
Abstract
Objective
: e-Health or web-based systems in the field of tinnitus have gained increasing interest. Cognitive behavioral therapy (CBT) delivered via the internet is currently witnessing a surge in both attention and offerings. This systematic review analyzed the efficacy and sustainability of internet-based therapies aimed at reducing tinnitus distress and comorbidities such as anxiety, depression, and sleep disorders. The review exclusively considered randomized controlled trials (RCTs) in which trained personnel were actively involved during intervention.
Methods
: Utilizing search terms such as tinnitus, internet-based therapy, and e-Health therapy, we identified 155 studies, from which 37 RCTs were carefully examined for data availability. Primary outcome measures included treatment effects for tinnitus distress (Tinnitus Questionnaire and other questionnaires) and handicap (Tinnitus Handicap Inventory), while secondary outcomes encompassed depression, anxiety, and sleep problems. Meta-analyses were conducted employing random-effect models. A study effect model was applied, yielding a singular effect size for each sample. The effect sizes were examined for influences of various moderators.
Results
: We found a statistically significant large effect size for improvement in tinnitus distress (d = 0.83; [confidence interval 0.61–1.06] with total n = 450 for the experimental group and total n = 504 or the controls), while the reduction of tinnitus handicap was smaller (moderate effect size d = 0.59; [0.44–0.73]). Less strong but still significant effects resulted for depression, anxiety, and insomnia. Most of the long-term outcomes remained stable. As moderators, the risk of bias (RoB) and the severity of tinnitus manifestations were identified.
Conclusions
: Internet-based therapy provides a valuable avenue for initial therapeutic contact, as supporting component in tinnitus treatment if accompanied by therapists. The heterogeneous quality with high drop-out rates or partly high RoB and the wide range of interventions (counseling, eCBT, mindfulness) might be considered as a limiting factor for a first-line management in tinnitus. So far, the use of e-Health is dependent on availability or user preferences.
Introduction
Chronic tinnitus is a leading cause of hearing-related disability, 1 affecting ∼15% of the European adult population (14.0% in men and 15.2% in women). About 1.2% of patients experience tinnitus as distressing (1.0% in men and 1.4% in women). 2 The prevalence of the tinnitus symptom increases significantly with age and hearing loss. 2 This condition implies a substantial burden for people and it also has a social and economic impact on health care systems and employment activity. The treatment of tinnitus causes high health care costs, especially if the tinnitus is experienced as distressing. 3
Chronic tinnitus is defined as a subjective sound or subjectively perceived noise without an external sound source. Often—but not always—the tinnitus symptom is preceded by hearing loss. Regardless of accompanying circumstances in the development of tinnitus (hearing loss, noise trauma, somatic aspects, or others), the suffering from tinnitus is to be primarily psychological in nature—tinnitus distress. 4 Current tinnitus management interventions are based on multimodal and biopsychosocial models, which include counseling and education programs, exercise programs, cognitive and behavioral strategies, relaxation techniques, sound and hearing supporting therapeutic strategies, self-monitoring systems, and self-management strategies. 5 –7
To treat patients with tinnitus more efficiently, more internet-based self-management, self-help, and low-contact treatment modalities have been offered in recent years—driven by the COVID-19 pandemic. 8 Studies have shown that treatment offered remotely via apps and videoconferencing can be used to replace or complement face-to-face clinical care for various conditions. 9 In the field of audiology and particularly in the field of tinnitus, telemedicine, in both full and mixed forms, has the potential to be used throughout the therapeutic process, at least in a supportive manner. 10,11
e-Health in tinnitus has been used as a tool for early screening, initial assessment, diagnosis, therapy, long-term monitoring, via the provision of web-based support, etc. In the last decade, computer platforms and smartphone apps have increasingly entered tinnitus treatment, mostly in the form of cognitive behavioral therapy (CBT) and sound therapy. 12 These apps are easy to implement in clinical practice and provide easily accessible treatment options. However, they could also improve the cost-effectiveness of tinnitus treatment. 13 Using these apps also presents a variety of challenges, most of which have not yet been overcome. (Digital tinnitus therapy applications face challenges such as ensuring data privacy and security, achieving interoperability with existing systems, securing user adoption, obtaining regulatory approval, managing costs and funding, addressing technical issues, bridging the digital divide particularly for older patients, obtaining clinical validation, engaging patients, and addressing ethical concerns.) Evidence of the therapeutic benefit via scientific studies is lacking for some approaches. 7,14
Currently, guidelines and treatment standards for tinnitus lack standardized definitions specifying which diagnostic characteristics necessitate the supportive or predominant use of e-health applications. 15 The treatments recommended in the guidelines are individual hearing aid fitting as needed and CBT. 4,16 These individually tailored, multimodal forms of treatment have proven to be effective, but they are also time-consuming and expensive. 3,17
A recent review on tele-rehabilitation for tinnitus emphasizes the importance of these forms of therapy to promote patient self-management and improve the cost-effectiveness of treatment. 18 A very recent review on internet-based therapies for tinnitus has been published, employing the following inclusion criteria: randomized, controlled trials conducted in English, involving human participants diagnosed with chronic primary subjective tinnitus. The review considered any telemedicine approach (including mobile, internet, telephone, and book) utilized to manage tinnitus. Various types of controls were permissible and only studies employing a questionnaire to measure tinnitus burden before and after each treatment arm were included in the analysis. 19
Taking into consideration this context, the primary objective of this systematic review was to assess the impacts of:
These detailed explanations provide a comprehensive understanding of the components and objectives of interventions targeting tinnitus distress and associated comorbidities within the framework of e-Health systems. In addition, we investigated various moderator variables regarding the efficacy of e-Health applications for tinnitus within this review. Our primary aim, extending beyond existing research, 18,19 was to assess online psychological interventions, specifically those grounded in CBT principles and exclusively guided interventions.
