
Abstract
Objectives:
Telemedicine use increased substantially with the COVID-19 pandemic. Understanding of the impact of telemedicine modality (video vs. phone) on post-telemedicine acute care for higher risk conditions is limited.
Methods:
We conducted a retrospective study of telemedicine visits, comparing video with telephone, for selected diagnoses with potentially higher illness acuity, evaluating post-telemedicine emergency department (ED) and hospitalization rates. In a large, multicenter cohort of adult patient-initiated primary care telemedicine visits from March 1, 2020, to July 31, 2021, we evaluated 7-day ED and hospitalization rates for higher acuity diagnostic categories (cardiac, gastrointestinal, and respiratory) by telemedicine modality, provider familiarity, and patient sociodemographic and clinical characteristics.
Results:
Among 431,705 telemedicine encounters, 128,129 (29.7%) were video visits and 303,576 (70.3%) were telephone visits. Adjusting for patient and appointment factors, telephone encounters for cardiac conditions were associated with significantly higher 7-day ED visit rates than video encounters (5.5% vs. 4.9%, respectively) but similar hospitalization rates (0.7% vs. 0.8%, respectively); for gastrointestinal conditions, post-telemedicine adjusted ED and hospitalization rates were comparable between telemedicine modalities (4.0% for ED and 1.2% vs. 1.3% for hospitalization, respectively); among respiratory conditions, video encounters were associated with higher ED and hospitalization rates than telephone encounters (ED: 5.9% after video vs. 5.2% after phone; hospitalization: 1.9% after video vs. 1.5% after phone). Telemedicine encounters with patients’ own primary care provider (PCP) were associated with lower adjusted rates of ED use across all conditions and modalities.
Conclusions:
Short-term ED and hospitalization rates following primary care video or telephone visits for selected acute, high-risk conditions varied by condition and PCP familiarity. Nuanced use of video visits may confer benefits triaging to downstream acute care.
Introduction
As the COVID-19 pandemic emerged in early 2020, health systems across the United States shifted rapidly from predominantly office to telemedicine visits, with a dramatic increase in telemedicine visits in the first pandemic year. 1 –3 The move to telemedicine, driven chiefly by needs to limit infection exposure and spread while preserving access to care, has persisted beyond the pandemic. 1,4 Convenience, cost, efficiency, and reimbursement changes drive continued telemedicine use. 5 At the same time telemedicine access and use vary by race/ethnicity, poverty level, and digital connectivity, raising concerns of equitable access to care. 3,6 –11
With increased telemedicine use, optimizing rapport, comfort level, and risk tolerance while remotely managing potentially acute conditions is essential. Telemedicine modalities may confer varied visual and nonverbal information to aid in achieving these aims. While across a broad range of ambulatory care-sensitive diagnoses, a generally comparable likelihood of testing or emergency department (ED) use following primary care telemedicine and in-person visits has been observed, 12 focused evaluations of telemedicine for potentially serious diagnoses are limited and conflicting, and less is known about differences between video and phone care. 13 –15 During the pandemic, with office visits drastically curtailed, patients often had only the options of video or phone care, presenting a situation in which one could assess postvisit acute care differences between these modalities.
Video telemedicine may provide a different quality and quantity of information from phone visits and offer “face-to-face” connection 16 and is associated with higher clinician orders, including testing and medication, compared with telephone visits. 17 Phone visits may not provide the level of information available by video, so this may be more likely to be triaged to in-person care, whether in the office or ED. Among all-condition primary care telemedicine encounters during the early pandemic, subsequent in-person office visits, ED visits, and hospitalizations were all significantly lower after video compared with telephone visits. 18 Furthermore, video or phone modality may be especially relevant when patients see an unfamiliar primary care provider (PCP), as interactions are limited by the lack of in-person examination. Unfamiliar interactions, even when conducted in the same medical group and aided by comparable electronic health record access, may be associated with differences in postvisit ancillary testing and acute care use and modulated by visit modality. Continuity of care with one’s personal PCP is associated with mortality benefits and lower health care costs. 19 –22
Whether telemedicine modality can mitigate challenges of triaging patients with potentially high acuity conditions, by their own personal PCP or an unfamiliar PCP in the same practice, warrants investigation, especially as overall health care utilization, intensity of care (tests, imaging, and medications), and costs continue to increase, and telemedicine grows more common. 23
STUDY GOALS
In a large, diverse, multicenter cohort of adult patient-booked primary care telemedicine visits, we examined video and telephone encounters across three acute, potentially high-risk diagnostic categories (cardiac, gastrointestinal, and respiratory conditions), investigating the association of telehealth modality and PCP familiarity with short-term acute care (ED visits and hospitalization), adjusting for patient and visit characteristics.
