
Abstract
Background:
The availability and utilization of telehealth services have been rapidly increasing in the past decade, which paved the way for ophthalmological care to be offered more easily and conveniently. However, the proficiency of telehealth in the context of ophthalmical care still requires further studies to prove its effectiveness. This study examined the proficiency of general practitioners in a telemedicine platform in identifying red flag symptoms, suggestive of retinal detachment, and devising optimal management strategies.
Methods:
Our cross-sectional study used chat-based consultations on Altibbi Telemedicine platform (2018–2023) to study ophthalmical patients presenting with “blurred vision” or “blindness.” Those endorsing red flag symptoms were categorized as having “positive symptomatology” and those reporting none as having “negative symptomatology.” Management plans were classified as referral or reassuring. Statistical analysis was performed using IBM’s Statistical Package for Social Sciences to examine associations between symptomatology and other variables. p values below 0.05 were considered statistically significant.
Results:
Five hundred and fifty (n = 550) patients with a mean age 22.5 ± 13 years were included. Patients expressing positive symptomatology were more likely to be referred relative to those expressing negative symptomatology (81% vs. 61%, p < 0.001). No significant difference was found between genders and referral (p = 0.053) or age and referral (p = 0.231). Multivariate regression showed a significant correlation between positive symptoms and referral (adjusted odds ratio [aOR]: 2.0; 95% confidence interval [95% CI]: 1.3–3.3), none between gender (aOR: 1.5; 95% CI: 0.9–2.2) or age (aOR: 1.0; 95% CI: 0.9–1.1) and referral odds.
Conclusion:
The telemedicine platform studied is effective in referring cases with red flag symptoms to urgent care, regardless of age and gender.
Introduction
The increase in the use of technology worldwide permitted the development of new modalities for eyecare, especially with the rise of the novel coronavirus (COVID-19), a public health emergency. 1 Many countries were forced into taking rapid action to control the spread of the virus by implementing lockdowns and quarantines, which by itself represents a major barrier to the normal consultation in the ophthalmology clinic. With the rapid adaptation that was required to fight the pandemic alongside the need to continue providing ophthalmological care, the concept of telehealth was implemented into various fields of medicine, including ophthalmology. 2 The typical telehealth service allows patients to communicate with primary care physicians, where the provider may either manage the condition through such telehealth consultation or triage patients to more specialized services or the emergency department. This allowed for ophthalmological care to continue being provided while keeping both the providers and patients safe during the consultation. 3
However, only a few studies conducted previously to describe the implementation of telehealth in ophthalmology care and its effectiveness in providing efficient virtual consultations and developing appropriate management plans, mainly for urgent ophthalmical complaints. 4,5 In two cases, telemedicine has been used in the diagnosis of retinal detachment, where primary care physicians communicated fundus images with specialized physicians to facilitate the management of the disease. Retinal detachment is a serious ophthalmical emergency, and its sequelae can be preventable with early surgical intervention, with high success rates following a single operation. This makes its early detection and referral paramount in the prevention of complete retinal detachment and vision loss. 6 –9 If patients with ophthalmical symptoms suggestive of retinal detachment were reassured by the primary care during the consultation, this will lead to delayed diagnosis and management of this ophthalmical emergency.
Although different prior reports advocated for the wider implementation of teleophthalmology, no previous study quantitively assessed its effectiveness for triaging patients with possible urgent complaints. In this study, we evaluated the accuracy of general practitioners used by a telemedicine platform in identifying the red flag symptoms associated with retinal detachment and devising optimal management strategies.
Methods
SETTING, SAMPLING, AND DESIGN
We conducted a cross-sectional study to evaluate the proficiency of general practitioners used by the largest Middle East and North Africa (MENA) telemedicine platform, Altibbi, in detecting ophthalmical conditions in patients who reported symptoms of blurred vision and blindness through chat-based medical consultations, between June 2018 and January 2023.
