
Abstract
Introduction:
Telemedicine can support home-based self-care for liver transplant recipients after discharge from the hospital. This study aimed to (1) provide an overview of the forms of home care for liver transplant patients; (2) identify the content elements of telemedicine in the home care of liver transplant patients; and (3) summarize the effect and outcome indexes of using telemedicine in liver transplantation patients.
Methods:
A search was performed in the electronic databases of PubMed, CINAHL, Web of Science, Cochrane Library, Embase, Google Scholar, CNKI, Wan Fang data and Wei Pu database through March 1, 2024. Subject heading and keywords were used to reflect the concepts of telemedicine, hepatic transplantation. Studies of tele-home care after transplantation in liver transplant recipients over 18 years of age and the form, content elements, and outcome assessments of telemedicine were included.
Results:
A total of 16 articles met the inclusion criteria, and from this, the application form of telemedicine in liver transplantation patients, intervention elements and evaluation outcome indexes were identified. The forms of application include internet platform, applications, network communication software, and portable devices; and the elements of intervention include telemonitoring, remote health guidance, telerecordings, teleconsultation, and telerehabilitation; and the outcome indicators include physiological indicators, psychological status, Quality of life, self-management ability, compliance, satisfactory degree, complication rate, readmission rate, and feasibility.
Conclusion:
Telemedicine is active and feasible in the home-based self-care of patients after liver transplantation, but its application is immature and there are still some problems.
Introduction
Liver transplantation, as an important treatment for irreversible liver failure, has the advantages of removing liver cirrhosis, cancer, and precancerous lesions. 1 With the development of medical technology, the safety and postoperative survival rate of liver transplantation have been greatly improved. 2 Liver transplantation increases the survival time of patients with end-stage liver failure and improves their physical function after surgery. 3 However, the majority of liver transplant recipients is affected by primary diseases before operation and need to take immunosuppressants 4 for life after operation. 5 Complications such as diabetes, hypertension, biliary complications, postoperative infection, 6 transplant rejection and tacrolimus drug toxicity 7 are easy to occur within 30 days after liver transplantation. 8
At present, the transitional care model after liver transplantation mainly includes outpatient follow-up, 9 telephone follow-up, 10 and home visit. 11 However, outpatient follow-up is under great pressure, telephone follow-up and home visits cost more, and the follow-up information collected is incomplete, which cannot fully meet the needs of liver transplant recipients after operation.
The World Health Organization defines telemedicine as: Under long-distance conditions, medical workers use communication technology and information to conduct research, evaluation, diagnosis, treatment, and prevention of diseases, so as to promote the health of individuals and the public. 12 In recent years, with the rapid development of network information technology and “internet + medical” services, telemedicine has been widely developed in the medical and health field. 13,14 At the same time, this field has gradually entered the practical application stage, including telemonitoring 15 and tele-emergence medicine, 16 teleconsultation 17 and treatment, 18 telemedicine guidance and other services. 19 At the same time, telemedicine has also been applied to chronic diseases 20 –22 and home care after organ transplantation 23,24 and has achieved good application effects. Especially during the prevention and control of COVID-19, 25 telemedicine has played a crucial role in providing diversified clinical nursing services for patients with chronic diseases, 26 –28 greatly alleviating the shortage of medical resources, due to its advantages of nonface-to-face medical treatment, 29 free from time and space restrictions in real life, monitoring and traceability. It improves the utilization of medical resources and reduces the risk of cross infection. 30
Studies have shown that telemedicine is helpful to improve the self-management ability 31 and immunosuppressant medication compliance of liver transplant patients, 32 thereby reducing complications 33 and improving the quality of life. Telemedicine also helps to relieve the travel pressure of recipients and reduce the risk of nosocomial infection in subsequent visits. 34 The form, content elements and outcome indicators of telemedicine applied to continuous care for recipients are not unified and clear, and there are great differences among different types of studies. This scoping review aims to review the main forms, content elements, and outcomes of telemedicine for liver transplant patients.