Methods
STUDY SETTING
Kaiser Permanente Northern California (KPNC) is a large integrated health care delivery system providing medical care for over 4 million members, with approximately 1.2 million ED visits yearly. KPNC members include approximately 33% of the population in areas served and are representative of the demographic and socioeconomic diversity of the surrounding and statewide population. 24,25
KPNC providers use a comprehensive outpatient-inpatient electronic health record (EHR) and patient portal. Patient-initiated video and telephone telemedicine with patients’ personal PCP began in 2014 in KPNC, 26 and since 2016, patients scheduling a primary care appointment through the patient portal choose their visit type: office, video, or telephone. Patients can choose to see their personal PCP or another available PCP in the same practice. All PCPs conducting telemedicine visits have full access to the patient’s EHR history, and patients can receive telephone visits at any U.S. phone number and access video visits through any internet-connected and video-enabled computer or mobile device.
Due to social distancing measures starting in mid-March 2020, patients could only choose between a telephone or video visit when scheduling an appointment. In-office visits were only available on a physician’s recommendation after an initial telemedicine visit. These protocols continued during the initial study period; patients could self-book in-office visits for a limited range of concerns in the latter half of the study.
The KPNC Institutional Review Board reviewed and approved this study. Informed consent was waived because this was a data-only retrospective analysis.
STUDY POPULATION
We conducted a retrospective cohort study among KPNC health plan members aged ≥18 years who had a patient-initiated primary care video or telephone telemedicine encounter with a primary visit diagnosis of an acute cardiac, gastrointestinal, or respiratory condition from March 1, 2020, to July 3, 2021. To bring the focus to “new” or “acute” rather than short-term follow-up of recurring complaints, we excluded encounters with similar diagnoses in the prior three months.
We were specifically interested in ED and inpatient care following primary care telemedicine for undifferentiated acute, potentially high-risk conditions that may require urgent evaluation, and for which patients often seek emergency care, including encounters potentially related to COVID-19. To approximate the spectrum of diagnoses frequently managed in EDs, we included high-acuity diagnoses, acute exacerbations of chronic conditions, and potentially high-risk symptoms listed as diagnoses, such as chest pain or shortness of breath. To identify the candidate conditions, two emergency physicians (D.R.S. and M.V.K.) iteratively designed lists of diagnosis groups using International Statistical Classification of Diseases, Tenth Revision (ICD-10) 27 codes based on a review of emergency care literature. 28,29 The same two physicians reviewed all ICD-10 diagnosis subcodes to ensure they represented acute conditions and used a modified Delphi method 30 to ensure the appropriateness of the candidate conditions using a two-round process. We used the primary visit diagnosis for study inclusion. A full list of included diagnoses can be found in the Supplementary Table S1.
OUTCOME MEASURES
We evaluated each diagnostic category separately (cardiac, gastrointestinal, and respiratory conditions). For each primary care telemedicine index encounter, we identified subsequent post-telemedicine ED and inpatient encounters that occurred within 7 days. We included ED and inpatient encounters that occurred within KPNC using EHR data or at non-KPNC medical centers using claims data.
COVARIATES
To assess the association of primary care index telemedicine type (video vs. telephone) and physician type (personal PCP vs. other PCP) with downstream ED and inpatient encounters, we accounted for a broad set of patient and visit characteristics shown to be associated with visit-type choice 10 and higher ED utilization. 31 We electronically extracted sociodemographic characteristics (age, sex, race/ethnicity, primary language), comorbidity burden (Elixhauser comorbidity score 32 ), use of specific high-risk medications (immunosuppressants, chemotherapy), recent health care utilization (ED, inpatient encounters), use of the KPNC patient portal in the prior year, residential address to describe surrounding neighborhood socioeconomic status (neighborhood deprivation index), and neighborhood residential high-speed internet access level using census tract-level data. We also extracted time and date of initial appointment booking, time and date of appointment, and patient’s home facility.
