
Abstract
Objectives:
To compare the health outcomes, specifically hospitalization and mortality rates, of primary care physicians’ referrals to the cardiology department for ambulatory assistance in heart failure (HF) over three clearly defined periods: before, during the electronic consultation program implementation (e-consult), and during the COVID-19 pandemic.
Methods:
Between 2010 and 2021, 6,859 HF patients were referred at least once. Of these, 4,851 received e-consultations, and 2,008 underwent single-act consultations. A time series regression model was used to analyze the impact of e-consult implementation (started in 2013) on all-cause, cardiovascular (CV), and HF-related hospital admissions and mortality rates.
Results:
e-Consults reduced the waiting time for cardiology care to 9 days. Hospital admissions decreased significantly after the implementation of e-consult (relative risk incidence [RRi] [95% confidence interval {CI95%}]: 0.867 [0.875–0.838] for HF, 0.838 [0.825–0.856] for cardiovascular disease, and 0.639 [0.635–0.651] for all-cause diseases), and mortality decreased (RRi [CI95%]: 0.981 [0.977–0.983] for HF, 0.977 [0.970–0.980] for CV, and 0.985 [0.984–0.985] for all causes). These improvements persisted during the COVID-19 pandemic.
Conclusions:
The implementation of the e-consult program for managing HF patient referrals resulted in reduced waiting times for cardiology care and decreases in hospitalizations and mortality rates. These benefits were maintained during the COVID-19 pandemic.
Introduction
For outpatient management, various telemedicine modalities have been developed in recent years. Electronic consultations (e-consults) facilitate asynchronous communication between primary care physicians (PCPs) and specialists, allowing PCPs to obtain expert opinions promptly. 1 Other public health systems report significant delays in ambulatory care. In England, where 92% of patients must wait no more than 18 weeks for a consultation, only 89.4% of patients were seen within this timeframe, an increase of 64.8% from the previous year. 2 In Northern Ireland, 71.6% of patients waited more than 9 weeks to see a specialist, an increase of 13.4%. 3
With e-consult models, waiting times are reduced to less than 6 days, and face-to-face visits are reduced. 4 These models present an alternative to traditional in-person consultations, which can often last over 4 weeks. 5
For heart failure (HF) patients, other telehealth models have shown beneficial effects on mortality and morbidity. 6 Accordingly, the 2017 European Society of Cardiology HF guidelines included a “may be considered” recommendation for home-based telemonitoring. 7,8 In HF programs, however, e-consult models have not been thoroughly evaluated for their impact on access to care and clinical outcomes. 9
Patients with HF are at high risk for clinical deterioration, requiring prompt assessment and treatment to prevent disease progression and hospitalizations. 7 Even though PCPs play an important role in managing these situations, specialist referrals are sometimes necessary. Preliminary data from our group suggest that an e-consult model that reduces waiting times might improve health outcomes by facilitating earlier decision-making and reducing emergency department visits.
This study aims to evaluate the impact of an outpatient care management program, incorporating a clinician-to-clinician e-consult system, on delay times in care, hospital admissions, and mortality in HF patients. We compared outcomes with those from the previous in-person consultation model and analyzed changes during the COVID-19 pandemic.
Methods
PATIENTS
Santiago de Compostela has a population of 450,000 people within its health care area. A single-act in-person consultation was instituted for all PCP referrals in 2008. An electronic consultation step was added to this program in 2013, resolving some referrals electronically and directing others for in-person consultations. 10 The characteristics and outcomes of this outpatient care program have been previously published. 10,11
An e-consult model uses a shared electronic health record that contains comprehensive patient data, including past consultations and test results (e.g., electrocardiograms, chest x-rays, and blood tests). During the e-consult, the cardiologist determines what type of consultation is appropriate for the patient: (1) resolving the issue without an in-person visit by documenting the response in the electronic health record or (2) scheduling an in-person single-act consultation. Postconsultation, patients are either referred back to their PCP or followed up in a specialized care program (e.g., for valvopathies, congenital heart diseases, HF, arrhythmias).