Methods
SEARCH
The reporting of this meta-analysis followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 statement. The project is preregistered (Open Science Framework; https://doi.org/10.17605/OSF.IO/ESN3F).
We searched PubMed, APA PsychArticles, Cochrane Central Register of Controlled Trials, Web of Science, and hand-searched references from systematic reviews without confining the publication date. Articles had to be in English or German language. This review focuses exclusively on German and English publications due to the research team’s proficiency in these languages, ensuring accurate comprehension and nuanced interpretation of the content. In addition, a significant proportion of high-quality and impactful research is published in these languages, which are also more readily accessible through major scientific databases. Limiting the review to German and English publications helps maintain consistency and comparability in methodologies and results across included studies.
Inclusion criteria included the following: adults, chronic tinnitus, randomized controlled trials (RCTs), at least some proportion of a psychological treatment, and internet-based intervention. Studies were retrieved until May 9, 2023. The process of identification and inclusion of studies is depicted in the PRISMA flow diagram (Fig. 1). As primary outcomes, tinnitus distress and tinnitus handicap were selected. Tinnitus distress is understood as suffering from tinnitus 20 and tinnitus handicap as functional limitations caused by the noise in the ear.
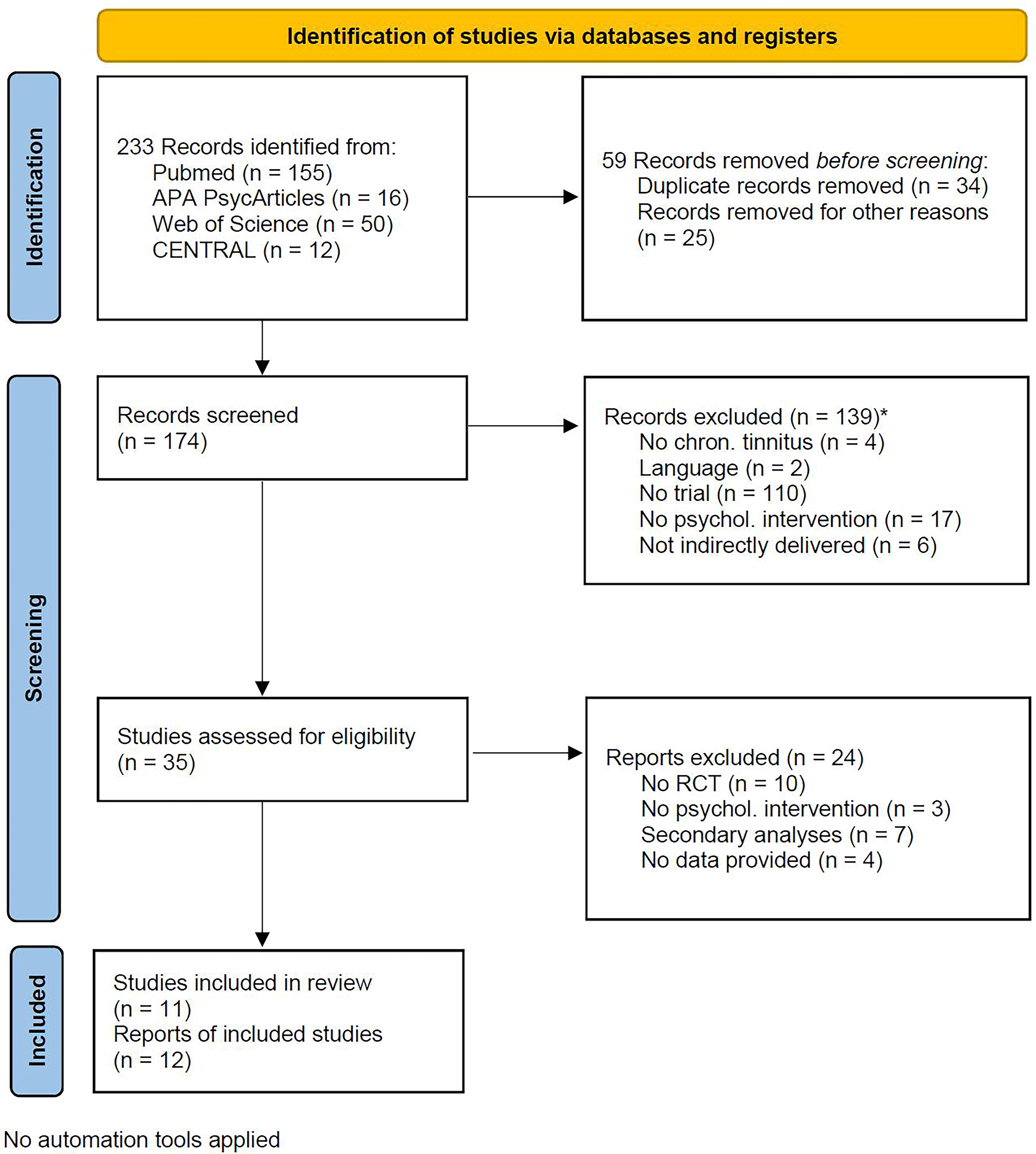
Flow of information through the phases of the review.