STATISTICAL ANALYSIS
We examined the associations of index primary care visits that were (a) video vs. telephone visits and (b) with a personal PCP vs. other PCPs with 7-day ED visits and hospitalizations. We used modified Poisson regression models with generalized estimating equations (GEE) to examine these associations separately for each condition, unadjusted and adjusted for the above covariates at the population level, including variables associated in the literature with access to video vs. phone telemedicine care. 6 –10 The GEE models account for repeated visits and provide estimates of adjusted relative risks of the outcomes of interest. We analyzed the three conditions separately because of expected differences in acute management, need for ED referral, and impact of coexisting COVID-19 pandemic protocols (for respiratory complaints in particular). Because the time to booking was significantly longer for personal PCP appointments, we applied an interaction term (personal PCP vs. other PCP and time to booking) to the GEE model. To assist with interpretation, we calculated adjusted rates in addition to adjusted relative risks for outcomes using SAS’s least squares means postestimation technique. We analyzed each condition excluding early pandemic months (March, April, May 2020) as a sensitivity analysis, as the early pandemic was associated with substantial, rapid changes in access, care-seeking behavior, and care delivery protocols.
All analyses were conducted using two-sided tests for significance and with p < 0.05 as the threshold for significance. Analyses were performed using SAS, version 9.4 (SAS Institute Inc, Cary, NC).
Results
Among 431,705 primary care telemedicine encounters within the three clinical condition categories in the study period, 128,129 (29.7%) were video and 303,576 (70.3%) were telephone encounters. Mean age of study participants was 47.8 years (standard deviation, SD ±17.5 years) and 58.3% were women. In terms of race and ethnicity, 18.0% were Asian, 7.4% were Black, 40.8% were non-Hispanic White, and 24.7% were Hispanic; 74.1% identified English as their primary language. Most study cohort patients had at least one telemedicine encounter in the past year (84%), and 92.1% accessed the online patient portal in the past year. Of included telemedicine encounters, 68,266 (15.8%) had cardiac diagnoses, 207,706 (48.1%) had gastrointestinal diagnoses, and 155,733 (36.1%) had respiratory diagnoses. See Table 1 for a full cohort description.
Characteristics of Patients with Telemedicine Visit for Cardiac, Gastrointestinal, or Respiratory Condition from March 1, 2020, to July 31, 2021
All observed differences between means (continuous variables) and proportions (categorical variables) for each characteristic between video and telephone visits were statistically significant at p < 0.05.
NDI, neighborhood deprivation index; PCP, primary care physician; SES, socioeconomic status.
ENCOUNTER MODALITY
Video visits were 2.8% of telemedicine visits in March 2020 and increased sharply during the first 3–4 months studied, stabilizing at 36% for the remainder of the study. Patients booking telephone encounters were more likely to be older, non-White, from neighborhoods with lower socioeconomic status and less digital connectivity, and to have higher comorbidity burdens and greater prior ED and hospital utilization compared with patients who booked video encounters (Table 1).
TIMING OF ACCESS TO CARE
Patients accessed primary care telemedicine appointments within 12 h of booking in 53.7% of included visits (43.9% for video and 57.8% for telephone). Over half of telemedicine encounters (52.4%) were with patients’ personal PCPs; mean times from patient-initiated booking to video and telephone appointments with one’s personal PCP were 24.0 h and 18.2 h, respectively, versus 5.3 h and 3.0 h, respectively, for video and phone appointments with another PCP.
DOWNSTREAM ED VISITS AND HOSPITALIZATIONS
Overall unadjusted 7-day ED visit and hospitalization rates after telemedicine visit were 5.6% and 1.1%, respectively. Cardiac conditions had the highest 7-day post-telemedicine ED visit utilization rates at 7.1%, compared with 5.7% for gastrointestinal and 4.7% for respiratory conditions (see Supplementary Table S2). Cardiac conditions had lower rates of hospitalization (0.6%) versus gastrointestinal (1.4%) and respiratory conditions (1.0%). Fig. 1 displays time from telemedicine encounter to subsequent ED visits with most occurring within 12 h.