From 2010 to 2021, 6,859 patients with HF were referred by their PCPs. Three periods were analyzed: (1) in-person consultations (2010–2012), (2) e-consultations before the COVID-19 pandemic (2013–March 2020), and (3) e-consultations after the pandemic began (March 2020–December 2021). A 1-year prognosis was determined based on all-cause, cardiovascular (CV), and HF-related hospitalizations, as well as death due to all causes, CV, and HF. This study was approved by the local ethics committee on March 23, 2022, reference number 2021/496.
STATISTICS
Descriptive analysis
Qualitative variables were summarized as percentages, while quantitative continuous variables were presented as means (standard deviation [SD]) or medians (interquartile range [IQR]). Differences between groups were assessed by using the χ2 for categorical variables and the t-student for continuous variables. Statistical significance was set at p < 0.05.
Prognosis analysis
We evaluated all-cause, cardiovascular, and HF-related hospitalizations, as well as all-cause, cardiovascular, and HF-related mortality within 1 year post-e-consult. To determine the impact of the e-consult program and the onset of the COVID-19 pandemic on these outcomes, we used an interrupted time series (ITS) regression approach. 12 Predictors included time elapsed since study initiation (months), consultation type (0 for in-person; 1 for e-consult), and the interaction between time and consultation type. Overdispersion was accounted for and controlled. We estimated the relative risk incidence (RRi) with 95% confidence intervals (CIs) for each outcome across three periods.
Multivariate logistic regression
For each outcome, a multivariate logistic regression analysis was conducted. The model included patient characteristics (age, gender) and comorbidities (arterial hypertension, diabetes mellitus, ischemic heart disease, atrial fibrillation, cerebrovascular disease, peripheral arterial disease) that could influence prognosis. In addition, factors related to disease management (consultation type, number of emergency department visits within the first year after e-consult) and COVID-19 were considered.
Data analysis
Statistical analyses were performed using SPSS version 22.0 (SPSS Inc., United States), and ITS analyses were conducted with R version 3.5.1 and BayesX open-source software.
Results
OVERVIEW OF THE SAMPLE AND OUTCOMES
We analyzed 6,859 patients (2,008 during the in-person consultation period and 4,851 during the e-consult period). Of these, 49.6% were women. Patients in the e-consult period were older (78.5 [9.8] vs. 76.2 [9.2], p < 0.01) but had similar gender distribution (p = 0.149). During the e-consult period, patients had a lower prevalence of ischemic heart disease (HR [CI95%]: 0.80 [0.71–0.91]) and cerebrovascular disease (HR [CI95%]: 0.73 [0.61–0.88]), while other comorbidities were similarly distributed between groups (Table 1).
Clinical and Health Care Characteristics and Prognostic Events in the Sample by Care Models
aMean ± (standard deviation).
b1st year after the e-consultation.
cPercentages over the total number of deaths.
*Statistics: chi-square test, statistical significance at p < 0.05.
COPD, chronic obstructive pulmonary disease; CV, cardiovascular; HF, heart failure.
During the e-consult period, 27.2% of PCP referrals were resolved without an in-person visit, with cardiologists providing clinical notes in the electronic medical record; an additional 39.4% were resolved with a single in-person visit, and the remainder were scheduled for follow-up visits. In contrast, during the in-person consultation period, 62.1% of patients required ongoing face-to-face follow-up visits (p < 0.001).
The time to care after e-consult implementation was significantly reduced compared to the in-person period (8.6 [8.7] vs. 55.4 [79.9] days, p < 0.001). In the e-consult period, 66.4% of referrals were resolved within 7 days and 85.4% within 14 days, compared to 36.3% and 40.8%, respectively, during the in-person period (Table 1).