According to the European guidelines for chronic tinnitus, 6 we selected well-documented domains representing frequent comorbidities in chronic tinnitus: anxiety, depression, and severity of insomnia.
As search terms we combined “tinnitus” with “psychological treatment” OR “psychotherapy” and “telemedicine” OR “self-help” OR “online” OR “internet-based” OR “internet-based intervention” OR “smart phone” OR “e-Health” OR “mHealth.” All terms were evaluated and confirmed as Medical Subject Headings (MeSH) terms using the PubMed Thesaurus. The term was automatically translated and the full query can be seen in Appendix X.
RISK OF BIAS ASSESSMENT
The quality of included studies was assessed using the Risk of Bias 2 (RoB 2) Tool (RoB 2-T). 21 The ratings were estimated by investigators H.S. and P.B. and compared with the algorithm implemented in the RoB 2-T. The RoB 2-T tool is a comprehensive instrument used to evaluate the RoB in the results of RCTs. It is designed to assess the internal validity of a study’s findings. The tool includes several domains, each focusing on different aspects of trial design, conduct, and reporting: (1) bias arising from the randomization process, (2) bias due to deviations from intended interventions, (3) bias due to missing outcome data, (4) bias in measurement of the outcome, and (5) bias in selection of the reported result. Each domain is rated as “low risk,” “some concerns,” or “high risk” of bias and an overall RoB judgment is made based on the ratings across all domains. Very few discrepancies arose during the double-blind assessment using the RoB 2-T. These were resolved through collaborative discussion among the researchers, ensuring consensus and maintaining the integrity of the bias evaluation process.
The integration of study effect size was executed using Review Manager ([RevMan], version 5.4.1, The Cochrane Collaboration, 2020). We applied a study effect size approach. Thus, effect sizes for domains measured by more than one instrument were integrated and secondary analyses were excluded. Studies reporting only change scores or effect sizes 22,23 were recalculated in RevMan. Effect sizes were classified as small (0.2 ≤ ES < 0.5), moderate (0.5 ≤ ES < 0.8), or large (0.8 ≤ ES).
For moderator analyses, publication date (<>2015 as median) and—due to potential influence of reported design characteristics of the analyzed studies—the RoB classification (RoB high, moderate, low) were chosen. 21 Studies including “broad” tinnitus-related distress severity levels included patients across mild, moderate, or severe levels of tinnitus-related distress, whereas studies classed only as “severe” included patients with severe levels of tinnitus-related distress as defined by the, respectively, used distress questionnaire. Active control conditions like only counseling, sound therapy, or relaxation techniques have been shown to deliver better results. 24,25
An alternative treatment or intervention, enabling a direct comparison with the experimental condition helps in assessing the relative efficacy of the therapy. Passive control conditions serve to measure the natural course of the condition and any placebo effects, without providing an active comparison to the experimental therapeutic approach. Accordingly, the quality of the control condition (passive, i.e., waiting list vs. active) was analyzed as potential moderator too. Mode of delivery distinguished studies using telephone contact from those providing messenger-based or email contact. As Baumeister and colleagues 26 reported better outcomes for guided interventions, the extent of therapist guidance was introduced as moderator. The intensity of therapy-guided activity (low/moderate vs. high) was defined in terms of less or more than 10 min per week. The rigor of adherence control (proportion of participation control) was defined as low vs. high by weekly or module completion, based on monitoring by therapists.
STATISTICS
RevMan 5.4.1 estimated integrated effect sizes and confidence intervals for each comparison and moderator analysis. In addition, heterogeneity was estimated using I 2. The I 2 value quantifies the percentage of total variation across studies that are due to heterogeneity rather than chance. An I 2 value of 0% indicates no observed heterogeneity, while higher values indicate increasing heterogeneity, with 25% considered low, 50% moderate, and 75% high. In case of statistically significant heterogeneity, we chose random effect models. As estimates for intragroup effect sizes we calculated as Hedges’ g correcting for population bias.
Results
CHARACTERISTICS OF THE INCLUDED STUDIES
Overall, 906 participants took part in all included studies, with a nearly equal distribution between intervention and control conditions. The 11 studies allowed comparing 12 results, as one study scrutinized a three-armed design with two internet-delivered psychological interventions compared to a monitored internet discussion forum as control condition. 27 One study 28 analyzed face-to-face-delivered group CBT as an additional comparator, which was not included into this analysis. The majority of the included studies refer to one early developed internet-based self-help intervention by Andersson and colleagues. 22,29 As a consequence, nearly all subsequent studies included here examine adaptions, modified versions, or succeeding translations of this primal “cognitive behavioral self-help treatment.” 29 Two studies applied a telephone-based indirect delivery of therapy, 30,31 one study a combination of a mobile app and a website, while the remaining studies framed their interventions in websites, usually combined with email or telephone feedback and/or guidance. Attrition rates differed widely in both groups, with numbers of patients treated per protocol varying from 25% to nearly 100% in the intervention groups. Attrition rates were consistently lower for control groups. For intervention groups, short-term (pre–post) intragroup effect sizes varied from 0.2 ([very] small) up to 1.90 and long-term follow-up effect sizes (2 months up to 1 year) from 0.59 to 1.86, indicating nameable sustainability of the interventions under question. The control comparators rendered effect sizes from close to 0 up to 0.7 and one unique study delivering face-to-face clinical care even 0.96, representing a large effect. All but one study drew positive conclusions for their indirectly delivered psychological interventions and identified particular problems associated with those studies (e.g., high attrition rates, participants’ technical problems of online interventions) (see Table 1).
