survey administration. The study was executed within community-based contexts spanning the geographical areas of Nineveh, Erbil, and Duhok.
Ethical considerations
Official ethical approvals were received from the University of Mosul to the Nineveh Health Directorate (NHD). The official approval was necessary for obtaining access to the individual's medical records database, registered in the IT department as war victims at Nineveh Center for Rehabilitation Disability People (NCRDP). Oral information regarding the study's objectives and advantages of participation was provided to all individuals who were contacted during the telephone interview. The research committee of training and development center approved the study protocol (Decision No. 80/21 in 23/6/2021).
Data collection
Data were collected, managed, and stored, and confidentiality was maintained during the collection and storage of the data. The study was conducted as a retrospective study 3 years after the war ended. This study investigated NSIs during 2015–2020 in the regions of Nineveh, Erbil, and Duhok, with Nineveh being the location of the war and Erbil and Duhok serving as reception centers for war victims. Access to the medical records, specifically (7,902) NSIs and (856) of them was SCIs as documented in medical discharge records was granted. Collaborating with governmental emergency hospitals, NSIs departments, and neurosurgery departments that predominantly managed cases during the period 2015–2020 according to Iraqi health system for management NSIs. Data concerning injuries and fatalities were compiled during the period 2017–2018.
This effort involved governmental coordination encompassing first aid units and diverse military sectors across the Nineveh, Duhok, and Erbil Governorates within the Kurdistan Region. Notably, certain humanitarian and international medical organizations, such as Doctors Without Borders, extended their assistance in initial medical and primary care capacities. However, these organizations were not incorporated into the present survey study. The majority of cases were subsequently documented within specialized medical committees dedicated to victims of terrorism at NCRDP, which constituted a significant data source for this survey study.
Regarding collecting information about SCIs, the main author sequentially contacted participants securing their voluntary consent by depending on a tele-assessment and tele-investigation approach, the survey initial phase was started. It involved gathering information about the injury, including type, degree, first aid, medical treatment, and rehabilitation, using a preprepared form. In a subsequent tele-call, psychological and social information was collected, using appropriate measures for individuals with SCIs. It should be noted, that all of these measures were taken under the conditions of closure imposed due to the outbreak of the COVID-19 Pandemic.
Participants
Official approval was necessary for obtaining access to all medical records of war victims at the NCRDP and with the help of social researcher, the author interviewer successfully contacted study participants by cell phone and WhatsApp video call. However, some participants phone numbers were not operational, therefore, the author was able to reach only 34 victims out of a total of 54, the females were 7 and 27 were males. Unfortunately, two cases who the corresponding author contacted died due to the complications of injury and also due to the neglect of rehabilitation in the previous 2 years.
Moreover, as a previous procedure of contact with participants, the center posted an announcement about the study on its official Facebook page informing victims about the study and stating that they would be contacted soon by a researcher to explain the study and invite them to participate voluntarily.
The oral information regarding the study's objectives, and advantages of participation, was provided to all individuals whom the authors were able to contact by telephone interview. During the sequential contacts with participants, they willingly consented to participate in the study.
Outcomes
The authors used a tele-investigation by telephone interviews to assess the physical complications, psychological, and social conditions of victims within 1–3 months after their injuries. Questionnaires and psychosocial scales were used in the evaluation. They identified 54 patients with traumatic SCIs who registered among ISIS victims. The authors conducted two-stage interviews via mobile phones. The first stage involved a customized questionnaire with 44 questions covering some characteristic of patients to assess and detect the body composition changes, injury details, circumstances, first-aid, medical treatment, rehabilitation, complications, and financial support, as is illustrated in Figure 1. The second stage included measurements of general psychological consensus (GPC) 14 ; post-traumatic stress disorders (PTSD) according to (DSM-IV) 15 ; satisfaction with life scale (SWLS) 16 ; and multidimensional scale of perceived social support (MSPSS) (Family, Friends, and Others). 5 These telephone video-call interviews were conducted during the COVID-19 pandemic.