Post e-consult implementation, there was a significant reduction in emergency department visits within 1 year (HR [CI95%]: 0.07 [0.05–0.08]), all-cause hospitalizations (HR [CI95%]: 0.79 [0.77–0.82]), CV-related hospitalizations (HR [CI95%]: 0.91 [0.87–0.94]), and HF-related hospitalizations (HR [CI95%]: 0.88 [0.84–0.92]). Additionally, there was a significant reduction in all-cause mortality (HR [CI95%]: 0.85 [0.82–0.89]), CV mortality (HR [CI95%]: 0.87 [0.82–0.92]), and HF-related mortality (HR [CI95%]: 0.80 [0.74–0.87]) (Table 1).
MULTIVARIATE ANALYSIS
Table 2 presents the determinants for hospitalizations and mortality. Older age and male sex were independently associated with increased risk of hospital admission and mortality. Comorbidities such as diabetes, ischemic heart disease, and peripheral artery disease were also associated with higher risks, while hypertension was associated with a lower risk.
Multivariate Analysis of the Relationship Between Clinical and Health Care Variables with the Outcomes Analyzed
Bold data indicate statistically significant factors (p < 0.05).
CI, confidence interval; HF-r, heart failure-related; OR, odds ratio.
Emergency department visits during the year preceding the consultation (both in-person and e-consult) were linked to an increased risk of hospitalization and mortality, particularly for HF-related hospitalizations. Patients requiring in-person consultations, especially those needing subsequent follow-up visits, had worse outcomes compared to those whose e-consults were resolved without in-person visits. Patients referred for e-consults during the COVID-19 pandemic (2019–2021) had similar 1-year outcomes to those attended in previous years.
RESULTS OF INTERRUPTED TIME SERIES REGRESSION ANALYSIS
Delay from PCPs referral to cardiology consultation
During the in-person consultation period, there was a gradual reduction in delays, which significantly decreased following the implementation of the e-consult program (RRi [CI95%]: 0.56 [0.56–0.57]). Postimplementation, delays stabilized at less than 8 days, with minor fluctuations. Similarly, during the COVID-19 pandemic, the time to care was further reduced (RRi [CI95%]: 0.80 [0.80–0.81]) (Fig. 1).
