
Abstract
Background:
The use of e-health interventions to promote physical activity (PA) among older adults has significantly increased in recent years. This review aims to comprehensively summarize the various e-health modalities and strategies used to encourage PA in aging adults.
Methods:
A systematic search of Medline, Embase, CINAHL, AMED, and PubMed databases was conducted to identify studies on e-health interventions targeting PA promotion in individuals aged 50 and older, published between 2012 and 2023. Information pertaining to study characteristics and e-health intervention specificities was extracted using a standardized data collection form. A narrative synthesis approach was employed to synthesize the data collected from the included studies.
Results:
Of 4,915 studies initially retrieved, 81 met the eligibility criteria. The findings reveal a diverse array of methods and interaction modes utilized to stimulate PA in aging adults, regardless of their medical conditions. Asynchronous methods such as web-based programs, mobile apps, and activity monitors were used in 71.6% of the studies and were most frequently employed for initiating behavior change components. Synchronous interaction modes mainly included videoconferencing and were predominantly featured in studies where real-time supervision and demonstration of exercises were integral to PA programs. There was a lack of information to guide the selection of the most effective e-health intervention format for motivating older adults to engage in regular exercise.
Conclusion:
This review underscores the versatility of e-health interventions, showcasing a wide spectrum of methods and interaction modalities. Future studies should compare these different modalities and methods while also identifying their barriers and facilitators. This will help in selecting the most suitable interventions for older adults.
Background
Physical inactivity ranks as the fourth most significant risk factor for global mortality, strongly contributing to the rise of noncommunicable diseases and chronic disorders. 1 The World Health Organization recommends at least 150 min of moderate-intensity physical activity (PA) per week. However, research indicates that a majority of the population, particularly older adults, fail to meet this guideline. 2,3 In older adults, physical inactivity is associated with a decline in both physical and cognitive abilities, as well as a reduction in overall quality of life. It also stands out as a key risk factor for adverse health outcomes and frailty. 4,5 It is, therefore, crucial to implement PA interventions promoting active lifestyle habits among older adults. To ease the active lifestyle habits, it is essential to understand and reduce the barriers related to PA practice in older adults.
Barriers to PA among older individuals encompass personal factors like health status, fear of falling, lack of time, and desire. 6 Additionally, there are environmental, structural, and organizational factors such as accessibility, safety, and expenses that contribute to difficulty in engaging in physical activities. 6 To overcome these barriers, strategies using e-health technologies (i.e., information and communication in support of health), including m-health (i.e., mobile wireless technologies for health), have been extensively used lately to promote PA by providing training, guidance, reminders, and motivation. 7 The use of e-health has received great interest, especially during the COVID-19 pandemic, where PA levels dropped drastically in older adults due to self-isolation and lockdowns. 8
Studies investigating e-health-based interventions targeting PA in older adults have employed a range of engagement methods, including synchronous (real-time) and asynchronous (decoupled) modalities, leveraging various technologies such as mobile applications, websites, and wearable activity trackers. Recent systematic reviews in this field have emerged, with several indicating promising outcomes for these interventions in terms of increasing PA levels and mitigating sedentary behavior among older adults, particularly in the short-term context. 9 –11 Furthermore, there is empirical evidence demonstrating improvements in physical function, reduced fall incidence, and enhanced overall quality of life attributable to these interventions. 12 However, not all systematic reviews have yielded definitive or unequivocal findings in this regard. 13
Despite the substantial body of literature available, previous reviews focused on a limited range of outcome measures, study designs, interventions, and control conditions, as well as on specific populations. This narrow scope may have resulted in an incomplete exploration of the various e-health interventions and methods employed for older adults.
Given the considerable potential of e-health interventions, it is essential to provide a comprehensive overview of the e-health strategies utilized to encourage PA in aging adults, as well as to identify any gaps in the existing literature pertaining to their application in this population and to suggest future research directions. Hence, the main objective of this review is to systematically categorize and summarize the diverse e-health modalities and approaches employed in the promotion of PA among aging adults. This study aimed to answer the following research question: What are the distinctive characteristics of e-health interventions utilized to stimulate PA in aging adults and how are they used?