The study used a dataset of all medical consultations provided by the telemedicine platform using Altibbi consultation history database. Altibbi, established in 2011, is the first telemedicine platform in the MENA region. Its objective is to facilitate access to health care by using a large network of medical professionals. As of 2023, Altibbi’s network comprised over 1,500 certified physicians who provide remote medical consultation through audio calls or text messages. 10,11
DATA EXTRACTION
From the dataset consisting of all ophthalmical patients, we extracted demographic data including age, gender, and country of residence. We subsequently narrowed down the dataset to only include patients who reported “blurred vision” or “blindness” as their presenting symptoms. In addition, we only included patients who primarily sought consultation via text message and excluded those receiving audio-based consultations from our study.
ASSESSMENT OF SYMPTOMS AND MANAGEMENT PLANS
We reviewed the full-text message exchange between doctors and patients in our selected sample to determine if patients positively endorsed the “red flag” symptoms suggestive of retinal detachment, including sudden onset of symptoms, floaters, flashes of light in one or both eyes, and a curtain-like shadow over the visual field. Patients who positively endorsed any of the red flag symptoms were categorized as having positive symptomatology, whereas those who did not report any such symptoms were classified as having negative symptomatology.
Moreover, based on the text message exchange between doctors and patients and the final recommendation provided by the doctor, the management plans were classified into two categories: an emergent/referral management plan if the physician requested a referral to an ophthalmologist, or reassurance if they included any of the following: medications (eye drops, painkillers, and/or cortisone), lifestyle modifications, or if the patient was informed that the symptoms would gradually improve and resolve over time without any intervention.
After categorizing patients into having positive or negative symptomatology as well as classifying the management plans provided by physicians as referral or reassuring, we constructed a flowchart presenting our findings (Fig. 1).
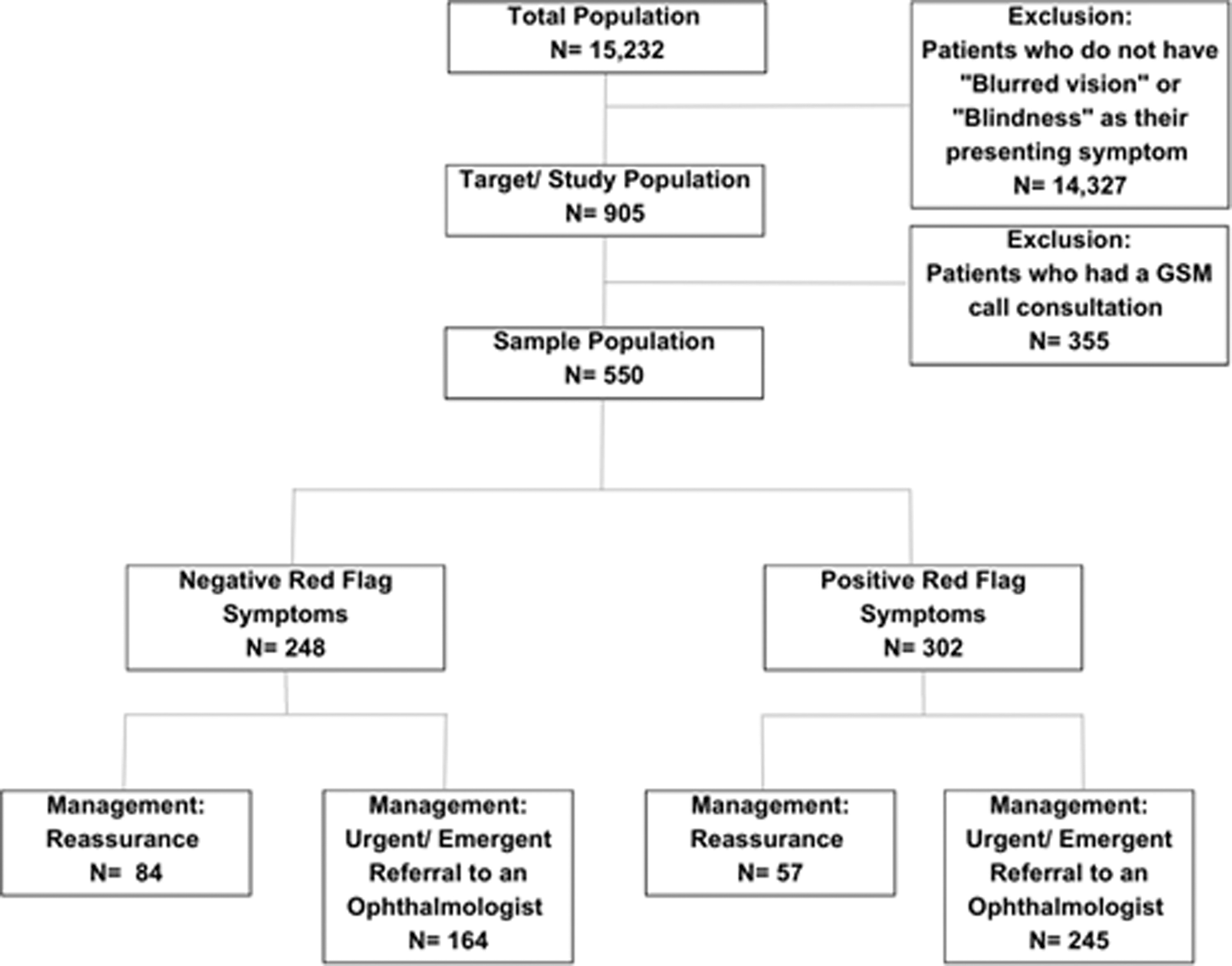
Flow chart of study population and exclusion criteria.
STATISTICAL ANALYSIS
