
Abstract
Background:
Patients with opioid use disorder (OUD) represent a high-risk population due to increased rates of adverse health outcomes and death. To evaluate whether telehealth utilization during OUD treatment compared with in-person encounters alone was associated with emergency department (ED) utilization, inpatient admissions, and mortality within three years of initiating buprenorphine.
Methods:
We conducted a retrospective cohort study within the Veterans Health Administration among Veterans treated for OUD between 2012 and –2022. The primary exposure was modality of care, characterized as telehealth encounters (with or without an in-person visit) compared with in-person visits only. Outcomes included an ED visit, inpatient admission, or mortality within three years of the index buprenorphine prescription. We measured the association between each type of treatment modality and outcomes through Cox proportional hazards regression modeling, adjusting for demographic and clinical covariates and confounders.
Findings:
Of the 57,021 Veterans diagnosed with OUD and who initiated buprenorphine, 38,072 Veterans met study eligibility criteria. The majority of Veterans were male, non-Hispanic White, 25–44 years of age, and lived in urban areas. Approximately 60% of this entire cohort experienced at least one ED visit, 40% experienced an inpatient admission, and 8% died during follow-up. Telehealth use compared with in-person visits only was associated with reduced ED visits (adjusted hazard ratio [aHR] 0.81; 95% confidence interval [CI] 0.77–0.85), inpatient admissions (aHR: 0.71; 95% CI: 0.67–0.76), and mortality (aHR: 0.80; 95% CI: 0.67–0.94).
Conclusions:
Telehealth may help overcome barriers to in-person care. During buprenorphine treatment for OUD, telehealth as a point of contact with providers and the health care system may reduce more adverse health outcomes, potentially through improving treatment retention. Qualitative studies may help shed light on the mechanisms through which telehealth directly impacts clinical outcomes.
Introduction
Opioid use disorder (OUD) has impacted over 3 million people in the United States (U.S.), leading to a national emergency declaration in 2017. 1,2 Those with severe OUD may experience poor general health, but other health consequences include infection, systemic effects, emergency department (ED) visits for overdoses, and mortality. 3 Mental health comorbidity is a concern due to experiencing depression, posttraumatic stress disorder, and personality disorders. 4 The Food and Drug Administration has approved three medications (buprenorphine, methadone, and naltrexone) for OUD treatment. 5 In addition, counseling and therapy sessions may be provided during treatment, particularly when concurrent mental health comorbidities are present. 6 Accessing counseling services in-person routinely may present logistical and financial challenges to the patient and may result in incomplete treatment and exacerbation of mental health concerns. 7
Telehealth facilitates provision and availability of mental health care while reducing logistical challenges. 8 While the Veterans Health Administration (VHA) was a pioneer in telehealth before the COVID-19 public health emergency (PHE), capacity rapidly expanded after to mitigate infection transmission. 9 Additionally, telehealth was not permitted for provision of buprenorphine prior to the PHE, though telehealth policies were relaxed to facilitate access to necessary treatment through expanded reimbursement for telehealth use, permission of audio telehealth use, and removal of the Ryan Haight Act requiring in-person contact before initiating buprenorphine. 10 –12 Previous studies in the pre-PHE era examining the role of telehealth for OUD among Veterans demonstrated that telehealth was associated with increased treatment retention with buprenorphine, 13 and that Veterans who initiated buprenorphine and stayed on this medication had a lower mortality risk. 14 However, there is still a gap in evaluating the clinical effectiveness of telehealth for OUD. First, the impact of telehealth services on clinical outcomes including ED visits and inpatient admissions (markers of clinical morbidity) and the direct relationship with mortality have been understudied. Second, it is not evident whether expansion of telehealth services resulting from the PHE translated to improved or comparable outcomes to in-person care. Third, while telehealth was increasingly adopted over time, there may be inequities in telehealth effectiveness within vulnerable subgroups. 15
Our primary objective was to evaluate the association between telehealth utilization compared with solely in-person visits and outcomes occurring within three years of buprenorphine initiation including ED visits, inpatient admissions, and all-cause mortality. We hypothesized that telehealth would be associated with lower risk of each outcome. Our secondary objective included investigating effect modification in the relationship between service modality (i.e., telehealth vs. in-person services) and clinical outcomes by (1) continued buprenorphine during follow-up and (2) Veterans’ demographic characteristics.