Methods
This review uses a scoping review methodology according to the Preferred Reporting Items for Systematic Review and Meta-Analyses, Scoping Review extension (PRISMA-ScR) guidelines 14 as well as to Arksey and O’Malley methodological framework 15 (Supplementary Data S1). Scoping reviews provide a comprehensive summary of the existing literature on a particular topic, helping to identify gaps in current research and guide future work. 16
DATA SOURCES AND SEARCHES
A comprehensive literature search of various databases, including Medline, Embase, CINAHL, AMED, and PubMed, published from 2012 until February 2023, was carried out after consultation with an experienced librarian. Keywords and medical subject headings covering the review concepts, such as PA, elderly, and telehealth, have been used (Supplementary Data S2). In addition, a manual examination of the reference lists from the articles that were selected in the review was also performed.
STUDY SELECTION
Two independent reviewers, R.W. and P.B., assessed the retrieved articles for eligibility. Any conflicts or contradictions in the article selection were resolved through deliberation and agreement. A total of 4,915 articles were identified and meticulously examined to determine their eligibility. The selection method involved eliminating duplicates, verifying titles, and conducting a comprehensive evaluation of the whole text based on the specified inclusion and exclusion criteria.
INCLUSION CRITERIA
Studies that met the following criteria were included: (1) m-health/e-health interventions that implicated PA or physical rehabilitation; (2) aging adults above 50 years with and without specific conditions; (3) studies with or without a comparator/control condition; (4) reporting any health outcomes (e.g., PA, physical/cognitive/psychological function, and quality of life); and (5) published in 2012 and after.
EXCLUSION CRITERIA
The following were excluded: (1) abstracts, presentations, protocols, and reviews and (2) to ensure a certain level of advancement of e-health interventions employed, pilot studies, those with a focus on feasibility and involving a sample size of less than 20 participants, and qualitative studies were excluded.
DATA EXTRACTION AND SYNTHESIS
Four independent reviewers (R.W., N.K., M.C., E.L.-M.) extracted the data from the eligible studies to guide the analysis process using a standardized form that was previously tested by the study team. The form contained the following fields: first author, publication year, country, journal and impact factors, relative citation ratio (a measure of influence at the article level), 17,18 title, objectives, intervention’s description, study design, population, sample size, mean age, sex/gender percentages, intervention modalities and characteristics (e.g., intervention content, intervention delivery modality [i.e., synchronous/asynchronous], intervention delivery method [i.e., web platform, mobile app, and videoconferencing]), intervention duration, session duration, session frequency, follow-up duration, comparator, primary outcomes, secondary outcomes, primary outcomes categories, statistical analyses, key results, adverse events, discussion, and conclusion.
