
Abstract
Introduction
: The role of telemedicine should be reassessed in the post-COVID-19 pandemic era. This study aimed to evaluate the perception and satisfaction of medical staff with telemedicine after the COVID-19 pandemic and compare these findings with those during the COVID-19 pandemic.
Methods:
Between January and February 2023, a questionnaire regarding the utilization, safety, and satisfaction with telemedicine was administered to 200 medical staff members (100 doctors and 100 nurses). Additionally, open-ended questions were included to gather insights on the strengths, weaknesses, and prerequisites of telemedicine. The satisfaction levels of the medical staff were compared with those from a previous study conducted during the COVID-19 pandemic.
Results:
The response rate among medical staff was 60.0% (50 doctors and 70 nurses). Concerning patient safety, 83.3% of respondents indicated a risk of worsening symptoms in chronic patients, and 68.3% expressed concerns about emergencies related to patient safety. Eighty-two percent of doctors preferred in-person visits over telemedicine, while 48.6% of nurses reported equal or greater satisfaction with telemedicine (p = 0.003). The reported strengths of telemedicine included the convenience of outpatient clinics (67%), while its primary weakness was the incomplete assessment of patient conditions (73%). The likelihood of partial substitution of telemedicine for in-person visits was significantly higher in the post-COVID-19 pandemic period compared to during the pandemic (71.7% vs. 49.0%, p < 0.001).
Conclusion:
In the post-COVID-19 pandemic era, telemedicine continues to offer significant benefits in enhancing patient access to medical care. However, medical staff remain concerned about its safety and show lower satisfaction compared to in-person visits. In response to these concerns, an effective telemedicine platform and legal standards, including practical guidelines, should be developed.
Introduction
In December 2019, an outbreak of pneumonia of unknown origin occurred in Wuhan, the capital of Hubei province in China. A novel coronavirus, later identified as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was isolated from patients with virus-induced pneumonia. 1 This led to the designation of the disease as coronavirus disease 2019 (COVID-19) by the World Health Organization (WHO) in February 2020. 2 The unprecedented COVID-19 pandemic impacted all aspects of social, economic, political, and environmental life worldwide. One of the most severe challenges was the significant disruption of access to essential health care services. 3,4
In light of these challenges, telemedicine emerged as a viable alternative and was rapidly adopted globally. 5 In Korea, telemedicine was not legally permitted before the COVID-19 pandemic. However, in response to the crisis, the Ministry of Health and Welfare temporarily permitted telephone-based telemedicine in 2020. Despite initial reluctance from both patients and medical staff, who felt compelled to use telemedicine in urgent situations, more than 70% of the Korean general public eventually used or expressed an intention to use telemedicine. 6 However, despite its widespread adoption, in-person visits may still be preferred over telemedicine in the postpandemic period. 7 Therefore, it is crucial to reassess the role and future of telemedicine as the COVID-19 crisis subsides.
We previously published a satisfaction survey assessing the experiences of patients and medical staff with telephone-based telemedicine during a temporary hospital closure when in-person visits were restricted due to in-hospital COVID-19 transmission. 8,9 This study aims to evaluate the perception and satisfaction of medical staff with telemedicine after the COVID-19 pandemic and compare these findings with those during the COVID-19 pandemic at the same institution. Additionally, we evaluated the prerequisites and potential improvements necessary for the more effective implementation of telemedicine as we transition into the COVID-19 endemic phase.
Methods
Medical staff (doctors and nurses) from a single university-affiliated hospital participated in this study. A questionnaire was distributed to 200 medical staff members in the outpatient clinic (100 doctors and 100 nurses). Participants provided informed consent and completed the questionnaire upon agreeing to participate in the study. The survey was conducted between January and February 2023. During this period, telemedicine was permitted for patients who were medically stable and had previous visits to the hospital. Patients who desired telemedicine could arrange an appointment during a doctor’s outpatient clinic times. Telemedicine was conducted via telephone or video call applications without a standardized telemedicine platform. This study was approved by our Institutional Review Board (approval No. PC22QISI0231).