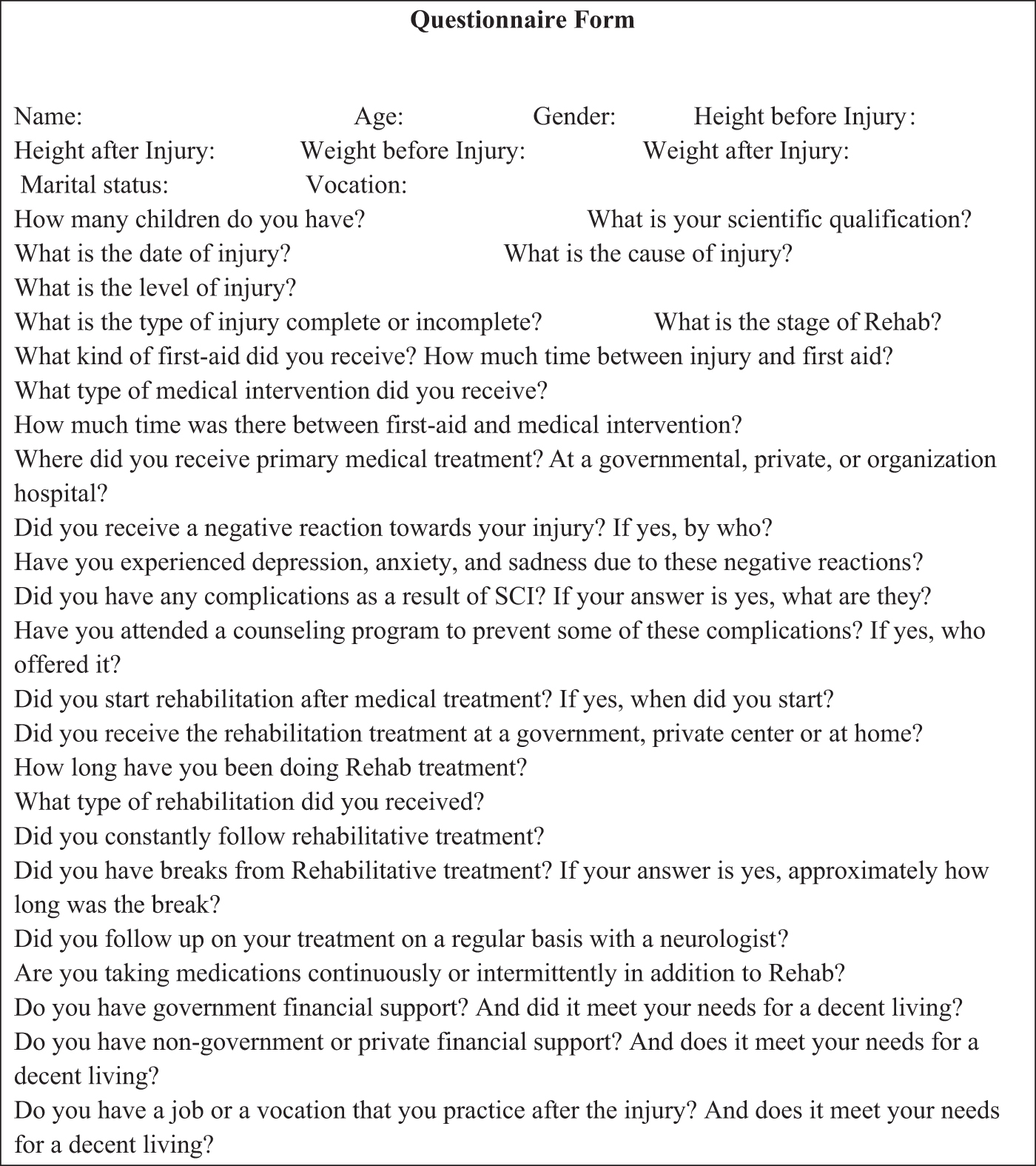
The questionnaire from which to identify some personal information, health, psychological, social, and economic conditions.