Description of the Included Studies
Henry 2018: Tele-Progressive Tinnitus Management (PTM)—severity adapted, some similarities to German guideline-recommendations.
For primary and secondary outcomes.
Tinnitus handicap.
Study effect model applied.
Based on more conservative imputation analysis.
Effect sizes based on change in THI.
Postassessments immediately after end of therapy/waiting period, if not otherwise stated.
IG, intervention group; CG, control group; ICBT, internet-based CBT; ACT, acceptance and commitment therapy; FU, follow up; TRQ, tinnitus reaction questionnaire; THI, Tinnitus Handicap Inventory; TFI, tinnitus functional index; GAD-7, generalized anxiety disorder; PSS, perceived stress scale; PTM, Progressive Tinnitus Management; ISI, insomnia severity index; PHQ-9, patient health questionnaire-9; HADS-A, Anxiety; HADS-D, Depression.
COMPONENTS OF THE INTERVENTIONS
The psychological interventions applied in the included studies all consisted of a bundle of different measures. Common therapeutic strategies referred to goal setting, structuring, motivation for maintenance of participation, or the provision of a structured framework for creating personalized plans. Relaxation techniques or meditation were imparted in all of the interventions. More specific CBT-related content consisted of thought analysis, cognitive restructuring, and planning of pleasant activities. Tinnitus-specific CBT elements expose to the tinnitus sound on a behavioral level, additionally use sound stimuli such as background noise to cope with the tinnitus experience; and attempting to achieve cognitive restructuring including reduction of negative emotions and avoidance.
Focus exercises should enhance the ability to shift the attention from tinnitus to other stimuli. Moreover, sound enrichment, hearing techniques, tinnitus reframing, or sleep management were discussed. Finally, positive imagery was a common element in many of the scrutinized studies too. One study, examining acceptance and commitment therapy (ACT), focused on mindfulness and distancing of internal experiences, as well as on the identification of personal values and goals and exercises that promoted willingness to experience tinnitus in this special context.
A waiting list condition was utilized as comparator in six studies, with a duration of eight weeks up to six months. Dobie and colleagues, 38 in a review of RCTs examining tinnitus treatments, demonstrated that nonspecific professional support and counseling might be helpful in tinnitus management. Monitoring by questionnaires, a moderated discussion forum, or systematically delivered face-to-face clinical care were used in the remaining five studies as a more valuable comparator. The presence of an active control condition was considered as a relevant moderator. Additional moderators were derived from (1) the mode of delivery of the intervention, (2) the level of guidance, and (3) the rigor of patients’ participation/adherence control. All studies but one providing follow-up data decided to offer a subsequent active intervention to the participants of the control group. As an exception, control group participants in the study of Henry and colleagues 39 had to wait until the end of the 6-month follow-up of the active condition before being offered tele-psychological tinnitus management (Tele-PTM).
ASSESSMENT OF RISK OF BIAS
All studies but two had a low RoB for randomization (D1, Fig. 2). Some concerns in this respect resulted from a nonrandom allocation sequence and the use of a worksite-based cluster randomization. Most of the studies followed an intention to treat analysis, resulting in low RoB for D2. Exceptions were studies with a high and/or unbalanced number of participants not receiving the allocated program. Moderate or high attrition rates, moreover, led to some concerns or high-risk grading for those studies, respectively (D3).

Risk of bias assessment.
Apart from one study explicitly reporting that the analysis process was masked for group allocation, some concerns related to the measurement of the outcomes could not be ruled out for all other studies: it could not be excluded that the assessment of the outcomes was potentially influenced by the knowledge of the intervention received (D4). Most studies reported to follow a prespecified statistical analysis plan or had prespecified outcomes, resulting in low RoB within this domain (D5). Multiple eligible analyses were available for some studies, offering per protocol vs. intention to treat analyses, and/or several imputation methods, which were in these cases appropriately reported and did not result in concerns for RoB. Due to the presence and handling of missing data, a high RoB was indicated for three studies. The majority of the remaining studies had a rating of some and mostly minor concerns and two studies had no detectable or relevant RoB.
Data for the integration of the selected domains of interest (tinnitus distress and handicap, depression, anxiety, and insomnia) were provided by at least 7 studies, with the smallest number of comparisons for insomnia (8 comparisons from 7 studies) and nearly complete data for anxiety (11 comparisons from 10 studies). These analyses included 360 up to 481 participants in the intervention groups and 309 up to 506 participants in the control conditions.
EFFICACY OF PSYCHOLOGICAL e-HEALTH INTERVENTIONS AT POST-TREATMENT
The results of the meta-analytic integration can be seen in Figs. 3–7. Tinnitus distress improved significantly in seven of the nine studies reporting this outcome. The resulting effect size can be considered large or close to large (0.78, CI: 0.51–1.06, p < 0.001). Heterogeneity for this comparison was high (I 2 = 75%; p < 0.001) (Fig. 3). A similar picture, but with less marked results, appeared for Tinnitus handicap. Six out of 10 studies reported statistically significant changes in favor of the participants in the intervention groups (Fig. 4). The resulting effect size can be considered as moderate (0.54, CI: 0.31–0.76, p < 0.001). Again, the proportion of heterogeneity for this comparison was high (I 2 = 65%; p < 0.001).

Forest plot for tinnitus distress (pre–post).

Forest plot for tinnitus handicap (pre–post).