Fig. 2 shows adjusted 7-day ED and hospitalization rates by condition, comparing telephone and video encounters. In models adjusting for patient and visit characteristics including time from booking to appointment, personal versus unfamiliar PCP, and sociodemographic variables and comorbidities, video visits were associated with lower 7-day ED visits for cardiac conditions (4.9% vs. 5.5%) but higher 7-day ED visits for respiratory conditions (5.9% vs. 5.2%) compared with telephone visits. For gastrointestinal conditions, there was no significant difference in 7-day ED visits (4% for both video and telephone encounters). Adjusted 7-day hospitalization rates were not significantly different for phone or video encounters for gastrointestinal and cardiac conditions, but for respiratory conditions, video visits were associated with higher 7-day hospitalization rates (1.9% vs. 1.5%).
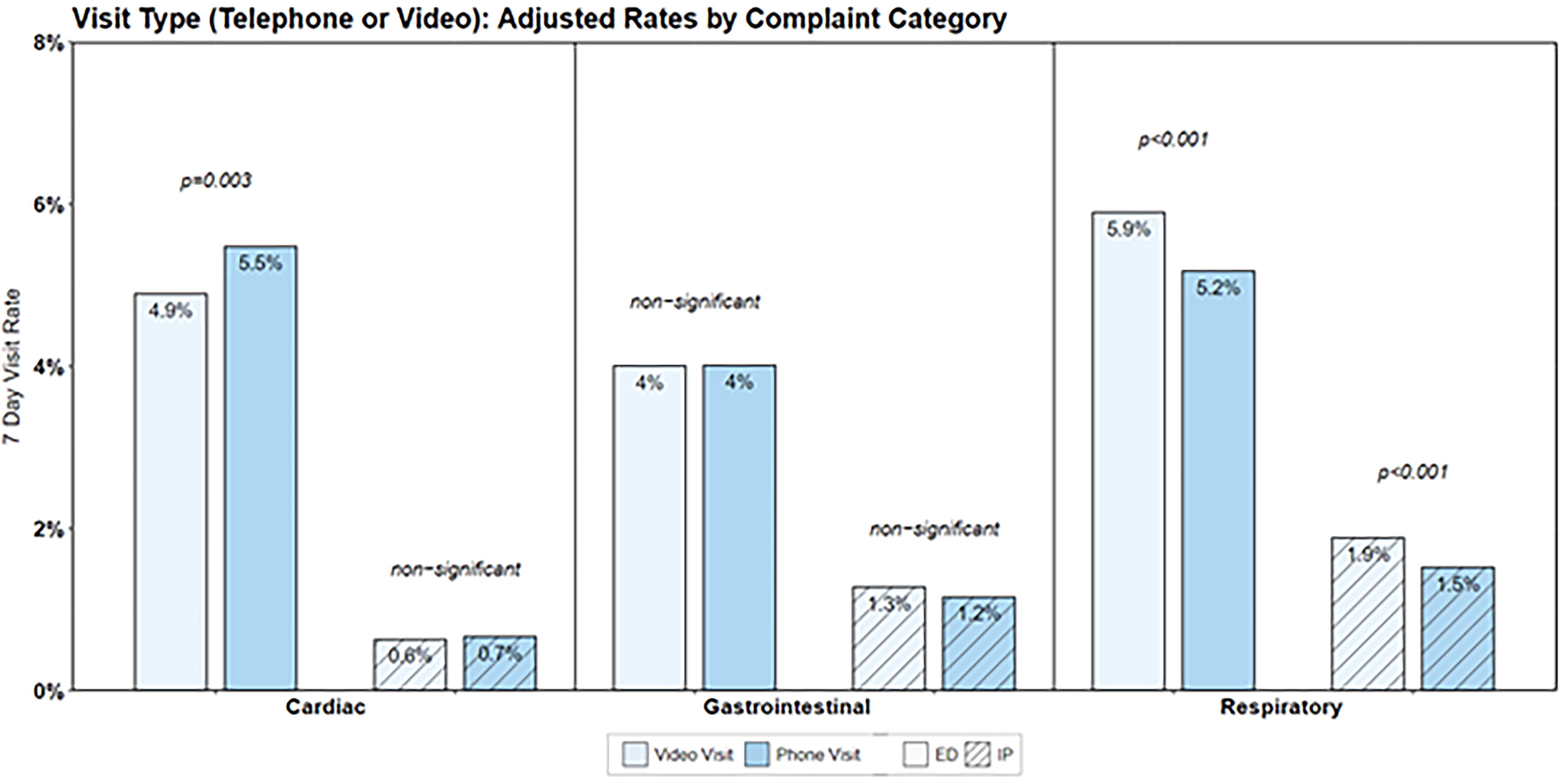
Adjusted rates of 7-day emergency department post-telemedicine visits among cardiac, gastrointestinal, and respiratory diagnoses comparing telephone and video encounters.