Statistical analysis
All statistical tests were processed using STATISTICA Software. (IBM-SPSS statistics processor version 24) for data analysis. The authors used mean (average) and standard deviation (SD) values for each variable. In addition, the authors used the ratio percentage (RP) and independent-samples t-test according to an alpha (≤0.05) was considered statistically significant. According to Statistical Power Analysis for the Behavioural Sciences Hoboken: Taylor and Francis. 17,18
Results
Table 1 presents a comprehensive overview of NSIs and a comparative analysis with the periods before and following the war, spanning from 2015 to 2020. The comparison encompasses the incidence of NSIs, their causal factors, and the fatalities stemming from related complications. The study findings indicate that a majority of head and spinal injuries before and after the war were primarily linked to road traffic accidents, followed by falls from heights, and violence as the third leading cause of injury. Notably, significant disparities in SCI occurrence were observed during the war years in contrast to the periods before and after the conflict spanning from 2015 to 2020. These disparities are visually represented in Figure 2. A detailed analysis of injury records related to NSIs underscores that a total of 2,990 injuries occurred during the war compared, with 2,811 injuries before and 2,101 injuries after.
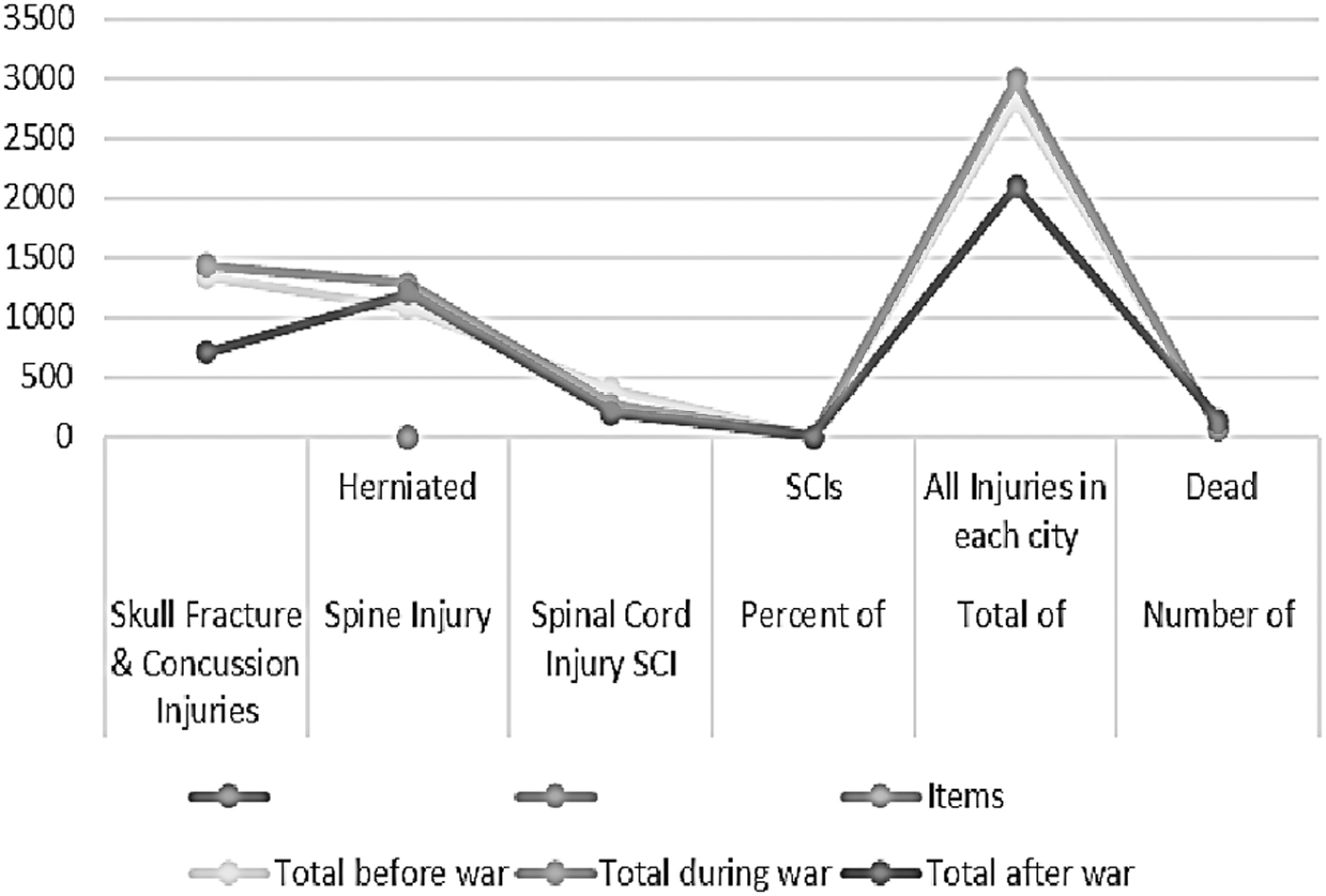
It shows the total scores of NSIs and the mortality as a resulting of these injuries (before war 2015 and 2016, during war 2017 and 2018, and after war 2019 and 2020) in three cities, at Nineveh, Duhok, and Erbil governorates, of this study. N = Number of participants, ± SD = Standard deviation.
