
Abstract
Background:
Telemedicine has been safely used across various surgical specialties at different stages of outpatient care, with effectiveness measured by clinical outcomes, cost savings, and user satisfaction. When employed for communication between physicians at a referral center and lower-complexity hospitals, it enables quick specialist evaluations for patients with relative emergencies. This study describes the experience of a tertiary care service in managing thoracic surgical conditions through telemedicine case discussions.
Methods:
This prospective study, from March 2022 to February 2023, focused on teleconsultations with hospitals in the referral area of a public academic hospital. Consultations were conducted synchronously and asynchronously via a proprietary platform. Data were collected on the originating hospital, patient demographics, admission date, diagnosis, and clinical summary. Cost savings were calculated by estimating avoided round-trip ambulance transportation. The analysis included data from the public health system’s referral records.
Results:
Out of 4,386 evaluation requests, 341 (7.7%) were discussed with a thoracic surgery specialist. Of these, 181 (53%) were managed without patient transfer, and 53 required rediscussion to revisit the initial medical approach. Immediate transfer, outpatient evaluation, or surgery was recommended in 160 cases.
Conclusion:
The incorporation of telemedicine into interhospital regulation of thoracic surgical diseases effectively reduced unnecessary patient transfers while providing the originating service with valuable information for managing specialty-specific situations.
Introduction
Telemedicine has emerged as a powerful tool in delivering safe and effective care to surgical patients. It has been successfully applied across various surgical specialties, demonstrating safety at different stages of outpatient surgical care. Its effectiveness has been evaluated through clinical outcomes, cost savings, and user/provider satisfaction. 1 –3
Patients with thoracic surgical conditions often require invasive diagnostic and therapeutic procedures of varying complexity. Some of these procedures, such as thoracentesis and pleural drainage, can be performed by nonspecialist physicians. However, the information obtained from these interventions may require the expertise of a specialist for accurate diagnosis. Clinical reasoning, combined with the analysis of pleural fluid or imaging abnormalities, along with patient history, can guide clinical decisions. 4
While many patient needs can be addressed with clinical measures, a significant portion may require procedures more closely associated with a specialist’s expertise. Particularly in pleural pathologies, procedures such as pleural biopsies, thoracotomy, or video-assisted thoracoscopic surgery are standard approaches in various scenarios. 5 These resources are rarely available in locations without a thoracic surgeon.
Teleconsultation serves as an alternative for patient selection and as a guide for managing patients with thoracic diseases. Through physician-to-physician contact, it can be determined whether a case can be managed locally or if the patient needs to be transferred to a higher-level medical facility. Various studies have shown that teleconsultation reduces mortality and ICU stays by sharing protocols, providing training, and discussing cases with specialists. 6 –8
Telemedicine, when used for communication between physicians at a referral center and those at lower-complexity hospitals, enables rapid access to specialist evaluations for patients with urgent conditions. It surpasses a simple phone call by allowing joint visualization of medical images and the exchange of a greater volume of information, including real-time access to medical records while discussing relevant data. Teleconsultation has been associated with increased confidence, improved information transmission quality, and faster decision-making. Additionally, it has led to reduced hospitalization time, faster diagnosis, and fewer unnecessary procedures. 9
We describe the experience of a tertiary service in addressing the needs of lower-complexity services for managing thoracic surgical diseases after implementing clinical case discussions among professionals by means of telemedicine.
Methods
This study was approved by the hospital’s ethics committee. It was designed as a prospective study with systematic data collection. All cases were discussed by one or two senior thoracic surgery specialists. Some patients were brought up for discussion more than once.
The emergency regulation module of the Sistema Informatizado de Regulação do Estado de São Paulo (SIRESP) system was used. São Paulo State’s Computerized Healthcare Regulation System (SIRESP) is a centralized platform designed to manage and optimize the allocation of healthcare services across the state, ensuring equitable access and efficient use of resources. Electronic forms of patients referred for tertiary care are screened by the medical team, and those with thoracic surgical conditions are selected and prepared for discussion. Two pathways based on risk classification were applied: (1) cases of absolute emergency or urgency are immediately accepted for transfer to ensure patient safety and (2) cases of relative urgency are eligible for teleconsultation. Elective cases are directed to the outpatient regulation module (Fig. 1).
