
Abstract
Background:
Missed appointments adversely affect clinical outcomes, clinic efficiency, and quality of care and could worsen the impact of pediatric workforce shortages on health care access. Telemedicine has the potential to reduce missed appointments. However, interventions that do not account for neighborhood factors could widen disparities. We analyzed the relationship between missed appointments and type of pediatric appointment and the role of telemedicine and neighborhood factors.
Methods:
This retrospective cohort study used three data sources: (1) electronic health records, (2) American Community Survey, and (3) Housing and Urban Development crosswalk data. The analyses were restricted to pediatric patients (<18 years) with completed or missed outpatient visits (March 2020–December 2022). The outcome was missed appointments. The primary predictors were pediatric visit type, appointment modality, census tract (CT) residential segregation, and CT poverty level. Generalized estimating equations were used.
Results:
The final sample size was 90,712 appointments for 32,305 unique patients. The overall no-show rate was 20.75%. The no-show rate for general pediatrics was 20.36% and 27.82% for specialty appointments. In multivariable analyses, there was an increased likelihood of missed appointments for pediatric subspecialty appointments compared to general pediatrics (Odds Ratio (OR): 1.62; 95% Confidence Interval (CI): 1.51, 1.74). Telemedicine appointments were associated with a decreased likelihood of missed appointments compared to in-person appointments (OR: 0.41; 95% CI:0.39, 0.44). There was a positive interaction between appointment type and pediatrics visit type with a larger effect for subspecialty visits.
Conclusions:
Tailored interventions that integrate telemedicine uptake and contextual factors have the potential to reduce missed appointments.
Introduction
Missed appointments refer to patient nonattendance of scheduled clinic visits without prior cancelation, exhibit disparities, and adversely affect care continuity and health outcomes. 1 –3 Missed appointments also limit health care access for other patients, adversely affecting clinic efficiency and revenue. 3 –10 Pediatrics studies have mostly reported missed appointment rates ranging from 8% to 40%, 4,9 –12 with some clinics reporting rates up to 80%. 13
Reducing missed appointment rates is crucial for pediatric clinics in academic medical centers given the significant proportion of underserved patients who receive care in these settings and the budgetary constraints often experienced by these health care systems. 14 –16 Persistent pediatric subspecialist shortages 17 –19 necessitate the identification of variations in missed appointment rates between general and subspecialty appointments, as these could guide targeted interventions.
Telemedicine has been associated with a reduced likelihood of missed appointments compared to in-person visits, highlighting the role this unique tool can play in reducing missed appointments. 20 –24 However, most of the studies in this area are focused on adults, restricted to subspecialty settings, focused on only telemedicine visits, or analyzed in-person and telemedicine visits separately. 20 –27
Neighborhood factors such as high poverty levels, the proportion of Black residents, or area deprivation have been associated with missed appointments. 3,11,24,25,28 –30 Few studies have analyzed the influence of neighborhood factors on missed appointments in pediatric settings, and it is unclear whether neighborhood factors affect the relationship between the type of pediatric visit and missed appointment. Our study aims to fill the gaps in the literature using the following research questions: (1) What is the relationship between the pediatric visit type (general vs. subspecialty) and missed appointments? (2) Are visit type, telemedicine appointment, and neighborhood factors independent predictors of missed appointments? and (3) Does the effect of telemedicine on missed appointments vary by pediatric visit type?
Methods
DATA SOURCE AND STUDY SAMPLE
This is a retrospective cohort study using three data sources: (1) electronic health record (EHR) data from a safety-net academic health care system with 11 FQHC clinics that implemented telemedicine in March 2020, (2) 2020–2022 American Community Survey (ACS) 5-year estimates 31 and, (3) 2020–2022 Housing and Urban Development (HUD) United States Postal Service Zip Code crosswalk data. 32 The analyses were restricted to pediatric patients (<18 years) with completed or missed general pediatrics, family medicine, or pediatrics subspecialty outpatient appointments between March 2020 and December 2022. The EHR data had information on appointment and demographic characteristics, as well as zip codes. ACS data had census block and census tract (CT) demographics information. The HUD ZIP Code to CT Crosswalk data were used to link the EHR and ACS data. In line with previous studies, 33 the CT with the highest proportion of residents was used for zip codes that crosswalked with multiple CTs in the HUD data.