The Numerical Data for Head Injury (Skull Fracture Injuries & Concussion); Spine Injury (Herniated Disc); Spinal Cord Injuries, the Percentage of Spinal Cord Injuries from Total Injuries in Each Year, the Mortality as a Resulting of These Injuries (2015, 2016, 2017, 2018, 2019, and 2020), at Nineveh, Duhok, and Erbil Governorates
N, Nineveh; D, Duhok; E, Erbil.
Figure 2 presents the differences of total NSIs among before, after, and during the war. Moreover, geographical distribution revealed the highest number of injuries, which were received in the city of Duhok. The injury statistics also encompassed 1,435 instances of head injuries inclusive of skull fractures and concussions, along with 1,288 cases of spinal injuries, including instances of herniated discs. This information is based on meticulous medical record-keeping, with patients being categorized within specialized neurosurgery departments based on their specific injuries. In addition, the research findings indicated that there were 57 fatalities which represented 27.14% of the total deaths before and after the war, which were 210 fatalities. These deaths attributable to complications arising from NSIs and most of them were due to head injuries.
Table 2 shows results of the questionnaire's answers that characteristics information and quality of life of the survivors, including their marital status and educational background. Less than half of the survivors were married, and a proportion of them had young children. The majority of the sample had no academic qualifications. In terms of injury level, over two-thirds of the participants had level T injuries, 41.18% in the lower part of the T level, and 29.41% at the upper part. A smaller number of individuals had injuries at level L (20.59%), and the least number of injuries were at level C (8.82%). Four (11.76%) patients were with incomplete spinal cord damage and 30 (88.23%) patients were with complete damage according to ASIA-scale test.
The Participants' Answers on the Questionnaire About Injuries, Complications, and Quality of Life from the Time Immediately After the Injury to the Time of Conducting the Interview with Participants
P, People.
Some participants were still in the sitting stage, with some experiencing an unbalanced sitting position due to neglected rehabilitation. A few individuals were able to reach the standing and walking stages with the assistance of devices. Attributed to their commitment to rehabilitation.
The study revealed that some victims encountered negative reactions from physicians and neurologists, which led to psychological depression and hindered their progress in rehabilitation. Rehabilitation varied in terms of duration and initiation time, with participants receiving rehabilitation in both private and government centers and some of them at their home. Only 22 participants were committed to rehabilitation for less than 1 year. The periods of commitment to rehabilitation varied, with little individuals underwent rehabilitation between 13 and 48 months. A majority of participants (28 individuals) reported improved general health conditions after rehabilitation, while 6 individuals did not benefit from rehabilitation due to irregular periods.
Related with type of rehabilitation intervention, 4 individuals were conducted epidural spinal cord stimulation and then exercises, and 3 individuals were conducted galvanic muscular stimulation and exercises for lower limbs, while 27 individuals were only given exercises and massage. Sixteen participants did not have periodic follow-ups with neurologists, while 18 individuals did have follow-ups. Despite rehabilitation efforts, all participants experienced complications, with 29 individuals suffering from bedsores and some of them are suffering till now. All participants were experiencing renal-tract and bladder infections. These findings highlight the challenges faced by survivors, including limited access to rehabilitation, psychological distress, and ongoing health complications.