Methods
This study was conducted according to the Joanna Briggs Institute methodology for scoping reviews. 35 This scoping review of the literature, which has not been registered, was conducted using Preferred Items for Systematic Reviews and Meta-Analysis (PRISMA) (Fig. 1). 36
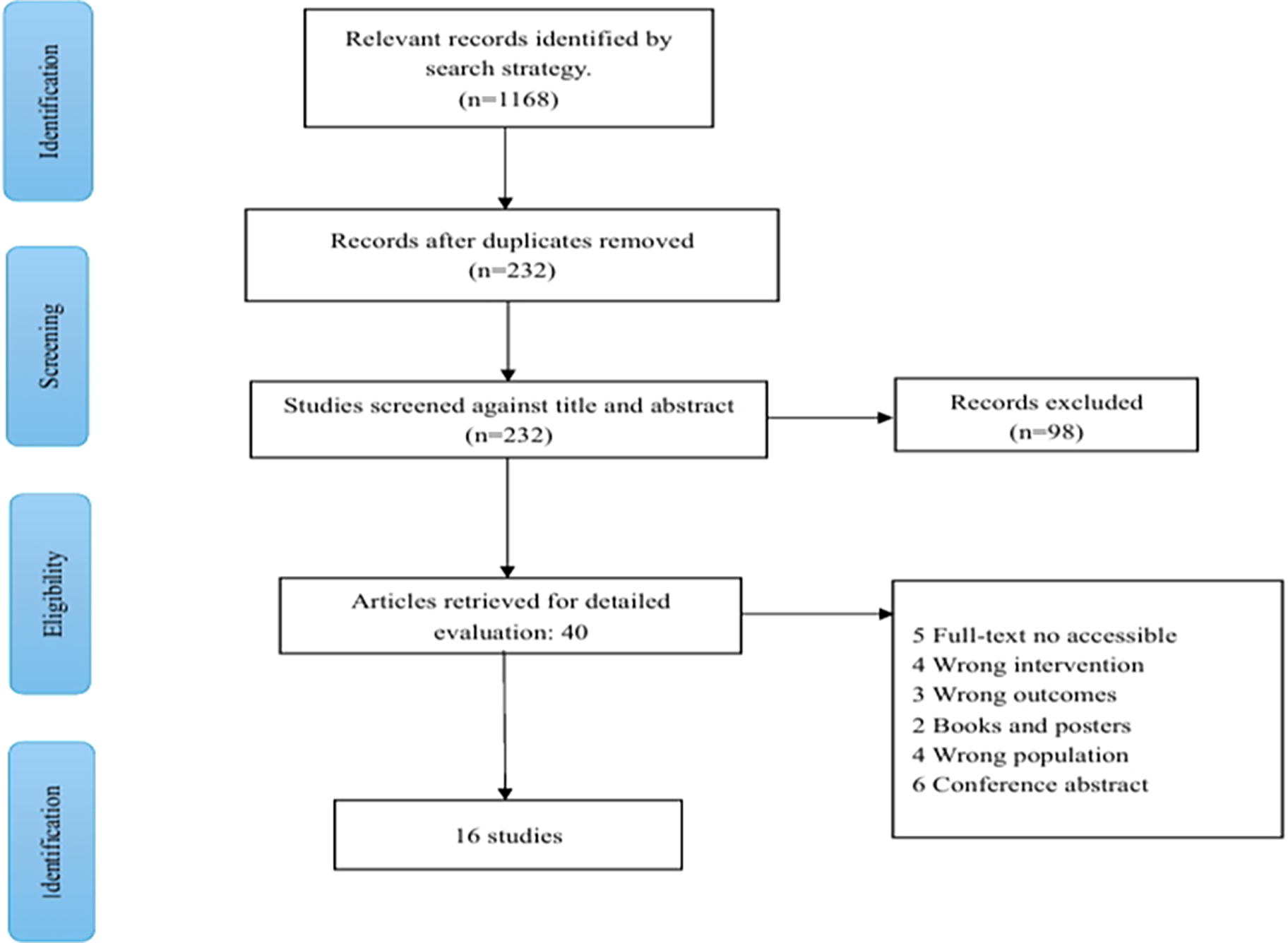
PRISMA—Literature selection process.
SEARCH STRATEGY AND SELECTION CRITERIA
The following four English databases and three Chinese databases will be searched: The PubMed, CINAHL, Web of Science, Cochrane Library, Embase, Google Scholar, CNKI, Wan Fang data, and Wei Pu data. The search terms will be based on two key terms, namely, “Liver transplantation,” “telemedicine.” The search field will be Title/Abstract. The language will be limited to English and simplified Chinese. The time period will be set as the day that the database was built to March 1, 2024. In addition, hand search will be performed for reference lists of the included literature.
DATA EXTRACTION AND SYNTHESIS
Information from the 16 articles was summarized in Table 1, which presented: (1) author(s)’ name, (2) Year of publication, (3) country of the study, (4) type of study, (5) sample size of control and intervention group, (6) the intervention methods of the control group, (7) patient reported outcomes, and (8) technology used in the study, duration and elements of the intervention group.
Characteristics of Studies Included in the Review
IG, Intervention group; CG, control group; QOL, quality of life.
Results
After preliminary search, 1,168 articles were obtained, 98 articles were selected by removing repetitive items, reading titles and abstracts, and 16 articles were finally included after reading the full text. The inclusion and selection details of the literature are summarized in Fig. 1. The main characteristics of the included papers are summarized in Table 1. All 16 manuscripts were original research published between 2016 and 2023.