A narrative data synthesis was conducted, wherein a comprehensive summary of the studies that were included is presented and categorized into three distinct themes: (1) study characteristics and goals, (2) methods and features of e-health interventions, and (3) characteristics of e-health PA program interventions.
Results
Of the 4,915 research articles yielded from the search strategy, 81 full-text articles met our inclusion criteria and were included in this review (Fig. 1 for PRISMA flow chart).
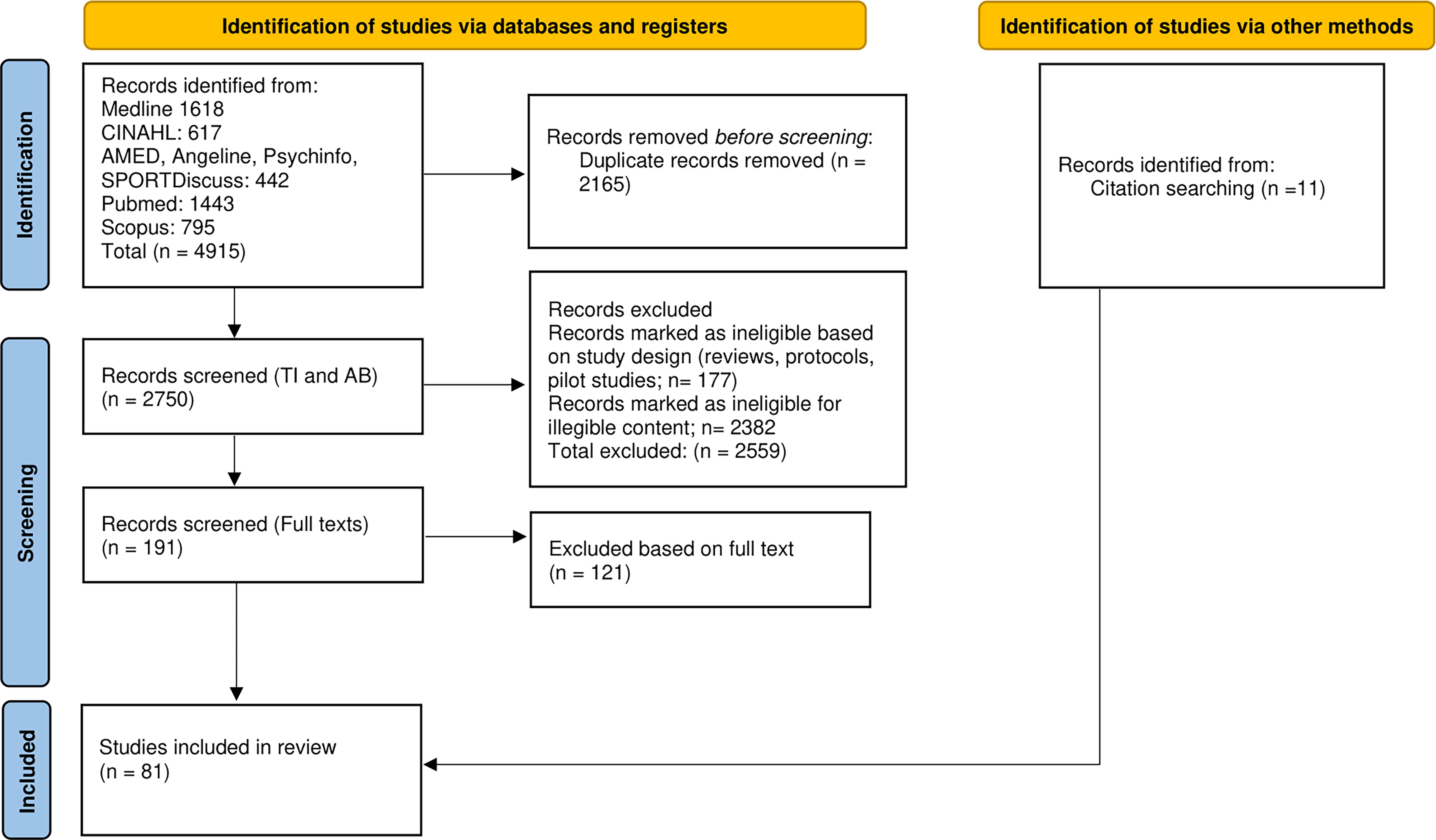
Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flow diagram.
STUDY CHARACTERISTICS AND GOALS
The characteristics of the 81 studies are summarized in Fig. 2 and Supplementary Data S3. Thirty-eight studies (46.9%) were published after 2020 vs. (n = 43, 53.1%) published between 2012 and 2019. Most of the studies were conducted in the United States (n = 23, 28.4%), The Netherlands (n = 9, 11.1%), Australia (n = 6, 7.4%), China (n = 5, 6.2%), Korea (n = 5, 6.2%), Germany (n = 5, 6.2%), Belgium (n = 4, 4.9%). Other publications were from Canada (n = 3), the United Kingdom (n = 2), Switzerland (n = 2), Turkey (n = 2), France (n = 1), Italy (n = 1), Ireland (n = 1), Greece (n = 1), Sweden (n = 1), Switzerland (n = 2), Saudi Arabia (n = 1), Malaysia (n = 1), India (n = 2), Cyprus (n = 1), Taiwan (n = 1), and Tunisia (n = 1), and two studies were multicenter (n = 2). Scopes of publishing journals included digital health (n = 20, 24.7%), aging (n = 17, 21.0%), behavioral medicine (n = 6, 7.4%) and PA and sports medicine (n = 5, 6.2%). Other scopes (n = 33, 40.7%) included public health, environmental research, and preventive medicine.

General characteristics of the included studies.
Relative citation ratios ranged between 0.08 and 13.91, with a median of 2.23. Most of the studies (n = 65, 80.2%) were RCTs, prepost design (n = 5, 6.2%), and quasi-experimental trials (n = 5, 6.2%). Other study designs included prospective longitudinal studies (n = 3), crossover (n = 1), and retrospective longitudinal studies (n = 2). Follow-up durations ranged between 12 days and 24 months. Populations included healthy older adults (n = 59, 72.8%) and those with specific clinical conditions (n = 22, 27.2%), with the most frequent conditions being older adults with obesity (n = 5), diabetes (n = 2), chronic obstructive pulmonary disease (n = 2), and cognitive impairment (n = 2). Study sample sizes ranged between 21 and 41,241, with a median sample size of 120 (interquartile range IQR1–IQR3: 50–243). Participants’ mean age was 67.7 ± 4.5 years, and 59.7% were women.