Methods
STUDY DESIGN, SETTING, AND SAMPLE
We conducted a retrospective cohort study of Veterans (ages ≥18 years) who initiated buprenorphine (with/without naloxone) between January 1, 2012 and December 31, 2022 within the VHA, using national administrative data from the Veterans Affairs Corporate Data Warehouse. 16 Eligibility included receipt of sublingual, short-acting buprenorphine within 6 months of an OUD diagnosis, determined by International Classification of Diseases—Clinical Modification Versions 9 and 10 (ICD-9, ICD-10). Exclusion criteria included Veterans who received buprenorphine patches, had a metastatic tumor diagnosis within two years of buprenorphine induction within the VHA, and those without geographical information. We excluded those who had an event (i.e., ED visit, admission, or death) on the same date as the index buprenorphine visit since the event may have preceded buprenorphine initiation. This study was approved by the local Institutional Review Board and VA Research and Development Committee and did not require informed consent. We report this study in accordance to the Strengthening the Reporting of Observational Studies guidelines. 17
MEASUREMENT OF TELEHEALTH AND IN-PERSON VISITS
We used the Decision Support System identifiers or stop codes from VHA outpatient encounters to classify telehealth services. Stop codes help identify the location for services, and those indicating mental health visits were first identified (i.e., codes 500–599). A second stop code indicating clinic-to-clinic or clinic-to-home video telehealth was used to identify telehealth visits, while the absence of these codes indicated in-person visits (Supplementary Appendix Table S1). Each encounter (whether telehealth or in-person) indicated a time-varying covariate based on individual use of health care services. While the frequency of visits required is not defined in the literature or guidelines and is unique to each Veteran’s needs, we were interested in those who sought mental health treatment and had at least one encounter every four weeks within the VHA as previously conducted and defined elsewhere. 13 Each encounter marked the beginning of a 28-day interval, and each subsequent visit within the 28-day interval reset the count to a new 28-day cycle. As telehealth visits only (i.e., no overlapping in-person visits) were relatively rare, we identified the following: telehealth (whether or not in-person visits also occurred in this window), in-person only, or no visits.
MEASUREMENT OF COVARIATES AND CONFOUNDERS
Sociodemographic factors assessed at baseline (i.e., index buprenorphine date) included age, race, ethnicity, gender, homelessness, and urban/rural designation status from the 2010 Rural-Urban Commuting Area codes. 18 Comorbidities and prior health care utilization were identified within the two years preceding the index buprenorphine prescription, defined from 2010 for the earliest cohorts initiating buprenorphine. We used the Quan coding algorithms to classify comorbidities and the Clinical Classifications Software coding scheme for additional mental health diagnoses. 19,20 We captured psychiatric medications prescribed in the year preceding the index buprenorphine prescription dichotomously. We classified buprenorphine status during follow-up as a time-varying covariate evaluated from the supply dates from each outpatient buprenorphine outpatient prescription through the number of supply dates. Similarly, in situations where Veterans may have transitioned to a different medication for OUD (MOUD) such as naltrexone or methadone, we included these medications as a composite “Other MOUD” category on any given day during the follow-up period.
OUTCOME ASSESSMENT
We identified three outcomes occurring up to three years from the index buprenorphine prescription within the CDW: an ED visit, inpatient admission, or mortality. ED visits were identified using stop codes from outpatient encounters, while hospital admissions were identified from the CDW inpatient domain. Mortality was evaluated using death and death date indicators.
STATISTICAL ANALYSIS
We evaluated the association between telehealth status and each outcome, while censoring records at the end of the study period (December 31, 2022) or the maximum follow-up period of three years if no event occurred. We measured the association between each demographic and clinical covariate and outcome through Cox proportional hazards regression modeling. Variables associated with the outcome, defined by a threshold of p < 0.2, were considered for the full model. We developed final multivariable models that included variables associated with the exposure and/or outcome to account for confounding of telehealth-related effect estimates. We did not compare telehealth or in-person visits with those who did not seek any treatment (i.e., had gaps in counseling services). This allowed us to limit the analysis to those who sought care within the VHA system rather than those who might have had some care outside of the VHA. Final selection of the models included evaluating Akaike information criterion values for the most parsimonious model and changes to the telehealth-related estimates. As we were concerned that telehealth could influence buprenorphine retention, which would subsequently impact each clinical outcome, we present associations from final models with and without adjusting for concurrent buprenorphine prescriptions. All analyses were completed using SAS version 9.4 (Cary, NC).