SURVEY QUESTIONNAIRE FOR MEDICAL STAFF
The questionnaire collected demographic information, including the department of the medical staff (medical or surgical), experience with telemedicine, current usage of telemedicine, mode of telemedicine (telephone or video), frequency of telemedicine (times per month), time spent per patient, reasons for discontinuing telemedicine, and reasons for not using telemedicine.
Additionally, nine questions were developed to assess two components of telemedicine: patient safety and medical staff satisfaction. The patient safety questions included: “Is an initial visit possible with telemedicine?”, “What is the possibility of worsening symptoms in chronic patients using telemedicine?”, “What is the likelihood of an emergency related to patient safety?”, and “Can video telemedicine help prevent emergencies?”. For medical staff satisfaction, the following five questions were asked: “How does the convenience of telemedicine compare with in-person visits?”, “How does communication in telemedicine compare with in-person visits?”, “Is there a possibility of substituting telemedicine for in-person visits?”, “How does satisfaction with telemedicine compare with in-person visits?”, and “What is your intention to use telemedicine in the future?”.
Similar to our previous study, open-ended questions were included to obtain medical staff opinions on the strengths and weaknesses of telemedicine and to identify prerequisites for its successful implementation.
COMPARISON OF TELEMEDICINE BETWEEN THE COVID-19 PANDEMIC AND POST-COVID-19 PANDEMIC
The medical staff’s satisfaction from the previous study was compared with that in the present study, which assessed satisfaction during the post-COVID-19 pandemic. Five questions regarding satisfaction with telemedicine were consistent across both studies. These questions included: “Possibility of an emergency related to patient safety,” “Convenience of telemedicine compared to in-person visits,” “Communication in telemedicine compared to in-person visits,” “Possibility of partially substituting telemedicine for in-person visits,” and “Intention to use telemedicine in emergency situations, such as during the COVID-19 pandemic.”
STATISTICS
Categorical variables from the questionnaire were compared using Pearson’s Chi-square test or Fisher’s exact test, depending on the expected frequency. Cronbach’s alpha coefficient was calculated to assess the internal consistency and homogeneity of the two components developed in this study. 10 Statistical analyses were performed using SPSS software (IBM SPSS Statistics, Version 26.0, Armonk, NY, USA), with a significance level set at 0.05.
Results
DEMOGRAPHICS OF MEDICAL STAFF WHO PARTICIPATED IN TELEMEDICINE
Fifty out of 100 doctors and 70 out of 100 nurses who participated in telemedicine responded to the survey, yielding a response rate of 60.0%. The demographic data of the medical staff are shown in Table 1. The current usage of telemedicine was 22.6% in the doctor group and 42.4% in the nurse group. Almost all medical staff (95.2%) used telephone-based telemedicine, and ∼80% spent <10 min per patient. The primary reasons for the discontinuation of telemedicine were the end of the COVID-19 pandemic (45.5%) and patient safety concerns (36.4%). The reasons for not using telemedicine differed significantly between doctors and nurses (p = 0.007), but after excluding nonresponders, the results were similar (p = 0.374). The most common reason was patient safety concerns (42.9%), followed by a lack of knowledge on how to use the technology (19.6%).
Demographic Characteristics of Medical Staff Using Telemedicine
p-Value was calculated after excluding nonresponders.
PATIENT SAFETY WITH TELEMEDICINE: COMPARISON BETWEEN DOCTORS AND NURSES
The two questions regarding the possibility of worsening symptoms in chronic patients and the risk of emergencies related to patient safety showed good reliability based on Cronbach’s alpha coefficient (α = 0.812). 11 However, two other questions (the possibility of an initial visit via telemedicine and the use of video telemedicine to prevent emergencies) were found to have unacceptable reliability (α = 0.473). 11 Ninety percent of the medical staff indicated that initial visits could not be conducted via telemedicine. The perceived risks of worsening symptoms in chronic patients and emergencies related to patient safety were 83.3% and 68.3%, respectively. However, 55.7% of nurses believed that video telemedicine could prevent emergencies, compared to only 36.0% of doctors. Overall, about half (47.5%) of the medical staff suggested the possibility of using video telemedicine to prevent emergency situations (Table 2).