INTERVENTION FORMS
The forms of telemedicine for continuous care of liver transplant recipients mainly include network information platforms applications, network communication software, and portable devices, specific descriptions are provided in Table 2. A total of eight studies used network information platforms to provide transitional care, including a doctor terminal app, patient terminal app, and management platforms—Wen Juan Xing platform to monitor health status and a WeChat public account to provide health guidance. 11,37 –43 A total of eight studies were supported by applications, which were installed on patients’ smartphones, 42 tablets, computers, 44 and other devices. 45 The application can record the development and changes of the patient’s condition, 46 and provide the appointment and follow-up service. 47 It can also be configured with alarm system, such as immunosuppressant drug miss alarm, 15 test critical value alarm, etc. In addition is supports online video communication between medical staff and patients and their caregivers, and provides health education such as rehabilitation exercises and drug taking methods. 48
The Forms of Telemedicine
A total of four studies used network communication software, using social media software such as WeChat and QQ to establish group chat, 42 relying on public accounts to carry out disease monitoring, peer support, health education and other work. 44 In addition, the use of Tencent conference, Facetime, and mobile phones facilitates online diagnosis and treatment, data collection, and other work. 5,46 A total of four studies used portable devices, with a wearable watch connected to an APP to remind patients to take their medication, 46 and tele-rehabilitation recipients equipped with aerobic steppers, resistance bands, and exercise pads. 38 Bluetooth technology 11 recorded and uploaded the health data obtained by electronic blood pressure (BP) monitor, oxygen saturation and heart rate (HR), body weight scale, and blood glucose (BG). 44
INTERVENTION ELEMENTS
The content elements of telemedicine for continuous care of liver transplant patients include telemonitoring, remote health guidance, telerecords, teleconsultation and telerehabilitation, details are described in Table 3. Twelve articles carried out remote health guidance, 11,39,41 –44,47,49 and the contents included disease knowledge, immunosuppressant medication, diet and nutrition knowledge, 37 wound care, 46 BG, mood and sleep management, sexual behavior, vaccination and skin cancer screening, 45 recognition and prevention of complications, and self-care skills. 38 Seven studies involved telemonitoring, 41,44 which monitored body temperature, BP, HR, blood oxygen saturation, 37 body weight, BG, 46 and electrocardiogram. BG and immunosuppressant use 11 were the key indicators of monitoring. Besides, infection alerts, 45 diet, sleep, gastrointestinal function, exercise, and T-tube drainage also important. 40
Contents of Telemonitoring and Remote Health Guidance Etc.
Patient heart rate (HR), systolic blood pressure (SBP), blood glucose (BG).
Eight studies remotely recorded the patient’s condition, including the patient’s name, age, temperature, systolic blood pressure, 11,42,46 skin color, diet and sleep, 14 psychological status, 37,41 medication use, fluid intake and discharge, 45 wound status, uncomfortable symptoms, 42 and the reason for readmission. Four studies conducted remote consultation, in which medical staff consulted by fax, text message, email, online video, and telephone, 5 which is generally used during public health emergencies, such as COVID-19. The consultation mainly included laboratory tests 5 and adjustment of immunosuppressive drugs. 15,40,45 Five studies provided telerehabilitation, with programs provided by transplant specialists and exercise physiologists 48 and consisting of aerobic step training and resistance training. 38,39 The specific rehabilitation content and skills were sent to the patients in the form of video, and the simple evaluation indicators were the number of steps, HR, sleep, and exercise capacity. 11,40
OUTCOME INDICATORS AND EFFECTS OF TELEMEDICINE
The outcome indicators and effects of telemedicine included 9 items, as listed in Table 4. First, three studies found that the weight, waist circumference, 38 BP, and BG of recipients were stable, 47 and their exercise capacity was enhanced after tele-rehabilitation intervention. 48 Besides, two studies used relevant questionnaires, including Hamilton Anxiety Scale, Hamilton Depression Scale, 47 self-rating anxiety scale and self-rating depression scale, 43 to propose that telecare on telemedicine platform had a positive impact on the psychological state. In terms of quality of life, four studies using the related quality of life questionnaire for liver transplant recipients, 43 such as SF-36 46 and SF-12v2, 38 showed that the quality of life of recipients was higher than that before surgery, but still lower than normal people. 40 In addition, six studies showed that telemedicine played a role in supervision and improvement of patients. 5,37,39,42,43,47
Outcomes of Telemedicine
6MWT, the 6-min walk test; SF-12v2, the 12-item Short Form Health Survey; MEDAS, the Mediterranean Diet Adherence Screener; BAASIS, Basel Immunosuppressive Drug Adherence Assessment Scale; ESCA, Exercise of Self-care Agency Scale; HAMA, HAMD: Hamilton Anxiety Scale; SAS, Self-rating Anxiety Scale; SDS, Self-rating Depression Scale.