MEASURES
The outcome variable was missed appointments (no [0]; yes [1]), defined as a missed clinic visit or a cancelation less than two hours before the appointment. The primary predictors of interest were the appointment type (general vs. subspecialty), appointment modality (in-person vs. telemedicine), CT residential segregation, and CT poverty level. Family medicine appointments were categorized as general pediatric visits. Residential segregation was operationalized using the isolation index, a minority-weighted index that measures the extent to which minoritized individuals, like non-Hispanic Black or Hispanic individuals, interact with the White residents of an area. 34,35 The isolation index ranges from 0 (no segregation) to 1 (complete segregation). 34,35 We derived CT Black and Hispanic isolation indexes. CT poverty level, derived from the ACS data, measures the proportion of residents in each CT living below the federal poverty level. The poverty level was categorized as low (<9.90%), intermediate (9.91–19.90%), and high (>19.90%). Control variables were race/ethnicity, sex, insurance coverage, and year of visit.
STATISTICAL ANALYSIS
Descriptive statistics of the sample characteristics were calculated, and differences by appointment type were analyzed using Pearson’s χ2 test and t-tests for categorical and continuous variables, respectively. We used generalized estimating equations with a logit link to account for the nested nature of our data and the dichotomous outcome variable using four models as follows: missed appointments and type of specialty appointment adjusting for the control variables (Model 1), then adjusting for telemedicine (Model 2), residential segregation (Model 3), CT poverty level (Model 4), and the interaction between type of specialty appointment and appointment modality (Model 5), respectively. All analyses were conducted using STATA/MP version 15.1. 36 Statistical significance was assessed at the α = 0.05 level. This study was approved by the Arizona State University and Valleywise Health Institutional Review Boards. The data were analyzed from January to March, 2024.
Results
The final sample size was 90,712 appointments for 32,305 unique patients (Table 1). There was a higher proportion of general pediatrics appointments (94.75%) compared to subspecialty appointments (5.25%) and in-person appointments (86%) compared to telemedicine appointments (14%). The highest proportion of appointments were for Hispanic patients (66.08%), followed by non-Hispanic Black (15.82%), non-Hispanic White (11.8%), Asian (2.92%), Native American (2.38%), and “other” (1%) patients. The missed appointment rates for general pediatrics and subspecialty appointments were 20.36% and 27.82%, respectively.
Descriptive Characteristics of the Study Sample (n
In multivariable regression analyses, there was a higher likelihood of missed appointments for subspecialty appointments compared to general pediatrics appointments (OR: 1.81; 95% CI: 1.68, 1.95) (Table 2, Model 1). This relationship remained statistically significant after controlling for appointment modality with a reduced likelihood of missed appointments for telemedicine appointments compared to in-person appointments (OR: 0.41; 95% CI: 0.38, 0.44) (Model 2). Missed appointments were associated with increasing Black (OR: 1.39; 95% CI: 1.16, 1.68) and Hispanic (OR: 1.19; 95% CI: 1.08, 1.31) isolation index. However, the isolation indexes did not explain the relationship between pediatric visit type and missed appointments. Model 4 shows that there was a higher likelihood of missed appointments among residents of CTs with intermediate (OR: 1.21; 95% CI: 1.14, 1.29) and high (OR: 1.25; 95% CI: 1.17, 1.34) poverty levels compared to residents of low poverty census tracts. Model 4 also shows that the relationship between the isolation indexes and missed appointments was no longer significant, indicating that the census tract poverty level explained this relationship. However, CT poverty level did not explain the relationship between missed appointments and pediatric visit type. Model 5 shows a statistically significant interaction between the type of visit and appointment type (OR: 0.24; 95% CI: 0.10, 0.59) an indication that the effect of telemedicine on missed appointments varied by type of appointment and was larger for specialty visits compared to general pediatrics visits.