Fig. 3 (adjusted 7-day ED and hospital admission rates by condition comparing personal PCP encounters and any other PCP encounters) shows that across all three conditions, telemedicine encounters with one’s personal PCP were associated with a lower risk of 7-day ED and inpatient utilization, even adjusting for telemedicine modality. To adjust for the significant difference in time from booking to appointment between personal and unfamiliar PCP visits, we included an interaction term for booking to appointment within 12 h and PCP type in our GEE model. In a sensitivity analysis excluding March–May 2020, encounters when video was much less common than phone care, trends in adjusted rates of ED and inpatient utilization were comparable by condition category, telemedicine modality, and provider familiarity to the full study cohort results.
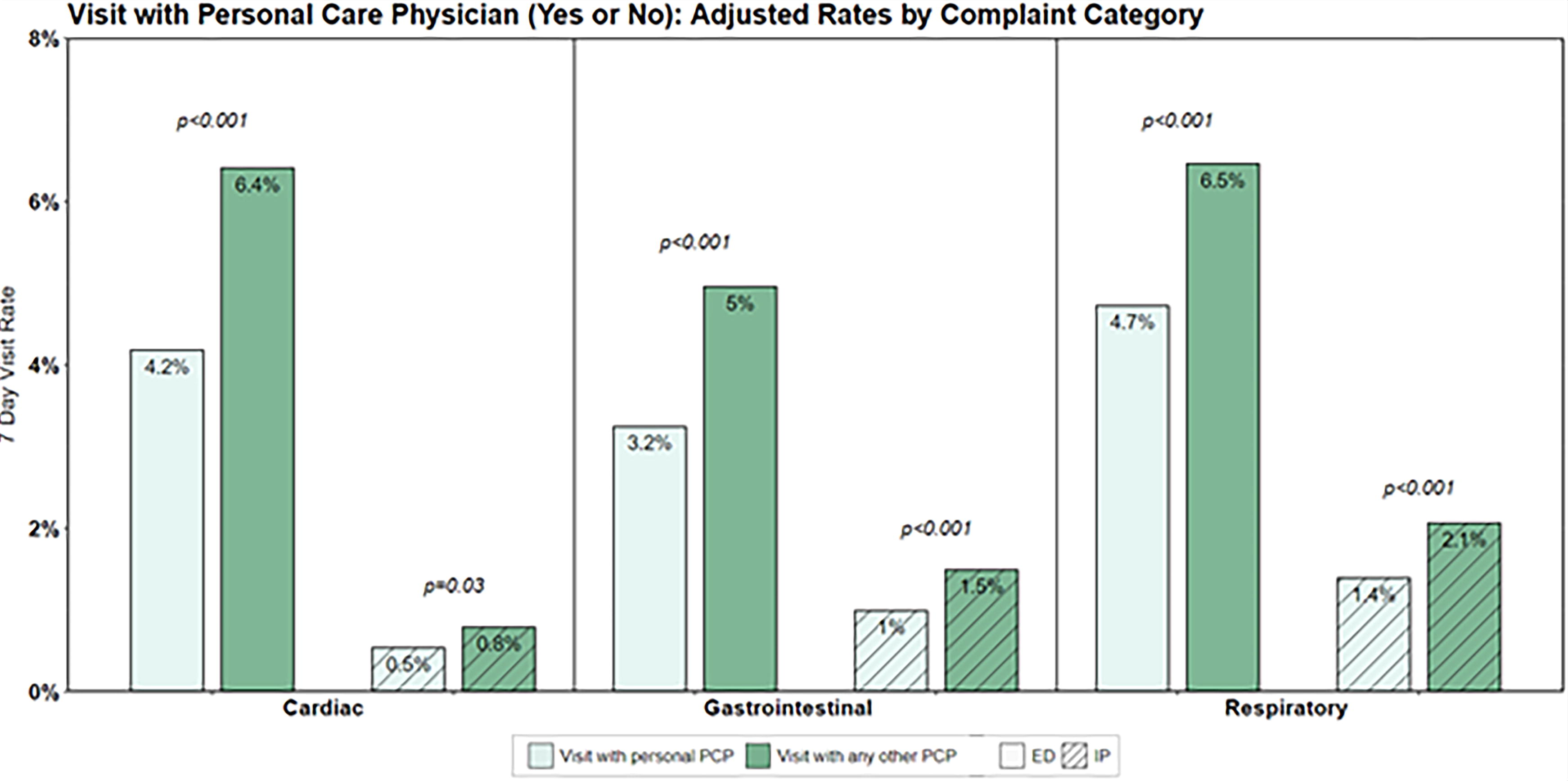
Adjusted rates of 7-day emergency department and inpatient post-telemedicine encounters among cardiac, gastrointestinal, and respiratory diagnoses comparing personal primary care physician (PCP) and nonpersonal PCP telemedicine encounters.
Discussion
In this retrospective analysis of patient-initiated primary care telemedicine encounters for acute, potentially high-risk cardiac, gastrointestinal, and respiratory conditions in an integrated health care delivery system, we observed condition- and modality-specific variation in post-telemedicine outcomes. The adjusted association between telemedicine modality and downstream ED utilization varied by diagnostic category, with video visits associated with lower short-term rates of ED use for cardiac conditions than phone visits but higher ED use for respiratory conditions. Furthermore, telemedicine visits with a patient’s personal PCP were associated with a lower adjusted risk of ED visit or hospitalization across all condition groups and telemedicine modalities.
Our study adds to a growing understanding of the impact of primary care telemedicine on downstream health care utilization, especially when in-person visits may be unavailable or less preferred by patients. We focused on primary care visits for acute, high-risk conditions that often require urgent diagnosis and evaluation in the ED and/or hospitalization. Our finding that video visits were associated with a lower adjusted rate of ED use for acute cardiac conditions compared with telephone visits suggests that video visits may provide visual and nonverbal cues to