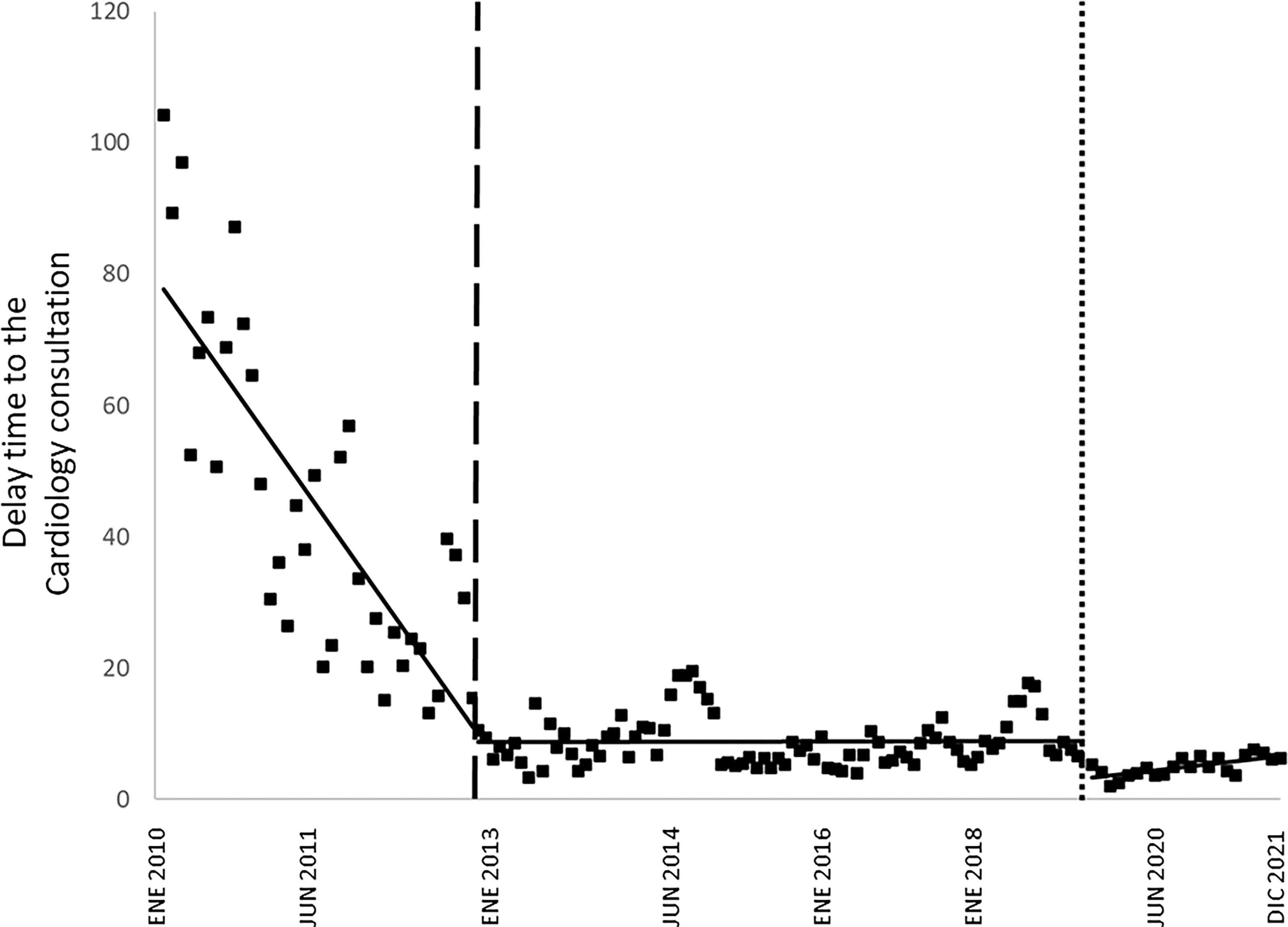
Analysis of the interrupted temporal trend of delay time in the three periods: in-person consultation, e-consult before COVID-19 and e-consult after the beginning of COVID-19 summary of estimated linear effects of the ITS model the delay time.
Hospital admissions at 1-year postconsultation
Within the first year after cardiology consultation, 758 patients (11.1%) experienced a total of 1,042 CV hospital admissions. The median time from cardiology consultation to first admission was 104 days (IQR: 34, 222), with a shorter duration during the in-person consultation period (67 days [IQR: 9, 170]) compared to after e-consult implementation (111 days [IQR: 39, 233]). ITS analysis demonstrated a significant reduction in CV hospital admissions following e-consult implementation (RRi [CI95%]: 0.838 [0.825–0.856]). All-cause hospitalizations and HF-related hospitalizations also decreased significantly (RRi [CI95%]: 0.639 [0.635–0.651]) and (RRi [CI95%]: 0.867 [0.875–0.838], respectively). During the COVID-19 pandemic, these rates were further reduced with the e-consult program (RRi [CI95%]: 0.985 [0.984–0.985] for all-cause hospitalizations, RRi [CI95%]: 0.977 [0.970–0.980] for CV hospitalizations, and RRi [CI95%]: 0.981 [0.977–0.983] for HF-related hospitalizations) (Fig. 2).
Mortality at 1-year postconsultation
Within the first year after cardiology consultation, 592 patients (8.6%) died. Table 1 summarizes the proportions of all-cause, CV, and HF-related deaths for the entire study period, including in-person and post-e-consult implementation phases. ITS analysis indicated a significant reduction in all-cause mortality following e-consult implementation (RRi [CI95%]: 0.809 [0.782–0.836]). Both CV mortality and HF-related mortality also declined significantly post-e-consult implementation (RRi [CI95%]: 0.860 [0.826–0.898] and RRi [CI95%]: 0.798 [0.750–0.858], respectively). During the COVID-19 pandemic, these mortality rates were further reduced with the e-consult program (RRi [CI95%]:0.883 [0.847–0.917]) for all-cause deaths, (RRi [CI95%]: 0.899 [0.859–0.940]) for CV deaths, and (RRi [CI95%]: 0.951 [0.904–0.990]) for HF-related deaths (Fig. 3).