The included studies predominantly aimed to assess the effects/effectiveness of interventions (n = 74, 91.4%). Four studies focused on interventions’ cost-effectiveness and three others had various objectives, such as assessing adherence 19 or usability differences between age groups. Primary outcomes included functional (n = 60), physiological (n = 14), psychological/cognitive (n = 18), and quality of life (n = 7). Other outcomes included adherence, acceptance, self-efficacy, expectations, satisfaction, and knowledge (n = 21).
METHODS AND FEATURES OF E-HEALTH INTERVENTIONS
The modalities and methods used to deliver PA interventions through e-health technologies are summarized in Fig. 3 and Supplementary Data S4. Asynchronous (n = 59, 72.8%), synchronous (n = 12, 14.8%), and hybrid modalities using both synchronous and asynchronous methods (n = 10, 12.4%) were used. Synchronous modalities mainly included videoconferencing (n = 11/12, 91.7%). Asynchronous modalities encompassed web-based programs (n = 19, 32.8%), apps (n = 11, 18.6%), text messaging/emails (n = 3, 5.2%), activity trackers used alone (n = 2, 3.4%), and a combination of two or more of these methods usually joining an activity tracker or a health monitor (e.g., glucometer, oximeter) with an app or a website (n = 30, 51.7%). Other methods included exergames (n = 3), computerized interventions (n = 1), computer interactive controlled systems (n = 1), and tutorial videos (n = 1).

Modalities and methods used to deliver physical activity interventions through e-health technologies.
The interventions consisted of PA programs (n = 25, 30.9%), behavioral change strategies to promote PA such as counsel, instruction, feedback, and incentive (n = 44, 54.3%), and a combination of both (n = 12, 14.8%).
Synchronous modalities were frequently used in studies employing a PA program as an intervention (10 out of 12 studies using synchronous modalities). Similarly, apps were more often used for PA intervention studies (8 out of 10 studies using apps). On the other hand, web-based interventions (13 out of 19 using web-based intervention) and activity trackers used alone or combined with another method (23 out of 32 studies using combined methods or activity trackers alone) were more often used in behavioral change studies. Intervention durations ranged between 2 weeks and 24 months with a median of 12 weeks (IQR1–IQR3: 8–17 weeks). In 54.3% (n = 44) of the studies, equipment was provided to the participants; in 24.7% (n = 20), they used their own equipment (smartphones, tablets); in two studies, both provided and personal equipment was used. In 18.5% (n = 15) studies, it was not specified if the equipment was provided to the participants or not.
PA INTERVENTION CHARACTERISTICS AND RESULTS (n = 37)
The characteristics of PA programs and the results of studies employing PA programs with or without behavioral change components as interventions are presented in Fig. 4 and Supplementary Data S5. PA programs included several activities, such as balance, strength/resistance, stretch/flexibility, and cardiovascular exercises. The majority of the studies combined various exercise modalities (n = 31/37). Two studies focused on strength exercises, two on yoga, and two others on balance and functional exercises. The exercise intensity was not defined and was tailored to the individuals in most of the studies (21/37). Perceived exertion rating and predefined intensity levels (e.g., beginner, intermediate, and advanced) were the main methods used to tailor the exercise intensity. In a few studies, the exercise intensity was predefined as light (n = 1), moderate (n = 2), moderate to vigorous (n = 3) and vigorous (n = 1). The exact frequency of exercise sessions was not specified in 14 studies, and when reported, it varied between once a week and daily with a mean of 2.8 ± 1.6 times/week. Fifteen studies did not report the duration of exercise sessions, while in the remaining studies, the duration ranged from 10 to 80 min, with an average of 43.7 ± 16.2 min. Most studies used individual exercise sessions (n = 32, 86.5%), whereas a smaller proportion of studies implemented group exercise sessions (n = 2, 5.4%).

The characteristics of physical activity programs.