Except for one study, all included studies reported anxiety as an outcome. With only two exceptions, all studies observed a more substantial improvement in participants belonging to the intervention groups. The effects for the remaining studies did not significantly deviate from zero in four cases, while five studies identified moderate effect sizes for this comparison. The resulting total effect size was small to moderate (0.37, CI: 0.19–0.54, p < 0.001) (Fig. 5). The proportion of heterogeneity for this comparison was smaller but still high enough for a decision for a random effect model (I 2 = 37%; p < 0.10).
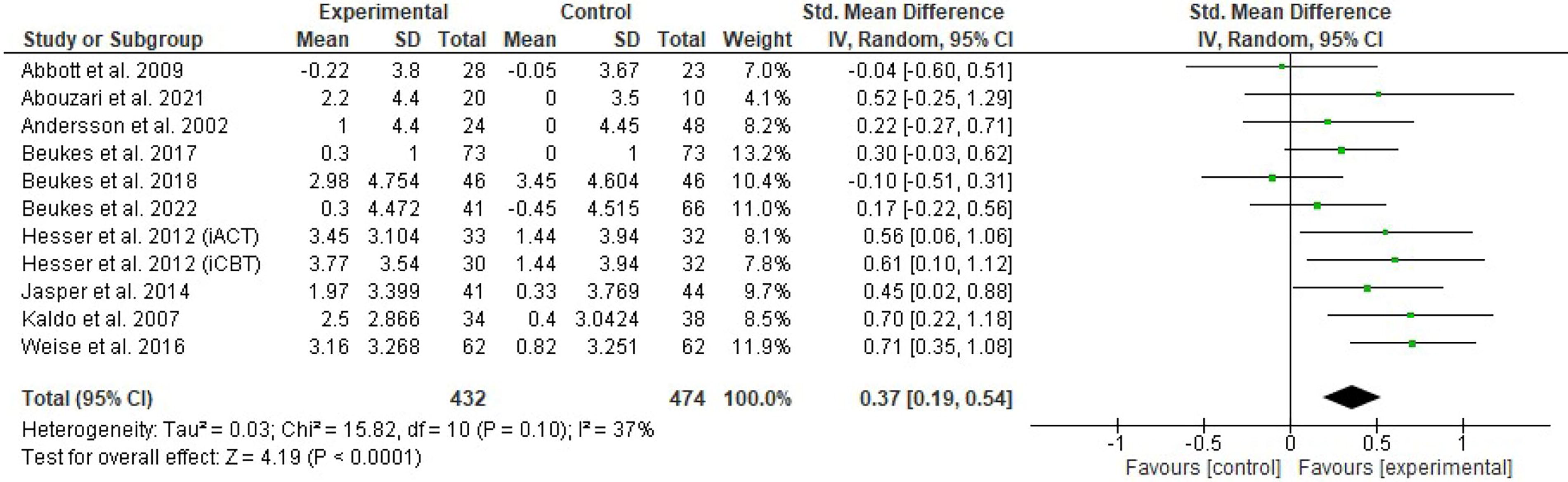
Forest plot of comparison: secondary outcome Anxiety (pre–post).
The degree of depression was assessed in nine studies. Again, the two studies reporting no improvement for anxiety did not find an improvement for depression too. The effects for the remainder were not significantly different from zero for three more studies, while five studies reported moderate to large effect sizes for this comparison. The resulting total effect size was small to moderate (0.34, CI: 0.14–0.54, p < 0.001) (Fig. 6). The proportion of heterogeneity was elevated (I 2 = 53%; p < 0.02).
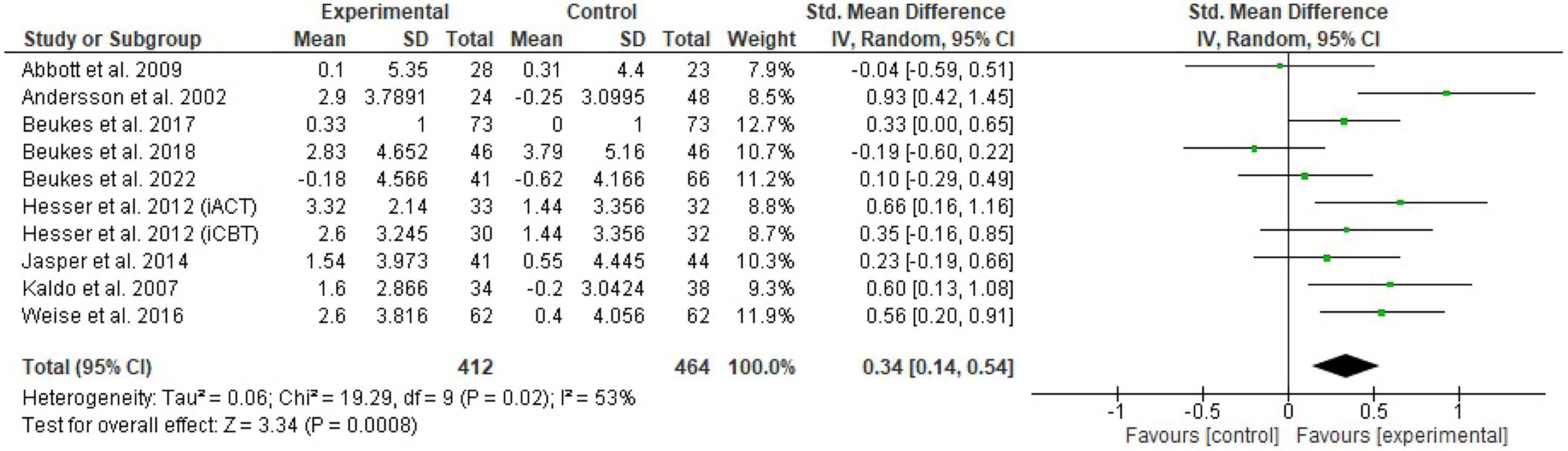
Forest plot of comparison: secondary outcome Depression (pre–post).