Multivariable Regression Analyses of Missed Appointments (n = 90,712)
Hispanic ethnicity includes any race.
p < 0.001.
p < 0.01.
Fig. 1 shows the predicted probability of missed appointments for general pediatric appointments was 0.22 for in-person appointments compared to 0.11 for telemedicine appointments (11% reduction). For subspecialty appointments, the probability of missed appointments for in-person visits was 0.32 and 0.04 for telemedicine (28% reduction).
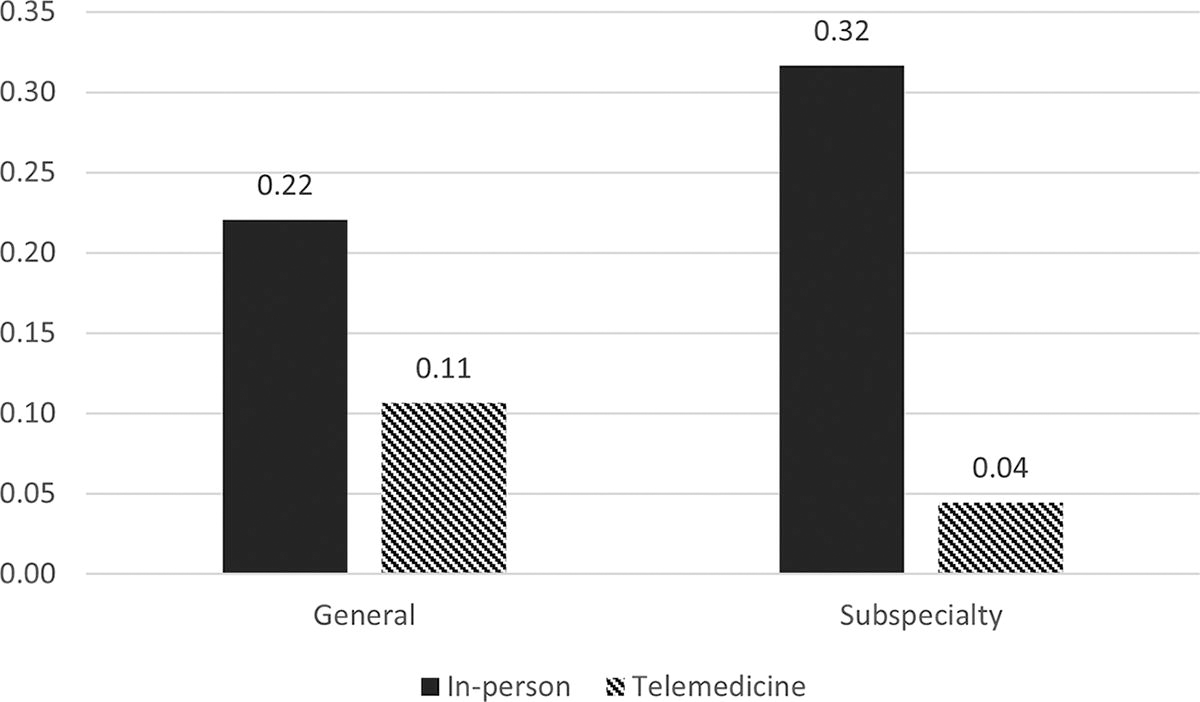
Predicted probability of missed appointments by specialty type and appointment modality.
Discussion
This study analyzed the relationship between missed appointments and type of pediatric appointment, whether telemedicine appointments, residential segregation, and CT poverty level explain this relationship, and whether the effect of telemedicine on missed appointments varied by type of pediatric appointment. Results showed a higher likelihood of missed appointments for subspecialty appointments compared to general pediatrics appointments. Appointment modality and CT poverty level were independent predictors of missed appointments and did not explain the relationship between the type of appointment and missed appointments. Finally, the effect of telemedicine on missed appointments was larger for pediatric subspecialty appointments compared to general pediatric appointments.