The findings of these studies regarding the effects of e-health interventions are summarized in this paragraph. e-Health interventions were considered superior to control conditions if at least one outcome improved significantly in the experimental group. Eight RCTs compared an e-health intervention with a traditional PA intervention(e.g., on paper/in-person programs). 19 –26 Among these, four RCTs reported positive results on physical function and adherence in favor of e-health interventions. 21,23,25,26 The four remaining RCTs showed that e-health interventions were as effective as traditional PA interventions. Sixteen RCTs compared e-health PA intervention with no intervention or standard/usual care. 27 –42 Among these, 13 RCTs reported positive results on physical function, 27 –29,31 –36,38,40 –42 psychological health, 30,37 and blood sugars 39 in favor of the intervention. Moreover, three RCTs compared the e-health PA intervention with another e-health intervention but without an exercise component (e.g., pedometer only or education). 43 –45 Three of these RCTs reported positive results in favor of the e-health PA intervention on physical and cognitive functions and quality of life. 43 –45
Moreover, three quasi-experimental studies showed positive effects on physical 46,47 and cognitive functions. 48 Similarly, four pre-post studies demonstrated significant improvements in physical and mental functions 49 –51 as well as lower back pain and quality of life. 52
Lastly, information on adverse events was lacking in most studies. Only 10 studies examined this aspect, and none of them reported any serious adverse events related to e-health interventions. 20,22,25,31 –33,35,38,43,45
Discussion
The aim of this review was to summarize the characteristics of e-health interventions used to promote PA among aging adults and to identify gaps in the existing literature pertaining to their application in this population.
The findings revealed a growing number of publications in the last 5 years. This finding may be due to the increasing use and acceptability of technology by older adults in the late years 53 and the COVID-19 pandemic. Acceptability to use e-health for PA interventions was assessed in two of the reviewed studies. 54,55 In one study, it was measured using the Computer Program Acceptability Scale, 53 while in the other, it was assessed through engagement (i.e., adherence). 54 Both studies reported good levels of acceptability. This positive feedback suggests that older adults are generally receptive to using e-health technologies for PA interventions.
The majority of studies included in the present scoping review were carried out in high-income nations, possibly attributed to the higher levels of internet and technology accessibility and familiarity in these countries. 31 However, most of these studies supplied participants with equipment or technology. This is an important finding since, even in affluent nations, limited household income and education might hinder the ability to utilize technology. 53
The study populations were heterogeneous, ranging from aging adults in good health (73% of the studies) to individuals with specific medical conditions. Furthermore, e-health interventions were employed either for overall physical fitness and wellness or for the aim of rehabilitation. The study outcomes included physiological, functional, and psycho-cognitive aspects. These findings highlight the broad range of applications and versatility of e-health in promoting PA among aging adults.
Regarding interaction modalities, asynchronous methods, including web-based programs, mobile apps, and activity monitors, were the most frequently used. Synchronous methods mainly included videoconferencing and were used predominantly in PA program intervention studies. It is worth noting that both types of engagement present their own merits and drawbacks. Asynchronous techniques may offer greater flexibility and convenience by enabling users to access information or PA programs at any time of the day. 31,56 This could enable older persons with chronic diseases to modify their exercise regimen based on their health variations. Asynchronous techniques could also be easier to adapt to different cultures and languages, which can be influential in reaching different communities. 54 Nevertheless, these approaches do not allow for direct interactions with the intervention provider. This lack of direct engagement might potentially impact the effectiveness of the intervention, as it may lead to misunderstandings, improper motions, or exercises that are not suitable for the individual’s level of fitness and specific characteristics. 57 Conversely, synchronous approaches enable immediate interactions and meticulous monitoring, resulting in higher engagement and improved adherence to the intervention, as demonstrated in a recent review. 57 They may also help build a relationship of trust and support between the intervention provider and the participants, which is important to older adults, as was demonstrated in a recent work. 58
While the information provided by the included studies is insufficient to determine whether one interaction modality is superior to the other, as only a few studies offered direct comparisons, the findings generally support the advantages of synchronous engagement for enhancing adherence and physical health. For instance, studies by Beauchamp et al. 31 and Granet et al. 56 found that synchronous groups had higher adherence, fewer dropouts, and better physical outcomes, which aligns with the results of a recent RCT. 59 On the other hand, the asynchronous group participants reported increased motivation probably due to strengthened feelings of self-efficacy as they had the ability to adjust training difficulty at their own pace. 56 Yerlikaya et al. also observed greater improvements in physical function in synchronous programs compared with asynchronous ones, suggesting that live guidance may help ensure proper exercise execution and adherence to the prescribed number of repetitions. 41 Taken together, these findings suggest that synchronous PA programs, especially group-based, can enhance adherence and health outcomes, while combining synchronous and asynchronous modalities may further boost motivation, engagement, and overall effectiveness.
Integrating e-health and in-person interventions as used in some of the studies reviewed 34 could also be a highly efficient and diverse strategy. Such a hybrid model harnesses the advantages of both e-health and in-person interventions, assuring intervention personalization, flexibility, and accessibility through e-health, while also providing safety, support, and long-term engagement through in-person interventions. By addressing key psychological components of the integrated behavior change model, 60 including autonomous motivation, self-efficacy, perceived behavioral control, and action planning, this approach could lead to a more comprehensive and effective intervention that meets the diverse needs of older adults and helps them engage in lasting PA. Future studies should assess the effectiveness and cost-effectiveness of such hybrid strategies to confirm their value in improving PA and overall health in older adults.