Medical Staff Responses Regarding Patient Safety and Satisfaction with Telemedicine
SATISFACTION WITH TELEMEDICINE BETWEEN DOCTORS AND NURSES
The five questions regarding satisfaction with telemedicine were found to have good reliability based on Cronbach’s alpha coefficient (0.8 ≤ α < 0.9). 11 The perceived convenience of telemedicine differed significantly between doctors and nurses (p = 0.014). Sixty-eight percent of doctors preferred in-person visits over telemedicine, while nurses showed almost equal preferences for telemedicine (41.4%) and in-person visits (42.9%). Both groups indicated that communication was better during in-person visits compared to telemedicine. More than 60% of each group believed that telemedicine could partially replace in-person visits. Satisfaction with telemedicine differed significantly between the two groups (p = 0.003). Eighty-two percent of doctors preferred in-person visits over telemedicine, while 48.6% of nurses reported equal or greater satisfaction with telemedicine. Approximately 30% of medical staff indicated they would use telemedicine in the future, and 55% expressed an intention to use telemedicine in emergencies, such as during the COVID-19 pandemic (Table 2).
STRENGTHS AND WEAKNESSES OF TELEMEDICINE
The strengths and weaknesses of telemedicine, based on the medical staff’s responses to open-ended questions, are illustrated in Fig. 1 and Fig. 2. The strengths of telemedicine included convenience for outpatient treatment (67%), time-saving (14%), convenience for disabled individuals (13%), and prevention of disease transmission (6%), based on a total of 99 medical staff responses. The weaknesses of telemedicine included incomplete assessment of the patient’s condition (73%), miscommunication (14%), the absence of a standardized telemedicine platform (9%), emergency concerns (3%), and potential for medical disputes (1%), based on the responses of 100 medical staff members.
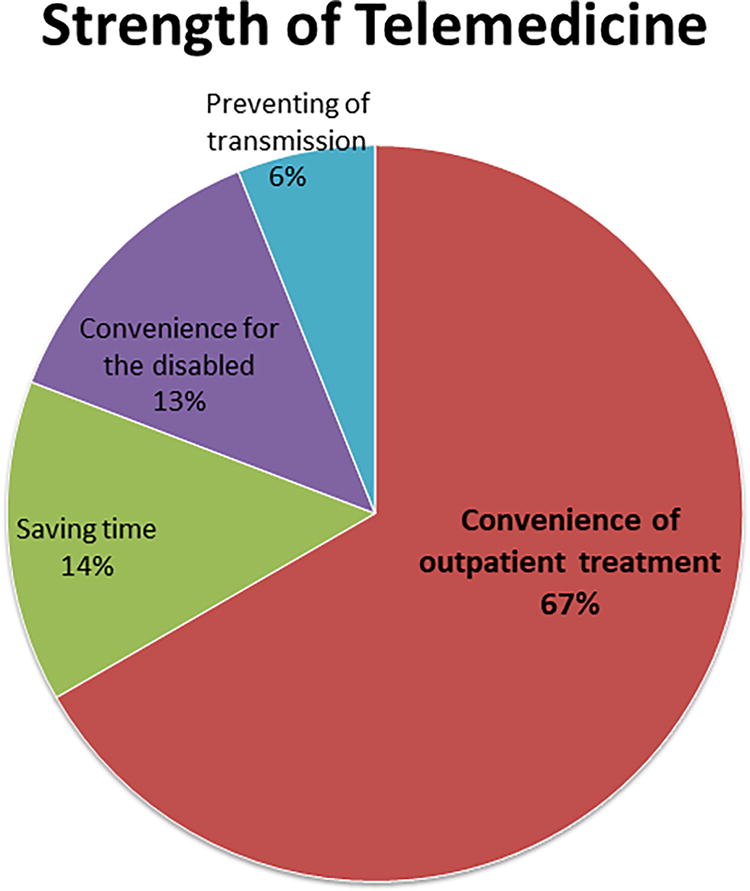
Strengths of telemedicine reported by medical staff (n = 99).