The continued pediatric clinician workforce shortage has undesirable implications for pediatric health care access, especially for underserved patients who reside in areas with limited subspecialty pediatrician availability. 17 –19,37,38 Limited pediatrician availability has been associated with prolonged wait times, increased travel distance to a provider, and delayed or forgone care. 17,19 Our study finding highlights the need to identify and address barriers to subspecialty clinic visits, such as lack of childcare, work schedule conflict, lack of transportation, and cost. 39,40
Telemedicine interventions can be leveraged to address missed appointments and their adverse effect on patient care and health care system operations, especially given that research has shown persistent occurrence of missed appointments despite strategies such as reduced appointment lead time, text and phone appointment reminders, and overscheduling. 3,4,7,41 –45
Our finding of a decreased likelihood of missed appointments with telemedicine appointments compared to in-person appointments and the larger effect of telemedicine on missed subspecialty appointments is indicative of the unique role that telemedicine could play in reducing the adverse consequences of physician shortages and improving health care access. 46 –48 This finding is in agreement with previous studies that have reported a reduced likelihood of missed appointments for telemedicine appointments compared to in-person appointments. 20 –24,49 This finding is also relevant considering the inconsistent effects of strategies like reduced appointment lead time, overscheduling, and appointment reminders. 3,4,7,41 –45
This study also found that the CT poverty level was an independent predictor of missed appointments, which is in line with previous studies that have shown an association between neighborhood deprivation and missed appointments and associated disparities. 25 The insufficiency of telemedicine in addressing missed appointments has been demonstrated by other studies that have reported missed appointments among patients with a scheduled telemedicine appointment. 21 Thus, nuanced telemedicine interventions that account for individual-level and contextual factors are needed. Strategies that integrate other health care workforces, such as community health workers, could facilitate the implementation of such interventions without placing an additional burden on the pediatrician. 11,19
Limitations
This study has several limitations. First, the study setting is an academic safety-net health care system; therefore, the results might not be generalizable to other health care settings. Second, the analyses were restricted to the variables in the EHR, and we were thus unable to control for other factors that could potentially affect missed appointments. Third, data limitation did not allow us to differentiate between audio-only and audio-visual telemedicine appointments.
Finally, we are unable to make any causal inference due to the cross-sectional study designs. This study has several strengths. First, our study fills a critical gap in the literature about the differences in missed appointments by pediatric specialty type and the role of telemedicine and neighborhood factors. Second, the use of EHR data reduced the potential for recall bias or measurement errors. Third, the inclusion of neighborhood factors provides insight into the importance of telemedicine strategies that incorporate contextual factors when targeting missed appointments. Fourth, the study period spanning the early and later pandemic periods provides a more thorough overview of the relationship between the COVID-era telemedicine expansion and missed appointments.
Conclusions
Interventions that aim to increase telemedicine use in pediatric settings have the potential to reduce missed appointment rates and, potentially, the adverse effect of pediatrician shortages on health care use, care continuity, and clinical outcomes while improving health care system operations. However, such interventions could worsen disparities if efforts are not made to also address the adverse effect of contextual factors like area poverty. Research is needed to provide insights into strategies to develop and implement such nuanced interventions.
Footnotes
Authors’ Contributions
C.O.O. conceptualized and designed the study, analyzed the data, drafted the initial article, and critically reviewed and revised the article. L.J. coordinated data acquisition, extracted the data, and critically reviewed and revised the article. L.N., J.P.C., and S.Y. contributed to the study conceptualization and critically reviewed and revised the article. All authors approved the final article as submitted and agreed to be accountable for all aspects of the work.
Author Disclosure Statement
The authors have no conflicts of interest relevant to this article to disclose.
Funding Information
This work was supported by the Arizona State University College of Health Solutions Jumpstart grant.