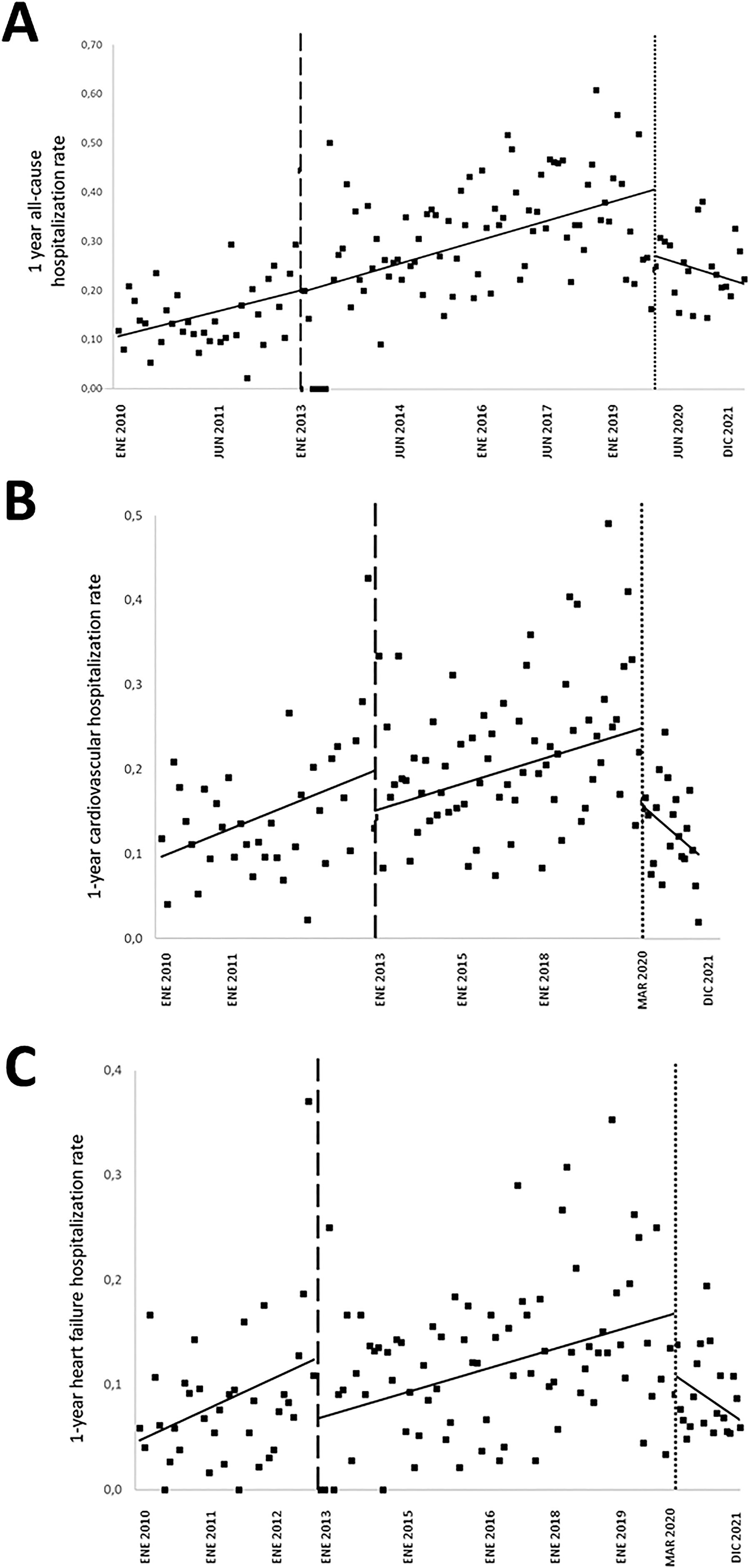
Analysis of the interrupted temporal trend of hospital admission in the three periods: in-person consultation, e-consult before COVID-19 and e-consult after the beginning of COVID-19.