For our secondary objective, we evaluated whether key demographics (age, race, ethnicity, gender), pandemic stage (pre-COVID-19 era as prior to 2020 vs. COVID-19 era as 2020 to the end of follow-up), and buprenorphine status on any given day served as multiplicative effect modifiers in the relationship between telehealth and outcomes. Telehealth and buprenorphine status were defined as: telehealth (with or without in-person visits) and buprenorphine, telehealth and no buprenorphine, in-person visits only and buprenorphine, and in-person visits only and no buprenorphine.
SENSITIVITY ANALYSES
We performed several sensitivity analyses that addressed sampling concerns and exposure misclassification. New users within the VHA may not have had the opportunity to see providers during the two years preceding the index buprenorphine prescription and could have had incomplete comorbidity data. Therefore, we excluded Veterans with less than seven visits in the two-year period prior to starting buprenorphine. Second, Veterans who discontinued buprenorphine within 28 days were excluded to account for those who might not have had the opportunity to seek care via telehealth or could have initiated buprenorphine within the VHA and continued treatment outside the VHA. Third, we changed our exposure window of 28 days between treatment episodes to 14 days as there is no defined number of counseling visits or required days in between visits. Finally, as telehealth became the dominant method of health care delivery during the COVID-19 public health emergency, we evaluated the sensitivity to these changes by measuring the association in the pre-COVID-19 period and COVID-19 period.
Results
CHARACTERISTICS OF SAMPLE
Of the 57,021 Veterans who initiated buprenorphine, 38,072 met study inclusion criteria (Fig. 1). In the cohort, 92% were males, 46% were 25–44 years of age, and 78% were White (Table 1). Additionally, 20% of Veterans had an indicator of homelessness or unstable housing, 16% were from rural areas, and prevalent comorbidities included depression (78%), anxiety (68%), and concurrent dependence on alcohol (38%).

Flow Chart of Sample Selection and Final Analytical Dataset.
Demographic and Select Clinical Characteristics of Veterans Treated for OUD with Buprenorphine in the VHA and ED Visits, Inpatient Admissions, and Mortality Occurring Within 3 Years of Buprenorphine Initiation, 2012–2022
ED, Emergency Department; NSC, Not Service-Connected; PTSD, Posttraumatic stress disorder; SC, Service-Connected; VHA, Veterans Health Administration.
Demographic and clinical characteristics associated with ED visits and inpatient admissions were similar; younger age, Black race, and homelessness were associated with increased risk of health care utilization (Table 2). For mortality, males, older age, Black race, non-Hispanic ethnicity, and homelessness were associated with an increased risk of death during the follow-up period. The presence of clinical and psychiatric comorbidities was associated with an increased risk of all outcomes.
Association Between Demographic and Select Clinical Characteristics of Veterans Treated for OUD with Buprenorphine in the VHA and ED Visits, Inpatient Admissions, and Mortality Occurring Within 3 Years of Buprenorphine Initiation, 2012–2022
ED, Emergency Department; NSC, Not Service-Connected; PTSD, Posttraumatic stress disorder; SC, Service-Connected; uHR, Unadjusted Hazard Ratio; VHA, Veterans Health Administration.
ED VISITS
Nearly 60% (n = 22,525) of the cohort experienced an ED visit during the follow-up period (Table 2, Supplementary Appendix Table S2). Compared with those with in-person visits only, telehealth use was associated with a reduction in ED utilization (uHR: 0.67, 95% CI: 0.64–0.70) (Fig. 2). This association persisted in the final models without adjusting for buprenorphine (aHR: 0.81; 95% CI: 0.77–0.85) and with adjusting for buprenorphine (aHR: 0.84; 95% CI: 0.80–0.89). We observed evidence of effect modification by treatment modality and concurrent use of buprenorphine (p < 0.001); compared with those with in-person visits only and no concurrent buprenorphine, those with concurrent buprenorphine (with or without telehealth) and those with telehealth without buprenorphine had a lower risk of ED visits (Fig. 3). In stratified analyses, the association between telehealth and ED visits persisted among those who were 25–44 years, 45–64 years, and Veterans who were Black, White, Non-Hispanic, urban, and rural (Supplementary Appendix Fig. S1). Results were similar across sensitivity analyses, though the protective association between telehealth and ED visits was more prominent in the pre-COVID-19 period (aHR: 0.50; 95% CI: 0.45–0.55) compared with the COVID-19 period (aHR: 0.86; 95% CI: 0.80–0.92) (Supplementary Appendix Fig. S2).