aid in triaging potentially high-risk conditions such as chest pain or angina. However, visit modality was not associated with differences in ED use for gastrointestinal conditions, and video visits were associated with higher rates of ED use for respiratory complaints. It is possible that a potential driver of ED visits is referral for urgent testing to “rule out” serious disease, and video visits may provide condition-specific benefit in telehealth-based triage. Hospitalization rates at 7 days for cardiac and gastrointestinal conditions, however, were similar for video and phone modalities. Beyond intuitive use cases such as video for dermatologic complaints and telephone for routine refill requests, the utility and effectiveness of video and phone care are nuanced, and further investigation of the condition-specific role of video visits and how to improve access to video care should be priorities in telemedicine expansion and research.
We hypothesized that video visits might convey visual information via “face-to-face” connection, which might be helpful to patients and providers, potentially overcoming barriers of physician-patient unfamiliarity in remote visits. Telemedicine visits with a patient’s personal PCP were associated with lower 7-day ED visit and hospitalization rates across all condition groups we studied, even after adjusting for telemedicine modality, booking to appointment interval, and patient characteristics, and despite availability of a comprehensive EHR. Our findings are similar to prior studies describing increased use of urgent and emergency care services among patients without an affiliated PCP and those experiencing PCP turnover or loss. 33,34 Patients older than 65 years with a familiar PCP have also been found to have lower ED visit rates than those without a familiar PCP, 35 and one recent study reported lower 7-day ED visits after a telemedicine visit with one’s personal versus an outside PCP. 36 The consistency of this finding in ours and prior studies may reflect physician-patient familiarity and different risk tolerance of familiar versus unfamiliar physician-patient interactions. Conversely, unmeasured factors, such as higher illness acuity, may account for the difference. However, to account for the potential impact of observed differences in booking to appointment times between familiar and unfamiliar PCPs, we adjusted for PCP familiarity and booking to appointment interval within 12 h in our models.