The insomnia severity index assessing insomnia as often co-occurring clinical phenomena in patients with tinnitus was reported by seven studies. All studies found a more pronounced improvement for the participants of the intervention groups, with four of them reaching statistical significance. The resulting total effect size was small to moderate (0.44, CI: 0.29–0.59, p < 0.001) (Fig. 7). The proportion of heterogeneity for this comparison was small and a fixed effect model was chosen (I 2 = 0%; p < 0.56).
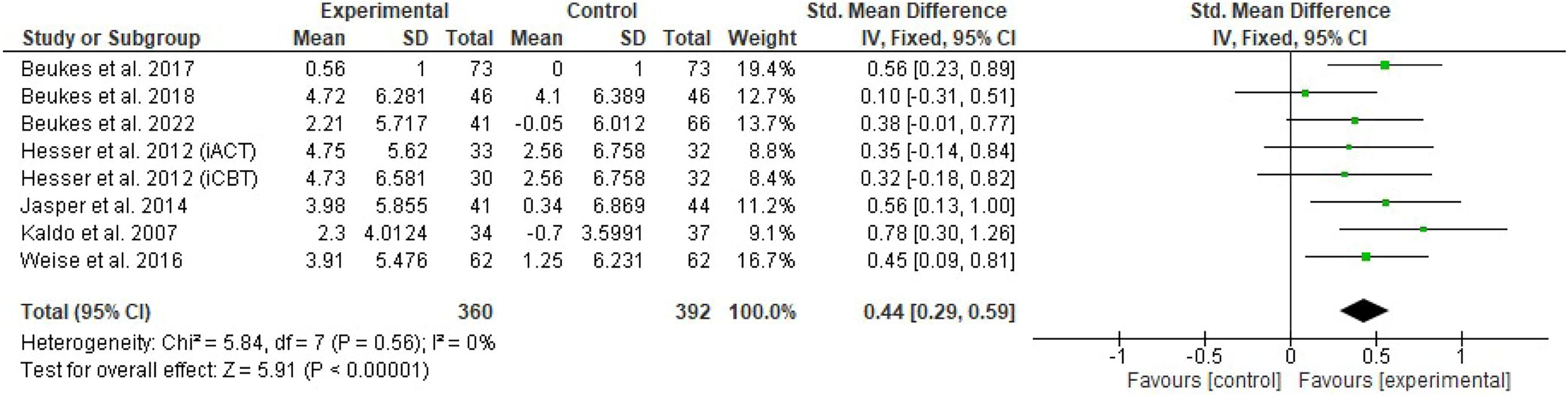
Forest plot of comparison: secondary outcome Insomnia (pre–post).
MODERATOR ANALYSES
Regarding the formal characteristics of the included studies, the effect sizes derived for tinnitus distress reduction for more recent studies did not differ from the older studies (Table 2). The quality of the study execution as determined by the RoB assessment resulted in statistically different effect sizes for those, with the highest effect sizes when RoB was low (two studies) and still large when a high RoB was indicated (three studies), while a moderate RoB was associated with a moderate effect size. Severe initial tinnitus distress was related with a higher reduction of distress, although this trend did not reach statistical significance. The effect sizes of studies with active control groups as compared to studies with passive control conditions appear to be slightly smaller. However, their confidence intervals overlap and so this difference was not significant. Regarding the mode of delivery, the effect of therapeutic guidance and rigorousness of adherence control was small and no significant differences were observed, while electronically delivered interventions, smaller doses of guidance, and active control groups being associated with higher effect sizes.
Role of Moderators on Intervention Effect Size for Tinnitus Distress
Discussion
EFFECTS OF INTERNET-BASED THERAPIES AND e-HEALTH SYSTEMS (PROS AND CONS)
A total of 11 controlled, randomized primary studies with psychological interventions that were conducted via the internet but involved psychologists or therapeutic staff were included in this review. These trials involved more than 900 patients distributed across experimental and control groups. The focus was placed on selecting RCTs and therapist or trained personnel being involved during intervention to ensure direct comparability of effects with the current standard of tinnitus therapy—CBT administered by psychologists. Tinnitus distress and tinnitus related handicap in daily functioning improved significantly by e-Health interventions. For tinnitus distress (measured by TQ and other instruments) characterized as the emotional experience of suffering due to tinnitus, this is in line with other studies. 19,40,41
In our study, we defined tinnitus handicap as referring to functional limitations caused by the auditory disturbance (measured by THI) as second primary outcome. The effect size for tinnitus handicap across all selected studies were robust but smaller. We attribute this to a certain overlap in constructs. Tinnitus distress is defined as the emotional suffering experienced due to tinnitus. Although, under the term “handicap,” we primarily consolidate the audiological limitations imposed by tinnitus, it appears that the employed internet-based therapies are primarily effective in reducing emotional distress and enhancing overall quality of life. This is further supported by the smaller, yet significant effects observed in anxiety, depression, and sleep disturbances, all of which showed notable improvement following internet-based therapy.