All individuals in the sample were taking antibiotics regularly, and a portion of them used tonic drugs, analgesics, and muscle relaxants. In terms of financial support, approximately half of the participants received a monthly salary from the government, with varying times of receipt. Moreover, more than half of the participants did not receive any private financial support. However, nearly half of the injured individuals received financial support from their families.
Table 3 shows the psychosocial scales and presents the mean and standard deviation scores for PTSD, GPC, SWLS, MSPSS, and the weight before and after (4–5 years) the injury for both females and males. Regarding PTSD, females (N = 7) represented 20.59% (41 ± 6.03), and males (N = 27) represented 79.41% (29.81 ± 9.85). Also, the t-test revealed a significant difference between male and female, t(2.851) = 32, p < 0.008, the effect size is large (Cohen1's d = 1.22), and it is indicated that the females suffered from PTSD more than the males. In the GPC, the mean score for females was 25.28 ± 5.65 and for males it was 23.33 ± 6.39,
Differences of Psychosocial Scales and Weight Between Male (N = 27, 79.41%) and Female (N = 7, 20.59%)
N, Number of participants; M, Mean; SD, Standard deviation; t, t-test value; P , Alpha-beta value; Cohen's d, Standardized effect size for measuring the difference between means; PTSD, post-traumatic stress disorders; GPC, general psychological consensus; SWLS, satisfaction with life scale; MSPSS, multidimensional scale of perceived social support.
The t-test revealed no significant difference between male and female, t(1.139) = 32, p < 0.263, the effect size is medium (Cohen1's d = 0.48). For SWLS, the mean score for females is 14.28 ± 7.11; and for males, it is 17.59 ± 5.72. The t-test revealed no significant difference between male and female t(−1.129) = 32, p < 0.898, the effect size is very small (Cohen1's d = 0.06). Regarding MSPSS, which has three sources (family, friends, and others), the mean score for females in the family source was 22 ± 4.72, and for males, it was 22.55 ± 4.67. In the friends' source, the mean for females was 7.57 ± 6.12 and for males, it was 14.48 ± 6.82. In the “others” source, the mean for females was 20.86 ± 5.58 and for males, it was 21.7 ± 5.45.