Descriptive statistics (mean ± standard deviation) were used for continuous variables. Percentages (counts) were used for categorical variables. Data were compared using Chi-square analysis for categorical variables and two-way independent sample t-test for continuous variables. Normality was tested using the Shapiro–Wilk test and normality plots. Multivariable logistic regression was carried out with adjusted odds ratios (aOR) and 95% confidence intervals (CIs) produced for the covariates. IBM’s Statistical Package for Social Sciences Version 28.0, Armonk, NY was used for statistical analysis. A p value of less than 0.05 was considered statistically significant.
Results
Our study recruited a total of 550 participants. Out of the total 550 patients, 62 and 30 participants did not disclose their age and gender, respectively. The total cohort had a mean age of 22.5 ± 13, 57.5% (n = 299) were females and 42.5% (n = 221) were males. The majority of the patients in the sample, 64.5% (n = 355), were from Saudi Arabia. The remaining sociodemographic data can be found in Table 1.
Descriptive statistics for the included patients
62 participants did not provide age.
30 patients did not provide an answer for gender.
Out of the total 550 patients included, 54.9% (n = 302) endorsed at least one of the red flag symptoms. Of those, 81.1% (n = 245) were referred to an ophthalmologist for further management, and the remaining 18.9% (n = 57) were reassured and prescribed symptomatic relief. On the contrary, 45.1% (n = 248) patients expressed negative symptomatology. In this cohort, 66.1% (n = 164) were referred for further treatment and 33.9% (n = 84) were reassured (Fig. 1).
Patients who endorsed positive red flag symptoms were more likely to be referred for further management in comparison with those who did not endorse such symptoms (81% vs. 61%, p < 0.001). There was no significant difference between females and males in relation to referral to ophthalmology (78% vs. 70%, p = 0.053), and age had no significant effect on referral status as the mean age of those referred was 23.0 ± 13.3 years vs. 21.3 ± 12.0 years for those who were reassured (p = 0.231).
On multivariable regression analysis, patients with positive red flag symptoms were more likely to be referred to an ophthalmologist for further treatment (aOR: 2.0; 95% CI: 1.3–3.3). However, neither female gender (aOR: 1.5; 95% CI: 0.9–2.2) nor age (aOR: 1.0; 95% CI: 0.9–1.1) was associated with increased odds of referral (Table 2).
Outcome of Multivariable Logistic Regression
CI, confidence interval.