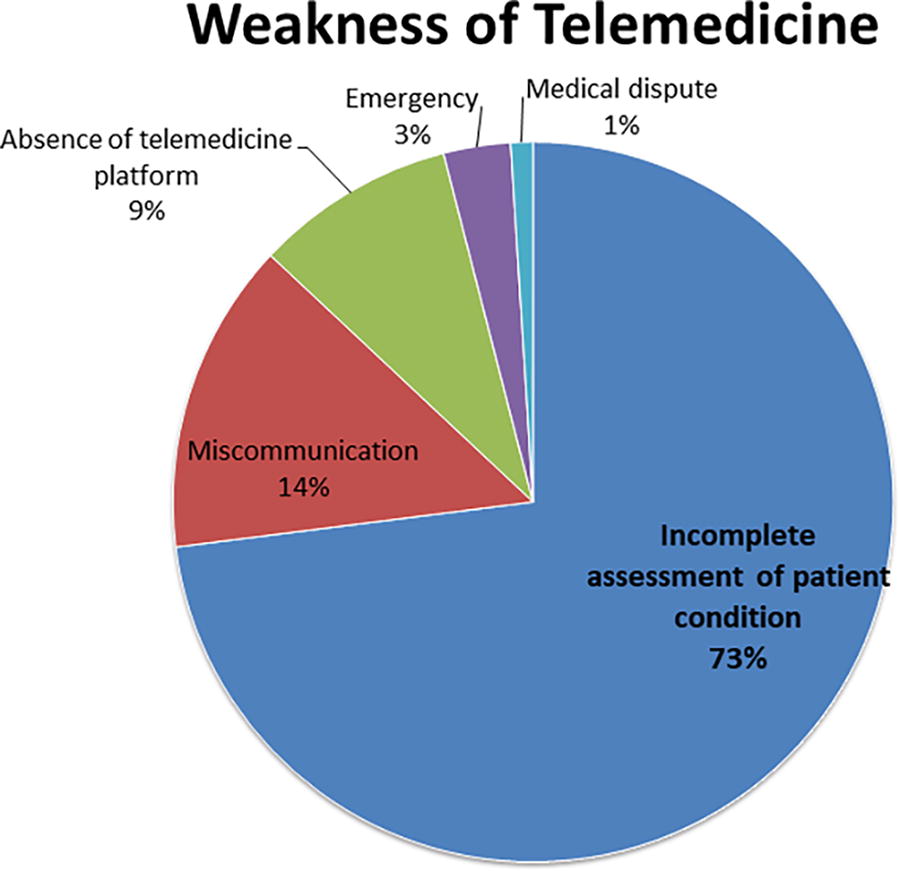
Weaknesses of telemedicine reported by medical staff (n = 100).
PREREQUISITES FOR THE APPLICATION OF TELEMEDICINE
The prerequisites for the application of telemedicine, based on a total of 76 medical staff responses, included legal standards (29%), a standardized telemedicine platform (29%), treatment guidelines (22%), limited use (11%), patient safety (5%), and protection of personal information (4%) (Fig. 3).
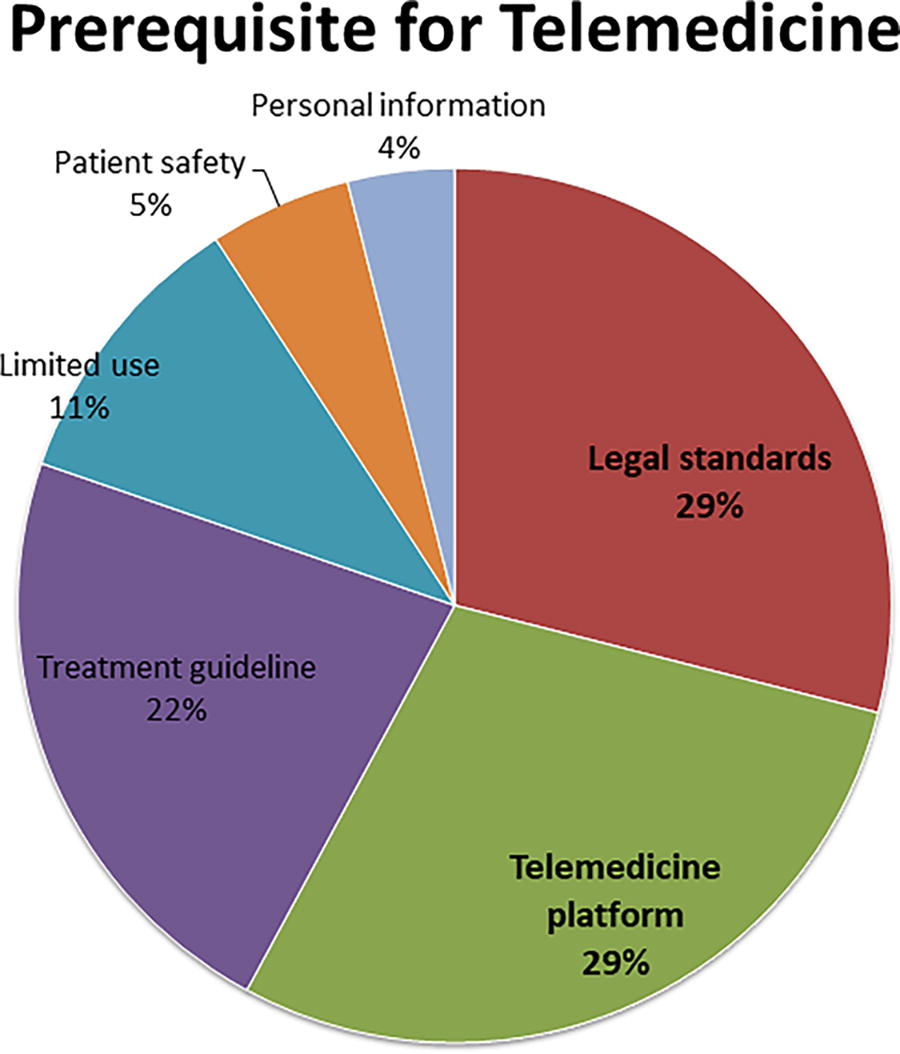
Prerequisites for telemedicine reported by medical staff (n = 76).
COMPARISON OF TELEMEDICINE BETWEEN THE COVID-19 PANDEMIC AND POST-COVID-19 PANDEMIC
A comparison of satisfaction with telemedicine between the COVID-19 pandemic and the post-COVID-19 pandemic is presented in Table 3 and Fig. 4. The possibility of an emergency related to patient safety, the convenience, and communication quality of telemedicine compared with in-person visits, and the intention to use telemedicine in emergencies, such as during the COVID-19 pandemic, were not significantly different between the COVID-19 pandemic and the post-COVID-19 pandemic (p > 0.05). However, the possibility of partially substituting telemedicine for in-person visits was significantly greater in the post-COVID-19 pandemic period than during the COVID-19 pandemic (71.7% vs. 49.0%, p < 0.001).
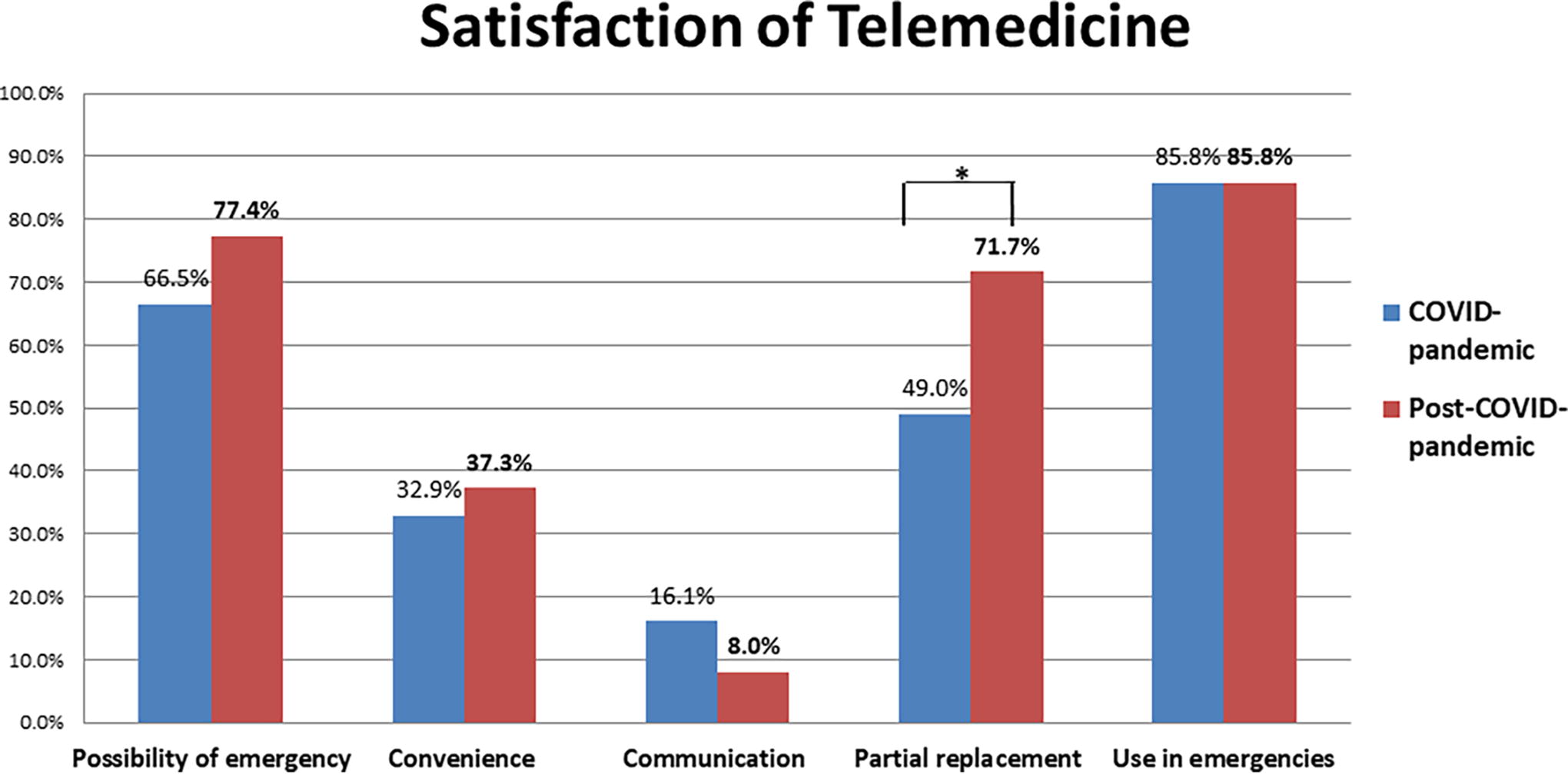
Medical staff satisfaction with telemedicine during the COVID-19 pandemic and post-COVID-19 pandemic periods.