The t-test revealed no significant difference between male and female in family source, t(0.111) = 32, p < 0.912, the effect size is very small (Cohen1's d = 0.05) and in others source t(0.333) = 32, < 0.7141, the effect size is small (Cohen1's d = 0.15). While the t-test revealed a significant difference between male and female in friend source t(2.435) = 32, p < 0.021, the effect size is large (Cohen1's d = 1.04), it is indicated that the friends source as a social support was a weak for female than male (Fig. 3). In the weight measures, the mean before injury for male was 65.73 ± 16.43, and for female, it was 60.57 ± 15.20, while the mean after 4–5 years of injury became 65.43 ± 12.64 for male and became 61.36 ± 12.47 for female.
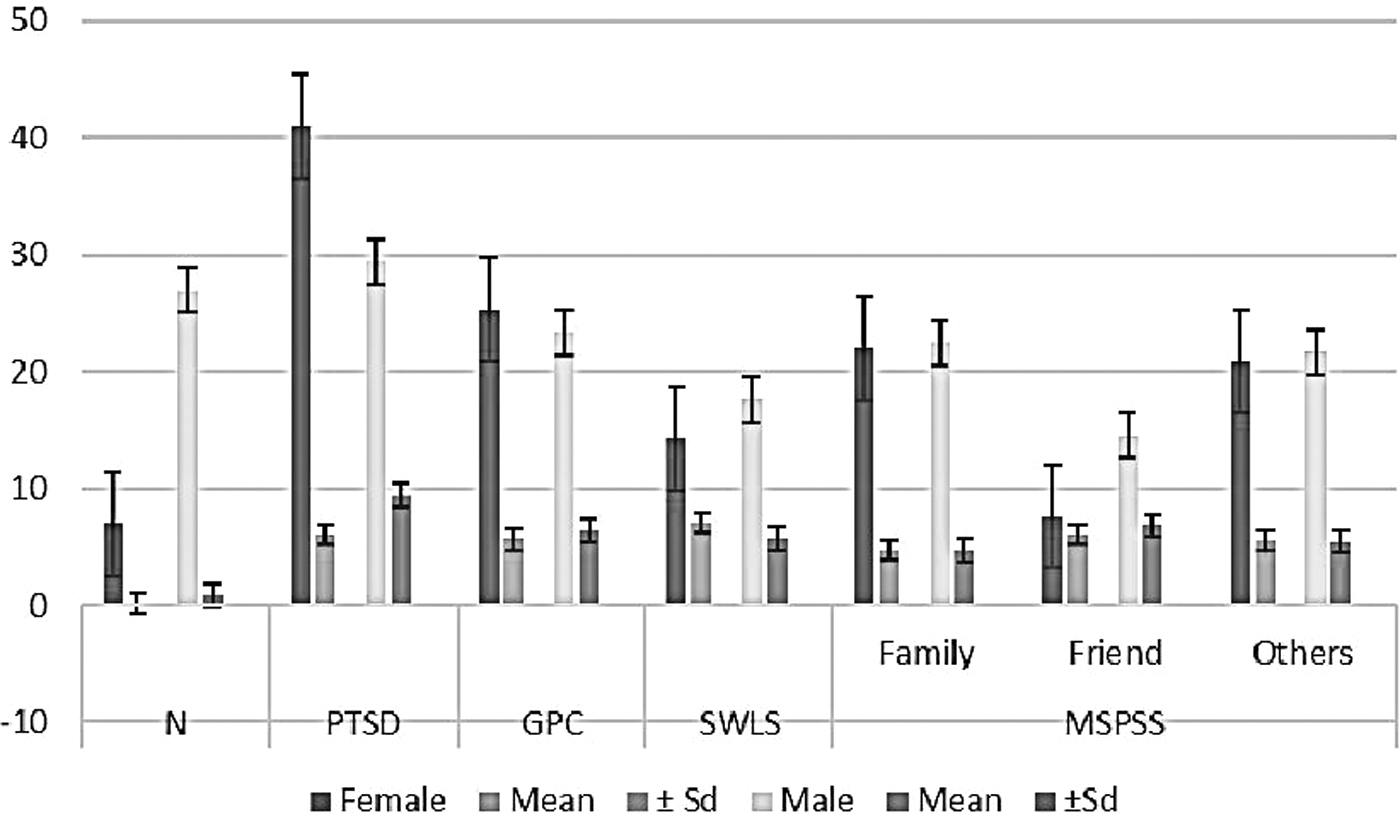
It shows the mean and standard deviation scores of the psychological and social scales injury for male and female participants in this study. N, Number of participants; ± SD, Standard deviation; PTSD, post-traumatic stress disorders; GPC, general psychological consensus; SWLS, satisfaction with life scale; MSPSS, multidimensional scale of perceived social support.
The t-test revealed no significant difference between male and female in weight before injury, t(0.747) = 32, p < 0.461, the effect size is small (Cohen1's d = 0.32). Also, no significant difference in weight between male and female after injury, t(0.761) = 32, p < 0.452, the effect size is small (Cohen1's d = 0.32).
Discussion
According to the study aims, NSIs and highlighted SCIs were documented among victims of wartime conflicts. These injuries were attributed to the destructive effects of war, such as explosions, missile impacts, and sniper attacks, with a focus on the years 2017–2018 during the ISIS conflict. The findings align with previous research conducted on war veterans and civilian victims, 19 such as those in Palestine's Gaza City, 20 which also explored mental health, social environment, and the nature and severity of psychological traumas. Autopsy investigations of civilian victims who suffered gunshot wounds supported these findings indicating that spinal injuries were prevalent. 21 The results of previous studies emphasize the evidence of prevalent SCIs in victims of ISIS in Iraq, because these groups used this tactic extensively.
In addition, it was observed that both battle and nonbattle-related spine traumas in military conflicts resemble severe SCIs resulting from polytrauma in civilian populations. 22 Also, Blair et al. concluded that the modern combat has witnessed an increase in spinal trauma, 23 and also the specific characteristics of urban warfare and modern combat strategies used during the war have increased the trauma.