Analysis of the interrupted temporal trend of mortality in the three periods: in-person consultation, e-consult before COVID-19 and e-consult after the beginning of COVID-19.
Discussion
Our study evaluated the implementation of a clinician-to-clinician e-consult program as the first step in managing HF in an outpatient setting, followed by in-person visits when necessary. Compared to the previous model of PCP referrals handled through a single in-person consultation, we observed a reduction in waiting times and an improvement in health outcomes. Regardless of the clinical characteristics of patients managed in-person or via e-consult, these benefits persisted. Even during the COVID-19 pandemic, our e-consult program maintained its positive results for these patient groups.
Based on an extensive literature review, the present study is the first to analyze waiting times and health outcomes of PCP referrals to cardiology departments using e-consultations. In addition, we evaluated the impact of the COVID-19 pandemic before and after e-consult to avoid bias.
According to our experience, e-consults can improve access and outcomes for HF patients referred by PCPs in health care systems with integrated electronic medical records. In contrast to the previous single-act consultation model, our e-consultation approach appears to counteract an upward trend in hospitalizations and mortality. We believe this improvement is due to the timely and effective risk stratification of patients based on clinical information provided by PCPs through e-consults, which is crucial for patients at high risk of clinical deterioration. The time elapsed until the first in-person consultation or resolution of the e-consult was an independent predictor of 1-year outcomes.
e-Consults enable us to identify at-risk patients earlier, enabling them to schedule and attend their first cardiology visit sooner. Patients with critical needs benefit most from prompt evaluations. There were approximately 25% of e-consults that were resolved without the need for an in-person visit, and this group of patients showed better outcomes than those who required an in-person visit.
Due to the large retrospective cohort of our study, we cannot establish direct causality, as other factors may have influenced our findings. Nevertheless, the ITS analysis provides robustness to our conclusions.
There is also evidence that telehealth models, such as remote patient monitoring, can prevent acute HF episodes by enabling early detection and treatment of deterioration, reducing emergency department visits, hospitalizations, and even mortality. 13 –16
A recent review by Liddy et al. highlights an increasing use of asynchronous, clinician-to-clinician electronic consultation services over the past 5 years. 17 The review lacked data specific to HF patients, and only three studies addressed mortality outcomes with mixed results. 15,18 –22
In a clinical trial involving 590 patients, Olayiwola et al. showed marked reductions in waiting times, in-person consultations, and emergency room visits. 23 Our findings have significant implications for health systems aiming to improve quality and reduce costs in managing HF patients. Cost reduction, quality improvement, and better care coordination may all be achieved with e-consults as the first step in PCP referrals. In a survey of patients and PCPs, the e-consult model was highly accepted. 10
The robust and consistent database supports the validity of our findings despite some limitations, including the retrospective nature of the data, unknown causes of death, lack of phenotypic classification of HF, and lack of data on private health care visits.
In conclusion, introducing clinician-to-clinician e-consult for HF patients before single-act consultations effectively reduces waiting times and improves 1-year outcomes. These results were consistent across different patient clinical characteristics and periods, including the COVID-19 pandemic. Our experience could help develop more efficient outpatient care pathways for HF patients.
Footnotes
Authors’ Contributions
S.C.S. has designed research/study, performed research/study, collected data, analyzed data, wrote article, and reviewed the last version. P.M.R. has designed research/study, performed research/study, collected data, analyzed data, wrote article, and reviewed the last version. M.A.B. has performed research/study and reviewed the last version. I.G.O. designed research/study, analyzed data, wrote article, and reviewed the last version. D.G.V. has performed research/study, collected data, and reviewed the last version. M.P.R. designed research/study, analyzed data, wrote article, and reviewed the last version. J.G.J. has designed research/study, performed research/study, collected data, analyzed data, wrote article, and reviewed the last version.
Data Availability Statement
Author Disclosure Statement
The authors declare no conflicts of interest related to this article.
Funding Information
The authors received no funding for the development of this study.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.