Association between Telehealth and ED Visits, Inpatient Admissions, and Mortality. ED, Emergency Department.
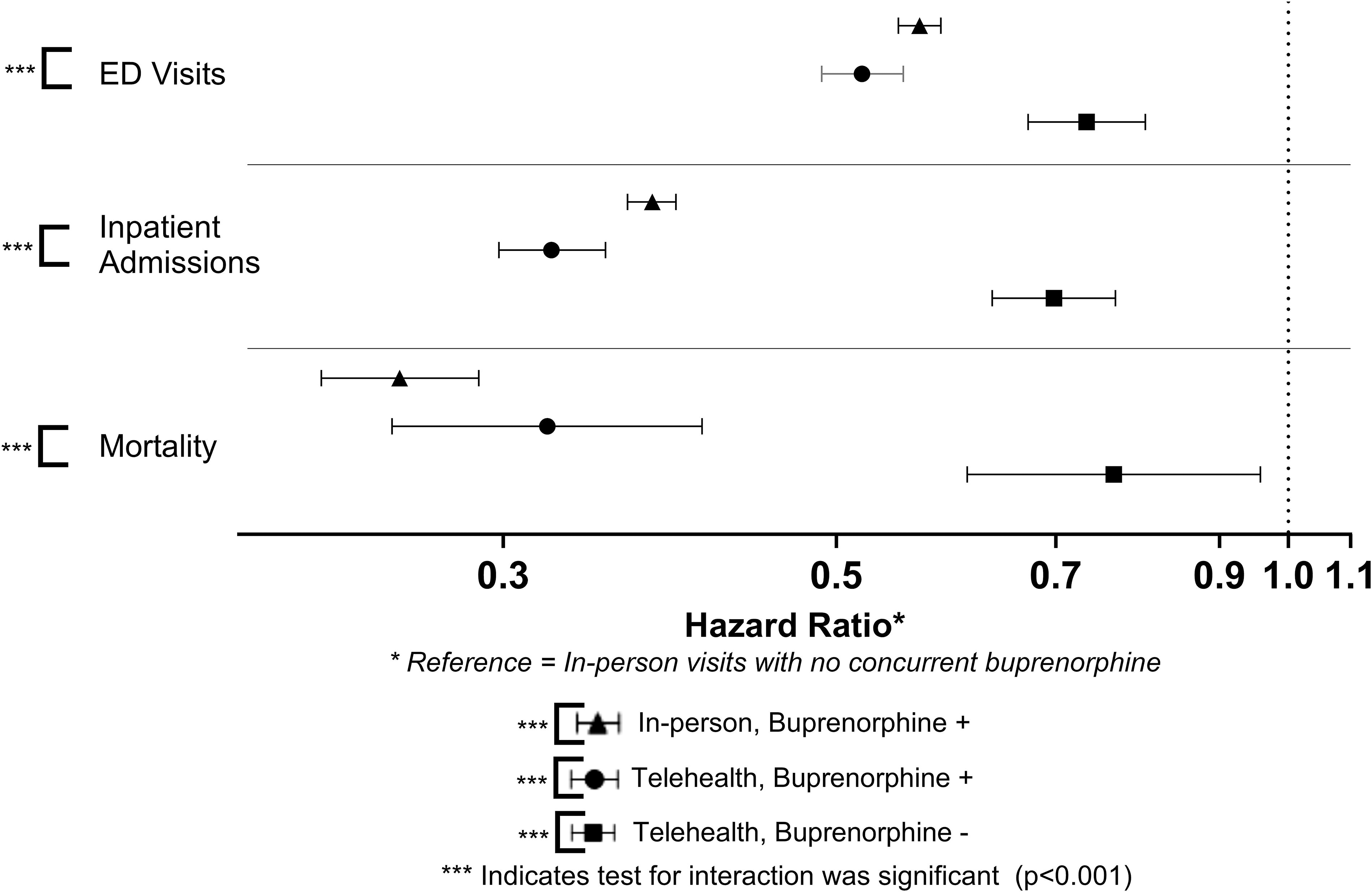
Association between Visit Type, Buprenorphine, and Outcomes.