Notably, the variation in injury prevalence across different spinal levels is evident, with injuries at the dorsal level representing the predominant majority, surpassing (70%) of the total injuries. Scholars elucidate this trend by attributing it to civilians' lack of familiarity with safeguarding themselves against sniper and explosive threats, particularly when using tactics of infiltration and concealment during their attempts to escape conflict zones. In addition, civilians lack the protective barriers commonly used to shield the torso.
Furthermore, these anatomical regions assume a salient configuration, featuring a wide and flat surface that renders them susceptible to projectiles discharged by snipers and fragments emanating from explosive detonations. 24 These dynamics were notably exemplified through the level and type of SCIs during the ISIS war.
Schoenfeld et al. found in their study that war in densely populated urban areas with unarmed civilians often leads to SCIs. 25 The war against ISIS in Iraq involved the use of civilians as human shields and improvised explosive devices, resulting in various craniospinal damages during the conflict. 24 Güzelküçük et al. a recent longitudinal investigation highlighted differences between SCIs caused by service bullets and civilian-inflicted ones, particularly in terms of the affected population, lesion types, and the degree of SCI caused by gunshots. 26 In addition, Blair et al. found that TSCIs in civilians may resemble conflict-related TSCIs. 27 Regarding the greater number of injuries for males compared to females, it agrees with study of Kang et al. who reported a higher number of male patients than females and common complications accompanying SCIs in different regions or countries. 6 Dryden et al. pointed out leading to persisting secondary complications long after the acute trauma SCIs. 28
Notably, in our work, we used a telephone call and video interview (Supplementary Video S1), we found that telehealth was an alternative and successful method to assess the participants from multiple aspects related to their health, psychological, social, and financial conditions. Our study results, in terms of the success of the tele-assessment approach and method, are consistent with the Sechrist et al. study that shows the feasibility and acceptance of a telemedicine intervention via iPad for individuals with SCI through positive. A Program Satisfaction Survey (PSS) rating and the wide variety of healthy clinical topics was addressed. 29
In a Phillips et al. study, preliminary evidence suggests that in-home telephone or video-based interventions do improve health-related outcomes for newly injured SCI patients, moreover may be cost-saving if program costs are more than offset by a reduction in rehospitalization costs, but differential advantages of video-based interventions versus telephone exist. 30 In addition, Van De Pol et al. concluded that the telehealth models of care promote better engagement with local health service providers (such as general practitioners, nurse practitioners, and allied health professionals) could improve equity of access and reduce the need for extensive travel. 31 The results show the dedication exhibited by certain participants toward rehabilitation and some of them treated with epidural stimulation which helped their progression to walking with assistive devices KAFO. Formento et al. concluded in their study that the epidural electric stimulator for spinal cord helps to reach the walking stage. 32
Regarding the victims' well-being and quality of life, all participants suffered from psychologically chronic complications, and in PTSD scale, the female suffered more than the male also in MSPSS in friends' sources, it was weak for female, the authors think the emotional and societal factors, including customs and traditions, significantly influence the characteristics of females in Mosul city, limiting social support specifically in friend sources. Also, the previous study emphasized that the familial dynamic plays a role in psychological distress, with boys and girls exhibiting different responses to war trauma. 33
However, the results showed the lack of support for females through the lower HRQOL as observed in individuals with cervical spinal lesions. Kanyoni et al. found that the gender was seen to significantly influence community reintegration with males being better prepared to resume normal roles and responsibilities in the community compared to females. 34 Similar results were reported by Whiteneck et al. and Buys et al., in which women experienced more environmental barriers; poor community reintegration because of unemployment among women with TSCI and also unmet community needs of women. 35,36
In terms of other measurements, both genders experience similar challenges, with minor differences that do not reach statistical significance. While the results of the PTSD, GPC, and SWLS were at a moderate level, the study correlates with findings from Ebrahimzadeh et al., Saadat et al., and Salter et al. 28,37,38 The prolonged SCIs from the Iran-Iraq war resulted in severe depression, negatively impacting subjective well-being, life satisfaction, and functional abilities. 39 Saadat et al. found that cervical spinal lesions among veterans also had a negative influence on mental and physical health-related quality of life (HRQOL). 28 Depressive disorders in individuals with SCIs pose a challenge as they affect self-reported well-being and daily functioning. 40 However, these challenges, while not always immediate, tend to manifest several months postinjury.