Video visits may present technical challenges including need for strong internet connection, a video-enabled device, and greater digital literacy. Similar to prior studies, 3,6 –10 we observed differences in telephone versus video visits by patient age, race/ethnicity, primary language, neighborhood income level and digital connectivity, comorbidity burden, and recent health care utilization. The reasons for these differences warrant further exploration, especially if video provides advantages in clinical assessment over telephone in specific situations, as overcoming barriers to video care is paramount to achieving equitable access to quality telemedicine care.
LIMITATIONS
Due to the retrospective observational study design, we encountered several limitations. Unmeasured differences between phone and video visit users and personal PCP versus nonpersonal PCP visits may persist despite inclusion of relevant covariates in regression analysis, and patients’ familiarity with their personal PCPs varies. We observed a difference in time from booking to appointment for personal versus unfamiliar PCP visits and included an interaction term to account for the difference, but unmeasured differences in visit availability may persist. We could not ascertain whether the telemedicine and ED or hospital encounters were for the same condition or if patients were referred or self-directed to the ED (although we observed a short gap between most telemedicine and subsequent acute care), or if booked visit matched actual visit modality (video visits may have been converted to telephone and vice versa). Technical support for video visits to patients and providers was substantial though, so booking mostly matched visit modality. Early in the pandemic, office visits were booked only after initial telehealth visit, so comparing office visits with telehealth was infeasible as office visits were likely preceded by telehealth visits rather than de novo evaluations for a given complaint. Claims data were used to capture outside hospitalizations and ED visits; while dual insurance coverage visits might have been excluded, dual coverage is rare in our cohort.
Our findings may have limited external generalizability to systems with less access to primary care or video visits and for health systems without a comprehensive EHR accessible to all providers. Our integrated system’s internal capacity for ancillary laboratory and radiology testing may not translate to other settings. We focused on ED-sensitive conditions specifically to evaluate patients with a higher probability of needing acute care, and findings may not apply to all-cause telemedicine visits.
Conclusions
In this study of patient-initiated primary care telemedicine encounters for potentially high-risk undifferentiated conditions, adjusted rates of post-ED and inpatient care varied by condition, with video associated with lower postvisit ED use for cardiac visits but higher use for respiratory conditions. Post-telemedicine ED visit rates were lower when patients interacted with their own personal PCPs in both telemedicine visit modalities. Our findings add to a growing understanding of the potential value of video care in triaging conditions with higher potential for needing emergency care.
Authors’ Contributions
M.V.K., D.R.S., M.E.R., M.J.S., and E.M.W. had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: M.V.K., D.R.S., and M.E.R. Acquisition, analysis, or interpretation of data: M.V.K., D.R.S., M.E.R., M.J.S., R.B., J.Y.Z., and E.M.W. Drafting of the manuscript: M.V.K. and D.R.S. Critical review of the manuscript for important intellectual content: M.V.K., D.R.S., M.E.R., M.J.S., J.Y.Z., A.S.R., R.B., and E.M.W. Statistical analysis: M.V.K., M.E.R., D.R.S., E.M.W., and M.J.S. Obtained funding: M.V.K., A.S.R., M.E.R., and D.R.S. Administrative, technical, or material support: A.S.R. and J.Y.Z. Supervision: M.V.K., M.E.R., and D.R.S.
Footnotes
Disclosure Statement
M.V.K., D.R.S., M.J.S., E.M.W., R.B., J.Y.Z., A.S.R., and M.E.R. report no conflicts of interest.
Funding Information
This project was supported by the Garfield Memorial Fund.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.