Discussion
Telemedicine was an integral part of the health care system during the COVID-19 period. In our analysis of telemedicine consultations, we found that the majority of blurred vision consultations for patients who also expressed symptoms suggestive of retinal detachment (aka. Red flags) were referred for specialized ophthalmical practice. Moreover, patients who expressed these red flag symptoms were more likely to be referred. However, 18.9% of symptomatic patients were reassured without proper referral or counseling about the possibility of retinal detachment, warranting proper education of counseling physicians about red flag symptoms in such consultations. This finding further suggests that telemedicine is a promising tool to complement the traditional face-to-face consultation. In addition, our study suggests no association between age and gender on the probability of patients being referred to the ophthalmologist clinic.
Age was not found to be associated with the management plans provided in the study. The absence of a correlation between age and management plans may be attributed to the possibility that doctors considered traumatic retinal detachment as a potential diagnosis in younger patients since it comprises 15% of all retinal detachments and is much more common among the young population. 12 Despite the recognized elevated risk of diabetic retinopathy in older patients, the projected surge in the global incidence of this condition may urge doctors to refer patients to an ophthalmologist irrespective of their age. 13 This is particularly important in the Saudi Arabian population, which makes up over half of the consultations in our population, where the prevalence of diabetic retinopathy is approximately 20% among patients with diabetic. 14 Moreover, an increased likelihood of in-person medical visits is suggested for older patients, which may be attributed to differences in access to the internet and technology. 15 This therefore also explains the mean age of our population being younger. The severity of symptoms could also be a contributing factor, as older patients may experience worse symptoms and are more likely to seek in-person medical consultation. However, both older and younger patients show an interest in telemedicine because of its availability and usefulness in settings where clinic access is difficult, for follow-up care for chronic illness, and for the management of comorbidities.
The upsurge in interest toward telemedicine may be in part because of its role in providing a safer alternative to the possibility of contracting COVID-19 and its associated complications from clinical environments, particularly during the period spanning 2020 and 2021. This fear may have been amplified among the older population who are more likely to suffer from chronic illnesses putting them at higher risk of COVID-19 complications, yet the global dissemination of fear and misinformation pertaining to the pandemic likely prompted patients, both young and old, to opt for telemedicine consultations as opposed to in-person visits to health care facilities. 16
Moreover, the results of our study indicate that there are no gender disparities in terms of female patients and their odds of being referred to in-person clinics. This lack of association between gender and management plans could also be because of the global increase in diabetic retinopathy. Despite the well-established higher risk of diabetes among males, the risk of diabetic retinopathy remains less pronounced between females and males. 17 This, therefore, explains the reason doctors may refer patients expressing positive symptomatology regardless of their gender. Furthermore, although the majority of patients with rhegmatogenous retinal detachment, the most common type of retinal detachment, are male, no significant association between gender and odds of referral was found. This emphasizes how retinal detachment is a medical emergency requiring urgent intervention, which should prompt doctors to refer patients presenting with positive symptomatology suggestive of the condition, regardless of gender. 18
Our study demonstrated that patients expressing positive symptomatology were more likely to be referred to an ophthalmologist; this reflects the overall proficiency of the general practitioners in the telemedicine platform in managing those patients appropriately. However, it is imperative to acknowledge that our research has uncovered a subset of patients who needed to be adequately referred yet were not, suggesting limitations in the referral process. This finding may be attributed to general practitioners commonly encountering a wide range of complex and diverse medical conditions, making it challenging to make accurate diagnoses and suggest appropriate management plans for the vast array of medical conditions they encounter. It is crucial to acknowledge that certain doctors have been terminated according to the company’s quality measures. Therefore, the timeline of the study does not reflect the quality of care provided by the physicians who are currently part of the team.