ICBT EFFECT SIZES
Because CBT is one of the most recommended evidence-based treatments for patients with tinnitus, it is not uncommon that studies have looked at internet-based CBT (iCBT) strategies. iCBT has been shown to be effective in treating post-traumatic stress disorder, anxiety, and depression. 42,43 Internet-based intervention programs such as iCBT and others such as internet-delivered ACT (iACT). This approach involves providing ACT interventions through internet-based platforms or applications, allowing individuals to access therapy remotely. iACT has become very popular in recent decades due to major advances in technology and the accessibility of the internet. Although iCBT and other CBT-based self-help treatments are a frequently researched topic in the e-Health field, the effect of specific apps and other applications compared to multimodal, individualized analog therapies has not been directly compared. In addition, there is considerable evidence that treating tinnitus sufferers with hearing impairments with a suitable device has a good therapeutic effect. 44 Analogous forms of therapy (preferably multimodal) can be used to diagnose a possible hearing impairment and, if indicated, to accompany and implement a hearing aid fitting.
The effectiveness of iCBT with guidance was also confirmed for tinnitus treatment in 11 studies. 22,23,27,28,30,32 –35,37,45 Most commonly, CBT is offered by a trained psychologist. In the studies by Beukes and colleagues, 23,34,45,46 patients received counseling from an audiologist. In a systematic review and network meta-analysis of CBT, larger but not statistically significant effect sizes (Standardized mean difference [SMD]: 3.44; 95% CI: −0.022, 7.09; I 2: 99%) were found for guided self-administered forms of CBT on tinnitus health-related quality of life, which refers to an individual’s perceived physical and mental well-being in relation to their health status and medical conditions. However, only face-to-face CBT was shown to result in statistically significant improvements (SMD: 0.75; 95% CI: 0.53, 0.97; I 2: 0%). 47 Thus, it can be assumed that although e-Health offers are readily accepted, especially by people with internet affinity, this form of therapy is not equally efficient for all tinnitus sufferers. A combination of face-to-face therapy with digital modules (e.g., for exposure exercises, information transfer or home assessment) is conceivable and desirable. To our knowledge, there is still a lack of appropriate combination approaches that have been validated by studies.
SECONDARY OUTCOMES
We were able to show a medium, but statistically significant effect of the psychological impairment caused by anxiety, depression, and sleep disorders on the therapy effect. Tinnitus is known to be closely associated with anxiety, depression, stress, and sleep disorders. 48 –50 The more serious these comorbidities, the poorer the prognosis for tinnitus. 51 These additional complaints have a major impact on the choice of therapy plan. 52 Gender also plays a role in how patients perceive their tinnitus. Men show fewer tinnitus-related symptoms than women. 53 Second, the prevalence of chronic tinnitus increases with age and older patients rate the loudness, annoyance, and distress of the tinnitus they experienced as higher. 54 Third, the patient’s social variables may be important, such as education or social support and integration. In addition, hyperacusis is often a comorbid complaint of tinnitus patients, which leads to a higher degree of tinnitus severity and psychological stress. 4 The above factors can have an impact on the effectiveness of a treatment and should therefore be considered in future research.
However, all these positive aspects also entail corresponding risks. Although effects of medium magnitude of online therapy, especially of online CBT on tinnitus handicap and on tinnitus distress, are found, the result cannot be classified as full success of e-Health therapies for tinnitus. The use of internet-based CBT for tinnitus should be well considered for several reasons:
LITTLE DIVERSITY OF PUBLICATIONS
The majority of the included studies refer to an internet-based self-help intervention first presented by Anderson in 2002. 22 Almost all studies included here are to be regarded as adaptations, modified versions, or follow-up studies of this original “cognitive-behavioral self-help treatment.” 29 The content orientation of 8 of the 12 included studies thus relates directly to the first publication. On the one hand, this can be an advantage, as different tinnitus samples with different characteristics and different contextual factors can be better identified. On the other hand, it must be clearly pointed out that all reviews for e-Health to date have only included studies from Europe and North America.
RISK OF BIAS
This is also supported by the RoB assessment of the 11 studies summarized here. Only 2 studies out of 11 36,37 showed a low probability of bias. Henry and colleagues evaluated the efficacy of delivering coping skills from Progressive Tinnitus Management by telephone in an RCT. Results showed that the Tele-PTM group had significantly better outcomes than the waiting group. These results were consistent across all outcome measures, indicating not only a reduction of tinnitus functional distress but also increased self-efficacy, improvements in measures of anxiety, and depression. Weise and colleagues assigned patients to therapist-guided iCBT or to a moderated online discussion forum.
Regarding tinnitus-related distress, positive effects of iCBT were supported by large effect sizes. For the secondary outcomes (tinnitus acceptance, anxiety, depression, and insomnia) significant interactions with small to medium effect sizes were found. In almost all studies in this review (except Beukes 46 ), the analysis of results was subject to certain limitations. In the study of Beukes et al., iCBT for tinnitus led to significant improvements 1-year postintervention for tinnitus and related difficulties like insomnia, anxiety, depression, hearing handicap, hyperacusis, and life satisfaction. The best predictors of improving tinnitus severity 1-year after the intervention were greater baseline tinnitus severity scores, reading more of the modules, and higher satisfaction with the intervention. Unwanted events (worsening of symptoms, the emergence of new symptoms, negative well-being, and prolongation of treatment) were reported by 11% of the participants. The RoB in the analysis of the results may to some extent be due to the specifics of e-Health applications, but it is important to consider it before using such strategies therapeutically.