INPATIENT ADMISSIONS
Approximately 40% (n = 15,269) experienced an inpatient admission during follow-up (Table 1, Supplementary Appendix Table S3). Telehealth was associated with a reduced risk of an inpatient admission in the unadjusted (uHR: 0.61; 95% CI: 0.57–0.65), the final models without adjusting for buprenorphine (aHR: 0.71; 95% CI: 0.67–0.76) and with adjusting for buprenorphine (aHR: 0.78; 95% CI: 0.73–0.83) (Fig. 2). As with ED visits, we observed evidence of effect modification by treatment modality and concurrent use of buprenorphine (p < 0.001); compared with those with in-person visits only and no concurrent buprenorphine, those with telehealth and concurrent buprenorphine and those with telehealth without buprenorphine had a lower risk of inpatient admissions (Fig. 3). In stratified analyses, the association between telehealth and ED visits persisted across all age-groups, and among Veterans who were Black, White, Non-Hispanic, urban, and rural (Supplementary Appendix Fig. S3). Results were similar across all sensitivity analyses, with no discernable difference between pre-COVID-19 (aHR: 0.67; 95% CI: 0.61–0.73) and the COVID-19 period (aHR: 0.71; 95% CI: 0.65–0.78) (Supplementary Appendix Fig. S4).
ALL-CAUSE MORTALITY
There were 2,842 deaths (7%) during follow-up (Table 2, Supplementary Appendix Table S4). Telehealth was associated with reduced risk of mortality in the unadjusted model (uHR: 0.71; 95% CI: 0.60–0.83), and in the final model without adjusting for buprenorphine (aHR: 0.80; 95% CI: 0.67–0.94); however, in the final model adjusted for buprenorphine, there was no significant association with mortality (aHR: 0.91; 95% CI: 0.77–1.08) (Fig. 2). When stratified by telehealth and buprenorphine status, there was evidence of effect modification (p < 0.001) as telehealth, when in combination with buprenorphine or not, was associated with lower mortality (Fig. 3). In stratified analyses, the association between telehealth and ED visits persisted among those who were White, Non-Hispanic, and urban Veterans (Supplementary Appendix Fig. S5). Results were similar across sensitivity analyses, with no discernable difference between pre-COVID-19 (aHR: 0.58; 95% CI: 0.39–0.85) and the COVID-19 period (aHR: 0.56; 95% CI: 0.42–0.73) (Supplementary Appendix Fig. S6).
Discussion
In this longitudinal, national assessment of telehealth incorporation treatment of OUD with buprenorphine, we observed decreased risk of ED visits, inpatient admissions, and mortality associated with telehealth compared with those who had in-person visits only. These findings are important for several reasons. First, Veterans experiencing each outcome in this sample was high (60% ED visit, 40% inpatient admission, and 7% death), suggesting a vulnerable and high-risk population that needs additional interventions and opportunities to improve clinical care. Second, these findings serve as indicators of clinical effectiveness of a telehealth care delivery model during treatment and will help guide researchers, patients, and clinical providers about treatment modalities while managing OUD.
There may be several explanations for why telehealth was associated with reduced risk of each outcome. First, telehealth may have additionally improved access to mental health specialist care, continuity of care, or medications by reducing logistical barriers and other challenges with in-person only care models. Concurrent therapy or engagement with counseling while maintaining buprenorphine may have positive impacts; a previous study examining trauma treatment for Veterans with OUD demonstrated increased buprenorphine treatment retention, 21 while another demonstrated that treatment options including medications, contingency management, naloxone delivery, and overdose education was associated with the greatest cost-saving reductions in OUD-related morbidity and mortality. 22 Claypool et al. demonstrated findings by simulating various OUD treatment strategies and found that a multifaceted approached that included telehealth (in addition to contingency management, ED initiation of buprenorphine, and training) was associated with increased cost-effectiveness and treatment duration. 23 Findings from our study also support additional measures and points of contact with clinical providers while maintaining buprenorphine for OUD treatment for clinical effectiveness.