Various strategies have been proposed in the literature and can be adopted to enhance general practitioners’ effectiveness in providing comprehensive patient care. Introducing mandatory work-based continuing education programs is a viable solution. Conducting programs for training doctors emerges as a key driver, facilitating the maximization of proficiency and efficacy in utilizing telemedicine tools, ultimately resulting in improved accuracy and diagnostic capabilities. 19 Controlled trials of continuing education strategies indicated that incorporating personalized feedback and work prompts into continuing education programs can significantly enhance their effectiveness. 20 Consequently, the provision of comprehensive training to doctors holds substantial promise in enhancing the quality of patient care while effectively leveraging medical resources.
Although our study used a telemedicine platform that provides services via chat-based and audio-call interactions between general practitioners and patients, there is a potential for greater effectiveness by expanding its network to incorporate additional specialized health care professionals. Collaborative efforts among general practitioners, specialists, and medical institutions have the potential to enhance telemedicine’s impact, particularly in situations involving novel and unfamiliar challenges like the COVID-19 pandemic, which necessitate medical counseling and team management. Furthermore, dedicated apps may facilitate prescription delivery to preselected pharmacies, providing patients with convenient access to the necessary medications. 21
Exploring strategies for remote monitoring of both outpatients and inpatients may also significantly enhance the effectiveness of telemedicine platforms. Our study included patients who primarily sought medical advice and were addressed through referral or reassurance without subsequent follow-up care. Implementing follow-up care effectively alleviates the burden on both doctors and patients.
Inpatient monitoring through telemedicine for follow-up purposes offers the potential to mitigate the risk of nosocomial infections and minimize the utilization of personal protective equipment compared with traditional medical rounds. Expanding outpatient monitoring may be achieved through several remote specialty-specific ambulatory practices. Remarkably, a study conducted in countries including the United States, Italy, and India demonstrated virtual migration rates ranging from 60% to 95% of the usual practice in specific specialties, thereby fostering bilateral and international collaboration to ensure equitable health care access. Another illustrative example involves the establishment of a pediatric telecardiology service in various Portuguese-speaking countries in collaboration with universities based in Portugal. This pioneering effort can serve as a valuable precedent for other specialties, such as teleophthalmology, to follow. 22,23
Auditing is a vital tool in assessing performance and identifying needs. 24 China has implemented a performance measurement system to evaluate the effectiveness of general practitioners to enhance the delivery of quality primary care services. 25 Moreover, instead of relying solely on text-or audio-based communication, patients could upload comprehensive medical histories, current and previous prescriptions, and available medical records. This capability enables doctors to gain a better understanding of each patient’s case, facilitating the formulation of appropriate treatment plans. 21 Such services may be promising for both emergent and nonemergent cases. This feature aids doctors in accurately referring complicated and high-demand cases to in-person medical services while effectively managing others remotely.
In addition, the integration of artificial intelligence into telemedicine platforms can play a vital role in elevating the overall quality of health care provided. 23 Data protection through cloud-based systems may also enhance the effectiveness of telemedicine by ensuring a private medical record-keeping database, also applicable to video consultations. 21 This functionality may contribute to building trust among patients who may exhibit concerns regarding the privacy and confidentiality of their consultations and personal information shared through telemedicine platforms, which may otherwise be unclearly ensured. 24 Considering a multidisciplinary approach involving specialized ophthalmologists in suggesting the management plan for patients would highly affect the quality provided by Telehealth platforms. 25
The various modalities developed in recent years enabled physicians to deal with high volumes of patients accurately and with great satisfaction, especially in the field of ophthalmology. 26,27 Skeptics are continuously questioning the quality of medical care provided by telemedicine, arguing that online consultation remains limited in comparison to physical consultation, especially in examining the posterior segment of the eye compared with the anterior segment. 28 Taking allsetbacks into consideration, patients and providers were motivated to use telemedicine considering its ease of use, low cost, and accessibility. 29
Teleophthalmology’s role is growing hand in hand with the development of new data transfer methods such as digital imaging of the anterior and posterior segments of the eye along with videoconferencing. 30 Chasan et al. conducted a study to find out the effect of diabetic tele-retinal screening on ophthalmical care outcomes, which concluded that tele-retinal imaging methods are effective for screening sight-threatening conditions, by measuring the agreement of the diagnoses between telescreening and face-to-face consultations. The agreement was 90.4%, and sensitivity was 73.6%. 31 Another study by Cook et al. looked at the impact of teleophthalmology on the diagnosis and outcome of ophthalmical conditions in South Africa. The impact on outcome was divided into general health and visual health, resulting in a 63% improvement in visual health and 39% in general health. 32
While the study represents the first analysis of accuracy in urgent referral worldwide and the first to analyze telehealth practice in the MENA region, with data spanning from 2018 to 2023, we identified several limitations in the conduct of our study. The study’s external validity may be compromised because of a potential geographical bias, given that the majority of the data sourced from Altibbi originates from the Kingdom of Saudi Arabia. Another limitation was that 355 patients who had a phone call consultation were excluded, as voice records were not available. Hence, we could not evaluate the management plans offered to this subset of patients and include it in the results demonstrated. In addition, the study only reflects the experiences of patients using Altibbi and does not necessarily represent the quality of consultations provided by all telemedicine platforms.