HIGH DROPOUT RATES
A limitation of the studies considered was the high dropout rates. Dropout rates for the use of smartphone apps have not been reported in all but two studies. Henry et al., 31 for example, reported a dropout rate of 8%.
Some of the included studies discussed the high dropout rates. First, iCBT might not be sufficiently motivating and engaging despite regular therapeutic support. 23,32 In addition, it is very demanding and time-consuming for the patients. 55,56 Thus, the therapist-guided CBT seems to be advantageous for patients in terms of (intermediate) motivation. Finally, the patient’s attitude toward the treatment and their personality can have a major impact. Patients with an open personality who had hope for improvement and believed the treatment was serious showed the best results. 57,58 However, it must be noted that patients who expect positive treatment outcomes are often also patients who are likely to improve.
MODERATOR VARIABLES
Contrary to our assumption that traditional telemedicine, now superseded by modern apps on smartphones, has different therapeutic effects in complex programmed applications for the implementation of CBT for tinnitus, we were unable to confirm this in the moderator analysis. The type of presentation of the therapeutic intervention (internet/mail or telephone), the amount of time spent with the therapist, or the intensity of monitoring the applications also had no effect on the therapeutic outcome. For a pure waiting group, the therapy effects tended to be more pronounced than in concurrent control groups with interventions other than CBT. The initial level of tinnitus distress in the study population also had an influence on the treatment effect in the included studies. People with moderate tinnitus burden benefit significantly less from ECT than those with high tinnitus distress. This is an effect that is known from CBT studies. 44 Patients with a lower initial tinnitus distress level seem to be less willing to complete the strenuous modules and are more likely to discontinue the study or to not respond. 56 However, the quality of the studies (RoB) had a significant effect on the therapy effects observed. Studies with a low bias showed larger effect sizes than studies with high bias. In the latter case, it can be speculated that the measured treatment effects are also influenced by the bias. This is supported by the fact that medium bias levels resulted in less significant effects than low and high bias levels.
Limitations of the Studies
All included studies revealed some concerns about RoB. However, a comparison of efficacy between studies was not possible due to the variety of questionnaires used to measure tinnitus distress level, severity, or distress. In addition, some critical confounders were not considered in all studies. Only a minority of the studies looked at the proportion of participants with hearing loss or how many patients used hearing aids. The studies focusing on e-Health applications such as self-help manuals, self-help devices, and smartphone apps also rarely defined the proportion of participants with hearing loss. Hearing loss is an important risk factor for the development of tinnitus. 59 In addition, there are patients with audiometrically normal hearing who suffer from tinnitus. 44,60 Therefore, hearing loss could be an important confounding variable to consider. An audiometric examination of patients with tinnitus is required and so far cannot be carried out without direct consultation. 4
Various negative aspects of e-Health offerings for tinnitus can be summarized: The absence of face-to-face communication can limit the depth of the therapeutic relationship, potentially affecting the quality of the therapeutic process. Not everyone has access to the necessary technology or possesses the digital literacy required for effective engagement with internet-based therapies. There may be concerns related to the security and confidentiality of sensitive health information transmitted over online platforms. Some individuals may not respond well to the standardized nature of certain internet-based interventions, as these may lack the tailored approach of an individualized personal therapy. Issues such as the ethical use of technology in therapy and the potential for miscommunication or misinterpretation of online interactions need careful consideration too.
Nevertheless, the range of digital health applications for tinnitus will continue to develop. Therapeutic efficacy has been proven in this review. Especially when access to specialists or multimodal therapies is difficult and to increase motivation to continue therapy or to continue learning after therapy, e-Health therapy offerings will be useful and important. When analog alternatives are not available and trained specialists (psychologists for CBT) are involved, digital services could replace direct therapy with therapeutic relationship building and social exchange.
Conclusions
The results of this systematic review indicate that, overall, there is low to moderate evidence that e-Health applications for tinnitus in the form of iCBT with guidance (self-help manuals, self-help devices, smartphone apps, and other internet-based interventions) effectively reduce tinnitus distress and handicap. Internet-based therapy might form an additional tool to the recommended in-person care that patients currently receive. This review emphasized, that the greatest barrier to the success of iCBT is the lack of compliance to treatment. Factors such as lack of time, engagement, motivation, age, social factors, and openness of the patient resulted in participant dropout and should be considered.
Although (e)CBT is not always accompanied by psychologists, active dialog seems to have a significant influence on the therapeutic effect. High drop-out rates seem to speak in favor of a connection between motivation, effort, and therapy effects in those affected by tinnitus, which are greater with direct therapy, possibly due to active feedback and interactional support.
Future research should consider limiting the ROB and should further explore which factors are most likely to cause the lack of compliance and how clinicians can counteract these factors. The study situation is statistically heterogeneous, but largely consistent as far as the individual outcomes are concerned. Not many studies are currently available (no manufacturer-independent studies on previously used apps and DIGITs f. e in Germany). Regarding the current developments in the field of psychotherapy for linking therapeutic intervention with technical possibilities, internet-based therapy with therapists represents an interesting possibility to support face-to-face or group therapy. If direct therapy methods are not available and tinnitus stress is high, they also offer a good opportunity for initial therapeutic support in addition counseling by otolaryngologists. Further developments and corresponding research on effectiveness is therefore to be expected and recommended.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
Christian Dobel is funded by the German Research Council (Do711/10-3).