Regarding methods, diverse technologies with different levels of complexity were reviewed. However, the rationale for using one specific technology was not always pointed out by the authors. Indeed, some technologies may be better suited for achieving certain goals than others. For example, m-health apps, especially when synced to activity monitors, can provide more behavior change techniques, such as goal setting, self-monitoring, and rewarding, than other e-health technologies without significantly increasing cost or time. 13 Therefore, if the goal is to activate multiple behavior change components, mobile apps would be more effective than other e-health technologies.
Moreover, the level of complexity is an important consideration when using e-health technologies in older adults. For example, certain technologies, like immersive virtual reality, may require advanced digital skills that older adults may not possess, which may be a barrier to e-health adoption and adherence. In fact, a recent review concluded that simple e-health interventions were more feasible in older adults. 61 Similarly, Lavoie et al. identified the lack of computer skills and difficulties using the technologies as barriers to the use of web-based interventions in older adults. 58 It is therefore important to identify e-health technologies that are simultaneously accessible, usable, and effective in promoting PA for older adults. It may also be central for the adoption and successful use of these e-health technologies to put efforts into strategies and interventions to improve their accessibility and usability. This can be achieved by implementing digital literacy evaluation among study participants and offering training and support when needed. Assessing the effectiveness of such strategies in future studies could be of great importance.
Studies with PA programs frequently included multiple exercise modalities and exercise intensity was customized for each participant in most of the studies. Also, there was a lack of agreement over the frequency and duration of sessions. Hence, determining the ideal utilization parameters that could lead to improved outcomes is challenging.
Lastly, although the main objective of this scoping review was not specifically to evaluate the efficacy of e-health on health outcomes among aging individuals, certain overall trends emerged, suggesting that e-health interventions were successful in enhancing PA levels as well as physical and cognitive health outcomes. This tendency aligns with earlier studies that have also emphasized the efficacy of e-health PA programs. 9 –12 Lastly, there were no recorded instances of negative occurrences associated with the usage of e-health. These favorable results indicate that e-health interventions can be recommended as efficient and secure substitutes to traditional fitness programs for aging adults.
This review has some limitations. First, it may not have captured all the literature due to the research terms. However, our research methods were validated by a specialist and a hand search was conducted to complete the initial search. Second, we included adults over 50 years old, which allowed a larger number of relevant studies to be included. However, the results may not be generalizable to older populations (>65 years). Reviews focusing on older age groups are needed. Moreover, various designs, interventions, and control conditions were included, and the quality of studies was not assessed. While it wasn’t the objective of this review, this made it more difficult to synthesize information and draw conclusions regarding the effects of e-health interventions.
Conclusions
This scoping review underscores the growing interest in e-health interventions designed to promote PA among older adults. The increasing number of publications reflects a rising enthusiasm for harnessing technology to enhance the health and well-being of older populations. The review highlights the versatility of e-health interventions, offering a wide array of methods, modalities, and interaction modes. This diversity presents opportunities for tailoring interventions to individual needs, ensuring flexibility, and improving accessibility. The review also highlights certain gaps in the existing literature. Current studies often lack the comprehensive information necessary for selecting the optimal e-health intervention format. This includes considerations related to modality, method, and usage parameters for older adults. Future research should address this gap by offering insights into the rationale behind choosing one format over another and by reporting on the challenges faced, particularly those related to technology literacy and accessibility.
Footnotes
Authors’ Contributions
R.W.: Conceptualization and methodology (equal), formal analysis (lead), investigation (equal), writing—original draft (lead), writing—review and editing (equal). P.B.: Conceptualization and methodology (lead), writing—review and editing (equal). N.K., M.C., and E.L.-M.: Investigation (equal), writing—review and editing (equal). M.L. and M.A.-L.: Writing—review and editing (equal). All authors read and approved the final article.
Disclosure Statement
The authors declare that they have no conflicts of interest. M.L. holds a Tier 1 Canadian Research Chair in Social Participation and Connection for Older Adults (CRC-2022-00331; 2023–2030).
Funding Information
Funding from Fonds de recherche du Québec (FRQ) – Platform of Funding Programs for Intersectoral Research on Aging – Living labs (2021-2022) supported this work.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4
Supplementary Data S5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.