Comparison of Satisfaction Between the COVID-19 Pandemic and Post-COVID-19 Pandemic Periods
Discussion
The COVID-19 pandemic has dramatically changed the paradigm of the medical system. 12 During the pandemic, telemedicine emerged as a practical and feasible option because health care resources were often unavailable due to the unprecedented situation. 13 However, as we transition into the COVID-19 endemic phase, the role and position of telemedicine should be reassessed. Additionally, it is necessary to review what needs to be supplemented or improved in this changed role. In this context, this study re-evaluated the efficacy of telemedicine during the post-COVID-19 pandemic, focusing on medical staff who had experience with telemedicine during hospital closures due to COVID-19 transmission.
Telemedicine has distinct strengths for patients. Medical staff in the present study identified the convenience of outpatient treatment, assistance for disabled individuals, and time-saving as key strengths of telemedicine. These results are consistent with our previous study. 8 Improved medical accessibility is one of the most critical advantages of telemedicine, as reported in numerous prior studies. 14,15 In the post-COVID-19 pandemic period, more medical staff indicated that telemedicine could partially replace in-person visits compared to during the COVID-19 pandemic (71.7% vs. 49.0%, p < 0.001). Additionally, 85.8% of medical staff expressed willingness to use telemedicine in emergencies, such as during the COVID-19 pandemic, both during the pandemic and in the postpandemic period. Beyond availability in situations where physical interaction is risky, telemedicine can also provide health care to patients in rural areas where quality treatment may otherwise be inaccessible. 16
However, concerns about patient safety with telemedicine persist among medical staff. Ninety percent of medical staff stated that an initial visit could not be conducted via telemedicine. The perceived risk of worsening symptoms in chronic patients and emergencies related to patient safety were approximately 80% and 70%, respectively. Additionally, 73% of medical staff suggested that the incomplete assessment of patients’ conditions is a significant weakness of telemedicine. An inaccurate assessment due to the lack of a comprehensive physical examination is one of the primary concerns associated with telemedicine. 17 Medical devices could serve as a valuable option to enhance patient safety. These devices can transmit vital signs and other data to physicians, enabling them to make informed treatment decisions. Furthermore, biometric data from wearable or remote monitoring devices, such as pulse oximeters or blood pressure cuffs, can be sent to physicians. 18 In chronic disease management, wearable devices have been reported to be effective in monitoring outcomes and improving adherence. 16 The rapid advancement of medical devices could significantly contribute to the safety and efficacy of telemedicine.