Further studies exploring other telemedicine platforms may expand the understanding of their effectiveness in detecting urgent ophthalmical conditions. In addition, the absence of access to ophthalmologists' final diagnoses poses a challenge in assessing the accuracy of telemedicine-based diagnoses. To validate the identification of red-flag symptoms through telemedicine, it is crucial to compare the preliminary diagnoses made by practitioners during consultations with the final diagnoses provided by specialists. Incorporating these confirmed final diagnoses into our analysis would enable a comprehensive assessment of the consistency between initial management plans and subsequent specialist evaluations, shedding light on potential misdiagnoses and uncertainties arising from telemedicine practices in ophthalmology. Future investigations should include final diagnoses obtained after telemedicine consultations to provide valuable insights into the reliability of telemedicine-based diagnoses.
Conclusions
In conclusion, despite this study’s demonstration on a telemedicine platform’s effectiveness in detecting red-flag symptoms in ophthalmical patients, it is essential to acknowledge that it only covers a single aspect of assessing the effectiveness of the platform. For a comprehensive evaluation of its impact, future research must consider additional factors such as patient satisfaction, clinical outcomes, affordability, accessibility, and the availability and efficacy of follow-up care. Telemedicine could become an invaluable tool for providing high-quality, accessible, and efficient health care services by implementing the aforementioned strategies and conducting further research.
To conclude, the findings of this study demonstrate, to a certain degree, the proficiency of general practitioners in a telemedicine platform in detecting red-flag symptoms indicative of retinal detachment among ophthalmical patients. Patients with positive symptomatology were significantly more likely to receive appropriate referrals, underlining the platform’s accuracy in identifying individuals needing more comprehensive evaluation by a specialist. There were no gender or age disparities in managing patients, highlighting equitable access to specialized health care provided by this platform. The findings presented in this study show that the use of telehealth in ophthalmology, specifically looking for the red-flag symptoms of retinal detachment, may be a feasible and successful adjunct to the original in-person ophthalmological consultation.
Footnotes
Acknowledgments
The authors thank Altibbi for their cooperation and sharing of data. They would also like to thank Abdullah Al-Ani, MD, for their help in statistical analysis.
Authors’ Contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by D.K.M., S.A.S., H.R., M.K., M.M.A., and S.A.A. The first draft of the article was written by D.K.M., S.A.S., H.A.R., M.K., and S.A.A., and all authors commented on previous versions of the article. All authors read and approved the final article.
Ethics Approval
To conduct this research, we obtained a Data Usage Agreement from Altibbi signed by both a representative of Altibbi and the corresponding author, allowing us to access and use consultation records. No IRB approval was indicated for this study as no patient identifiers were provided by Altibbi. The World Medical Association’s Declaration of Helsinki principles were followed to ensure ethical standards were upheld during the study. All the information included was collected with the patients’ consent and their awareness that it might be used for health care-related research purposes when creating an account with Altibbi.
Disclosure Statement
The authors report there are no conflicts of interest to declare.
Funding Information
The authors received no funding for this work.