In our study, participants reported distressing encounters with medical professionals, particularly doctors and neurologists, shortly after sustaining injuries. These negative interactions had detrimental effects on their well-being and impeded their rehabilitation progress. Studies focusing on the psychological well-being of individuals with SCIs affirms that significant psychological challenges are commonly experienced following such injuries. 41 The study's results align with Adebusoye et al.'s recommendations, suggesting that war-torn countries with significant unmet needs in terms of traumatic SCIs should be given special consideration, underscoring the importance of conducting more comprehensive studies in such conflict zones. 42
In the context of health care in Iraq, according to results, there is some interest in providing primary health care for the injured, including rapid emergency medical interventions such as surgery operations, although these are often a very limited number and delayed in wartime conditions. However, acute care is compromised due to limited financial resources and the inability to accommodate a large number of injured individuals during conflict. Postacute rehabilitation care is notably inadequate and frequently overlooked.
Regrettably, during the tele-assessment in our study, we revealed that several participants reported that doctors had given them bleak prognoses, advising them to accept their fate. Ironically, many of these individuals demonstrated significant improvements, achieving high levels of independence, regaining mobility, driving, and successfully reintegrating into society. Unfortunuity, these findings do not align with the principles of advanced health care systems that prioritize patient psychological well-being and a compassionate approach. The authors recommend that concerned authorities provide support and address the basic needs of these individuals related to their injuries and associated complications. Overall, the authors emphasize the need for comprehensive studies focusing on the well-being of victims with SCIs, especially in conflict-affected regions.
Conclusion
The numbers of NSIs, including SCIs, have doubled due to tactics used by ISIS. The consequences of war extend beyond physical harm, leading to psychological, social, and financial challenges. Cultural and environmental factors, such as social cohesion, positively impact psychological well-being and life satisfaction. The findings align with prior research on the prevalence and long-term complications of SCIs. Prioritizing rehabilitation and participation through public policies is crucial for mitigating the health, social, and financial burdens faced by war victims. Further investigations are needed to fully understand the conditions of survivors, considering demographic similarities and differences.
Footnotes
Acknowledgments
The authors express gratitude to all contributors, including the Center of Scientific Research and Human Development at NHD, Duhok Health Directorate, and Erbil Health Directorate at Kurdistan Region. They appreciate the facilitation of access to records of the injured, particularly the IT department and social researcher in Nineveh Center Rehabilitation of Handicaps. Also, the authors appreciate the participants and their family's cooperation during the program implementation.
Authors' Contribution
The corresponding author M.F. formulated and developed the research goals and ideas. In addition, M.F. and W.M. provided oversight and leadership for the research activity planning and execution. M.F. conducted a research and investigation process, specifically the telephone interview with participants according to questionnaire form, data/evidence collection, and analyzed the study data. Moreover, he managed and coordinated responsibility for the research activity planning and execution. Further, he managed data and maintain it, and the financial support for the completion of the study was based on self-financing by the corresponding author, and no financial funding was obtained from any other party.
M.F., W.M., F.F., and S.K. are contributed in preparation of the published work, specifically critical review, commentary, or revision – including pre- or postpublication stages equally. In addition, they prepared the published work, specifically writing the initial draft (including substantive translation). M.F. coordinated appointments to telephone interviews for assessing the psychosocial measures. W.M. supervised on mentorship external and S.K. scientifically supervised the medical aspects of the article. To confirm this scientific achievement, the researchers sought to obtain ethical approvals from the government agencies responsible for managing medical research.
Disclosure Statement
All authors contributed to the article in varying proportion and they agree with the content. The authors declare no competing interests.
Funding Information
This work was not supported financially nor funding, and the authors did not use copyrighted material in preparing this work. Finally, as a requirement for this type of study in Iraq, the ethical approvals were previously obtained from the research and development committee in the Nineveh Directorate of General Health (NDOGH).
Supplementary Material
Supplementary Video S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.