Second, telehealth utilization during buprenorphine treatment for OUD was previously evidenced to be associated with increased treatment retention. 13 We found that Veterans who were still actively prescribed buprenorphine had lower risk for each outcome; however, among those who were not actively receiving buprenorphine, those with telehealth encounters still maintained a reduced risk of each outcome compared with those who had in-person visits only. This underscores the role that buprenorphine plays in independently mitigating adverse health outcomes, but that in the absence of buprenorphine, contact with clinical providers via telehealth may additionally prevent ED visits and inpatient admissions. These findings suggest telehealth may mediate treatment retention, which then would impact subsequent health outcomes. Methods that increase treatment retention with buprenorphine should be prioritized; other studies have consistently demonstrated that retaining patients on these medications decreases ED visits, 24 hospitalizations, 24 and mortality. 14 An area for future research includes studies that delineate the direct and indirect impact of telehealth-mediated pathways on clinical outcomes, particularly as we observed adjusting for buprenorphine use attenuated the telehealth-mortality association.
The observed findings may also be reverse-causal or subject to residual confounding in administrative data, such that telehealth influenced more positive outcomes including treatment retention which led to a decrease in other outcomes. All sensitivity analyses were comparable to the primary analyses, suggesting reverse causality or other methodological concerns may have been less of a concern. Despite statistically significant tests for effect modification between the care modality and select demographics, differences were not clinically meaningful. There may be two reasons for this; first, as this was conducted among those with OUD and who initiated buprenorphine within the VHA, some subgroups may have been underpowered to detect a clinically meaningful difference. Second, the distribution of other clinical and demographic covariates may have varied across subgroups, leading to similar effect estimates.
We found that rural/urban designation consistently demonstrated similar findings across all outcomes, which is consistent with previous studies. 13 This may be a result of selection bias, such that those who have OUD and have the opportunity to be treated within the VHA represent a treatment-seeking population with access to health care. Second, the VHA has increasingly expanded services to rural communities even prior to the COVID-19 pandemic. 25 –27 We observed more profound differences in ED visits in the pre-COVID-19. This may be a reflection of telehealth-related changes within the VHA and the onset of the pandemic; there was more widespread use of telehealth in the COVID-19 era as telehealth treatment became the new norm. 28,29 Comfort and acceptability may have increased with telehealth utilization during the pandemic, 30,31 and those who had more predominantly in-person care could represent the more severe cases.
There are a few limitations to this study. With administrative data, there may been exposure and covariate ascertainment misclassification; however, we noted that changing exposure and covariate methodologies through sensitivity analyses yielded similar results. Second, we did not distinguish between subtypes of telehealth utilization (e.g., group counseling, individual, and OUD vs. mental health), and there may be variability in outcomes due to telehealth-specific modalities. Despite this variability, we found that telehealth was associated with reduced ED visits, inpatient admissions, and mortality, suggesting that future work should delineate both the quality and type of telehealth care received. Third, these findings were conducted within the VHA, which may vary due to the health system and the population served. Finally, the study period includes pre-COVID-19 and COVID-19 time periods, a time with significant and sweeping shifts in population health, health care access, and care modalities. There may have been other exogenous contributors to the observed findings; however, we attempted to control for exogenous events or changes that may have impacted our study findings.
Conclusions
In conclusion, this study contributes to the growing body of literature that telehealth may effectively provide alternative care to those with OUD and reduce adverse outcomes. For future clinical and research practice, we need to evaluate quality of care through telehealth, patient- and provider-related perceptions, barriers to telehealth utilization, and telehealth-mediated pathways to clinical outcomes.
Footnotes
Authors’ Contributions
J.P.V.: Conceptualization, analysis, and funding. J.P.V., B.L.C., S.A., and R.M.: Developed the methodology. K.D.C., B.C.L., and R.M.C.: Statistical oversight and consultation. J.P.V.: Writing, and all authors critically appraised and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States Government.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by funding from the Office for the Advancement of Telehealth,
Supplementary Material
Supplementary Appendix Figure S1
Supplementary Appendix Figure S2
Supplementary Appendix Figure S3
Supplementary Appendix Figure S4
Supplementary Appendix Figure S5
Supplementary Appendix Figure S6
Supplementary Appendix Table S1
Supplementary Appendix Table S2
Supplementary Appendix Table S3
Supplementary Appendix Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.