Telemedicine in Korea lags relatively behind, as Korean patients generally have good access to medical services. 19 Many aspects of telemedicine implementation in Korea still require development. In the present study, most doctors (95.2%) continued to use telephone-based telemedicine without a dedicated platform. Twenty-nine percent of the medical staff indicated that the development of telemedicine platforms was a prerequisite for effective telemedicine. The inferior convenience and communication associated with telemedicine, compared to in-person visits during both the COVID-19 and post-COVID-19 pandemic periods, could be related to the lack of an effective telemedicine platform. Although various commercial platforms were developed during the COVID-19 pandemic in Korea, they are primarily used for treating simple conditions such as the common cold, impotence, alopecia, and urticaria. 20 In contrast, Singapore’s Ministry of Health developed centrally managed telemedicine services during the COVID-19 pandemic, demonstrating that a nationwide, centralized telemedicine platform could be safe and effective as both a triaging tool and a medical consultation service. 21 Cloud-based platforms, in particular, can secure critical electronic health records and ensure data privacy. 22
In addition, developing legal standards and guidelines is an essential process to provide safe, efficient, and effective telemedicine. 23 Without clear standards, legal decisions might be guided by lawyers who may lack knowledge of telemedicine and potentially harbor biases. Guidelines are needed to educate users about the benefits and limitations of telemedicine and to provide evidence-based recommendations. 24 Furthermore, a reimbursement system is crucial for the broad adoption of telemedicine. In Korea, where national health insurance covers almost all medical costs for patients treated at any hospital, the government should engage in discussions with the medical community to establish appropriate reimbursement models. 25 These processes should be coordinated harmoniously with the medical profession, rather than being decided unilaterally by the government. 26
This study has some limitations. First, selection bias may have influenced the results, as medical staff interested in telemedicine were more likely to respond to the questionnaire. 27 The response rate of medical staff in this study was 60.0%. Second, the satisfaction survey focused solely on medical staff and did not include patients. Third, the results may vary depending on the hospital and surrounding conditions, as this study included medical staff from a single university-affiliated hospital. Therefore, further studies are needed to validate these findings, including patient satisfaction. Despite these limitations, a key strength of this study is that it is one of the few studies to assess changes in medical staff satisfaction between the COVID-19 pandemic and the post-COVID-19 pandemic period within the same institution.
Conclusions
During the post-COVID-19 pandemic, telemedicine has demonstrated strengths in providing patients with better access to medical care. However, medical staff still expressed concerns about the safety of telemedicine and reported lower satisfaction compared with in-person visits. To enhance the implementation of telemedicine in Korea, it is essential to develop an effective telemedicine platform, supported by medical devices that ensure patient safety, as well as legal standards, including evidence-based treatment guidelines. A significantly greater proportion of medical staff believed that telemedicine could partially replace in-person visits during the post-COVID-19 pandemic. Telemedicine has the potential to be a win-win solution for both medical staff and patients if its current limitations are adequately addressed.
Footnotes
Authors’ Contributions
Conceptualization: S.E.J. and H.Y.P. Data curation: Y.-M.K. and H.Y.P. Formal analysis: Y.-M.K. and H.Y.P. Methodology: S.E.J., S.Y.K., and Y.-H.K. Project administration: Y.-M.K. and H.Y.P. Supervision: S.Y.K. and Y.-H.K. Writing—original draft: S.E.J. and H.Y.P. Writing—review and editing: Y.-M.K. and H.Y.P. S.E.J. and Y,-M.K. contributed equally to this work as co-first authors.
Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This research was supported by Basic Science Research Program through the