Exercise of self-care Agency Scale Scores showed that self-care ability and self-management ability of patients had improved. Additionally, nine studies 5,49 indicated that the use of telemedicine intervention could improve the compliance of recipients in drug therapy, 45,47 self-monitoring and follow-up examination, 44 among which the Mediterranean Diet Adherence Screening 38 scale was used to investigate the dietary compliance of recipients. Basel Assessment of Adherence to Immunosuppressive Medications Scale 47 was used to evaluate the medication adherence. 42,43 About the satisfactory, eight studies pointed out that recipients and medical staff had high satisfaction with the carrier, content, method, system function, operation interface and process, and treatment method of condition changes of remote monitoring of mobile health. Only two studies included complication rate as an outcome measure. 47 Tian 40 pointed out that there was no significant difference in the incidence of major complications after liver transplantation between the two groups within 12 months of follow-up, but telemonitoring was beneficial for early identification of complications. Readmissions rates at 30 days 40 and 90 days 11,46 were also included as outcome measures.
Of course, feasibility affects patients’ willingness to use telemedicine. Six studies mentioned recipients’ acceptance rate, application mastery rate, and application completion rate and safety of app. 11,15,37 –39,41
Discussion
Studies have increased in the past five years. Although there are few studies, the existing evidence proves that patients after liver transplantation have a high acceptance of telemedicine in continuous care at home. 50 The occurrence of global public health events and the rapid development of mobile internet also accelerate the application of telemedicine in the field of liver transplantation.
LIMITATIONS AND FUTURE DIRECTIONS
The remote follow-up system requires professional information technology personnel to develop, debug and maintain. Mobile medical equipment and wearable equipment are expensive, and an excellent telemedicine team needs to receive systematic training. Therefore, the promotion of telemedicine in the continuous care of liver transplantation requires strong human, financial and material resources. 51 Therefore, it is recommended that the government provide technical and financial support to the team. Medical workers need to spend time outside work to guide patients on social media, which may increase the burden and cost of personnel. In the future, artificial intelligence robots can be introduced into social media to answer questions, 52 and machine learning can also be used to supervise patients’ punching in. Another, larger, challenge concerns the inconsistency and insufficiency of financial reimbursement and insurance coverage. 53
At present, most of the remote home rehabilitation programs for liver transplantation patients are universally applicable, that is, to improve the patient’s exercise capacity and resistance, but there is a lack of personalized evaluation of each recipient by rehabilitation doctors, personalized customization of rehabilitation programs and implementation feedback. 54 In addition, there are few studies that use patients’ psychological state as an outcome indicator, and liver transplant recipients are prone to negative emotions due to economic pressure and uncertainty about the prognosis. It is recommended to add real-time interaction content in telemedicine to improve the participation and persistence of patients, and promote the social regression and mental health of patients. The decline of physical function and the relative lack of electronic information skills of the elderly reduce their acceptance of telemedicine. 30 Therefore, the system design should adopt simple procedures, enlarged fonts, and the service content should be provided according to the different educational levels and electronic equipment literacy of the patients.
Few studies have focused on the standardization of services, legal supervision, data security, and privacy protection. Relevant state departments should issue relevant regulatory policies and service specifications for internet-based telemedicine, 55 such as the introduction of relevant laws to clearly define the scope of responsibility and access threshold of medical staff, so as to protect both doctors and patients. 56 The hospital-community-family cooperation model can be considered in future telemedicine, which is conducive to enhancing the confidence of caregivers and optimizing the allocation of medical resources. 57 In the future, the telemedicine team should include liver transplant specialists and nurses, information technology personnel, psychologists, rehabilitation doctors and nurses, and nutrition doctors. Multidisciplinary teams are more likely to meet the needs of patients. 58
There are some limitations in the current study. A lot of studies are quantitative studies with small samples and single center, and there is a lack of comprehensive, detailed and accurate high-quality longitudinal research and qualitative research. The evaluation indicators of telemedicine also need to be unified. The most used evaluation indicators are subjective indicators such as satisfaction, 59 compliance, and quality of life, and objective and unified evaluation indicators should be explored in future research.
Conclusions
This study summarized the main forms, content elements and outcome indicators of telemedicine. The results showed that telemedicine was positive and feasible in continuous care after liver transplantation. However, the current telemedicine system is still immature. In the future, comprehensive telemedicine strategies should be adopted under the guidance of relevant government laws and regulations, and the content of continuous nursing services should be expanded under the leadership of a multidisciplinary team to promote the early rehabilitation of liver transplantation patients and improve the survival outcome of patients.
Footnotes
Authors’ Contributions
R.G., J.Z.: Study conception. R.L., L.Z., S.F.: Data extract. All authors contributed to data analyses. R.G Drafting of the article. All of the authors approved the final version of the article.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.