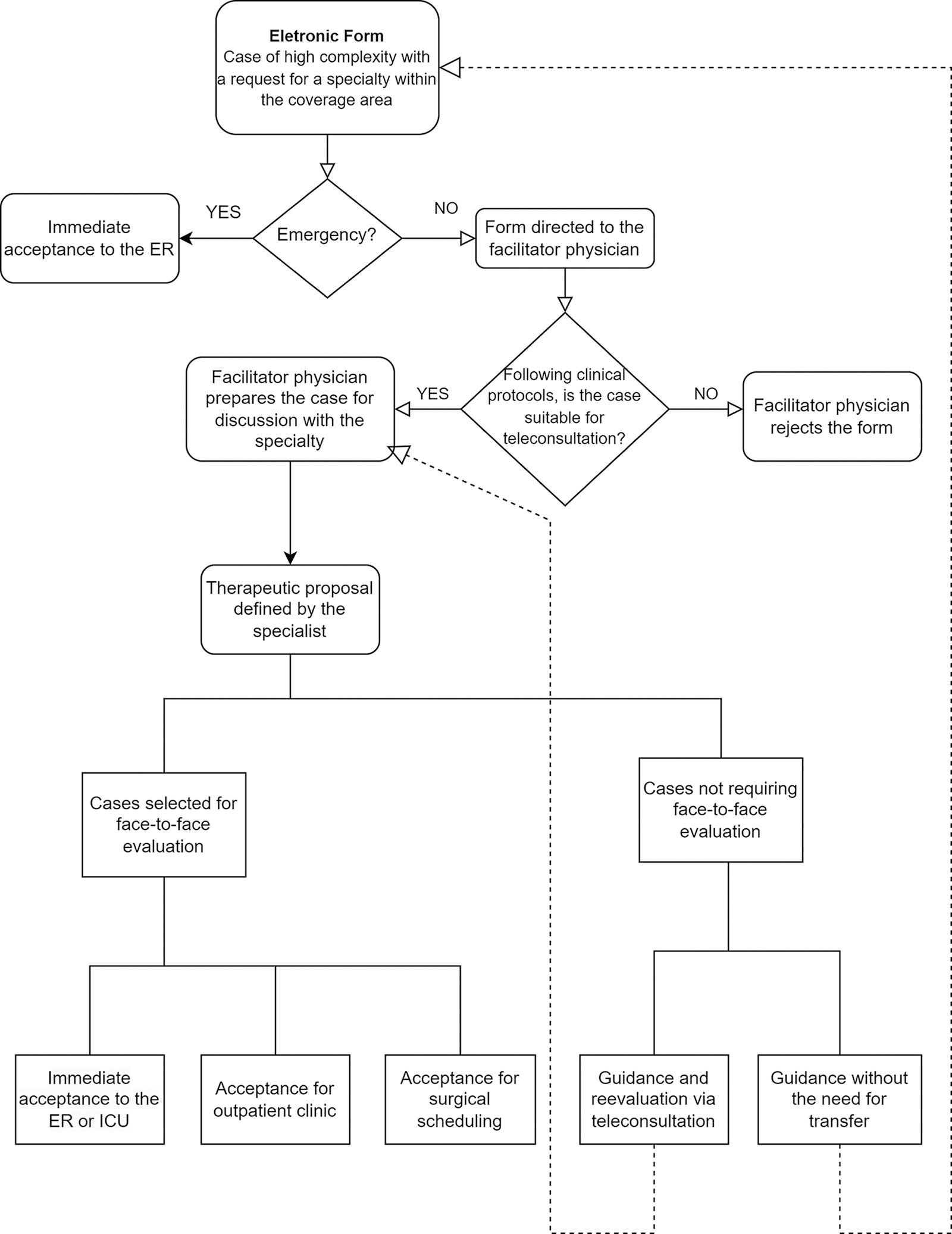
Care regulation flow.
Two teleconsultation models were utilized: asynchronous and synchronous. In the asynchronous mode, physician-to-physician contact is made by the control physician with the originating unit. The thoracic surgeon evaluates each case based on the clinical information and radiological images available in the electronic system. The agreed-upon treatment strategy is then communicated back to the originating unit through a follow-up contact by the control physician.
In the synchronous mode, the discussion takes place in real-time via videoconference, involving the requesting physician, a facilitating physician, and a specialist, with joint visualization of radiological images. For this purpose, the iConf® platform (iconf.incor.usp.br) from the Heart Institute of the Hospital das Clínicas at the University of São Paulo School of Medicine was used. This platform ensures confidentiality, as all data are securely recorded and stored, with no possibility of sharing or manipulation. The medical decision in this mode is made by mutual agreement among all parties involved.
The asynchronous mode was used at the beginning of the experience, and after the introduction of the synchronous mode, it was employed whenever the requesting hospital did not attend the discussion (Fig. 2).
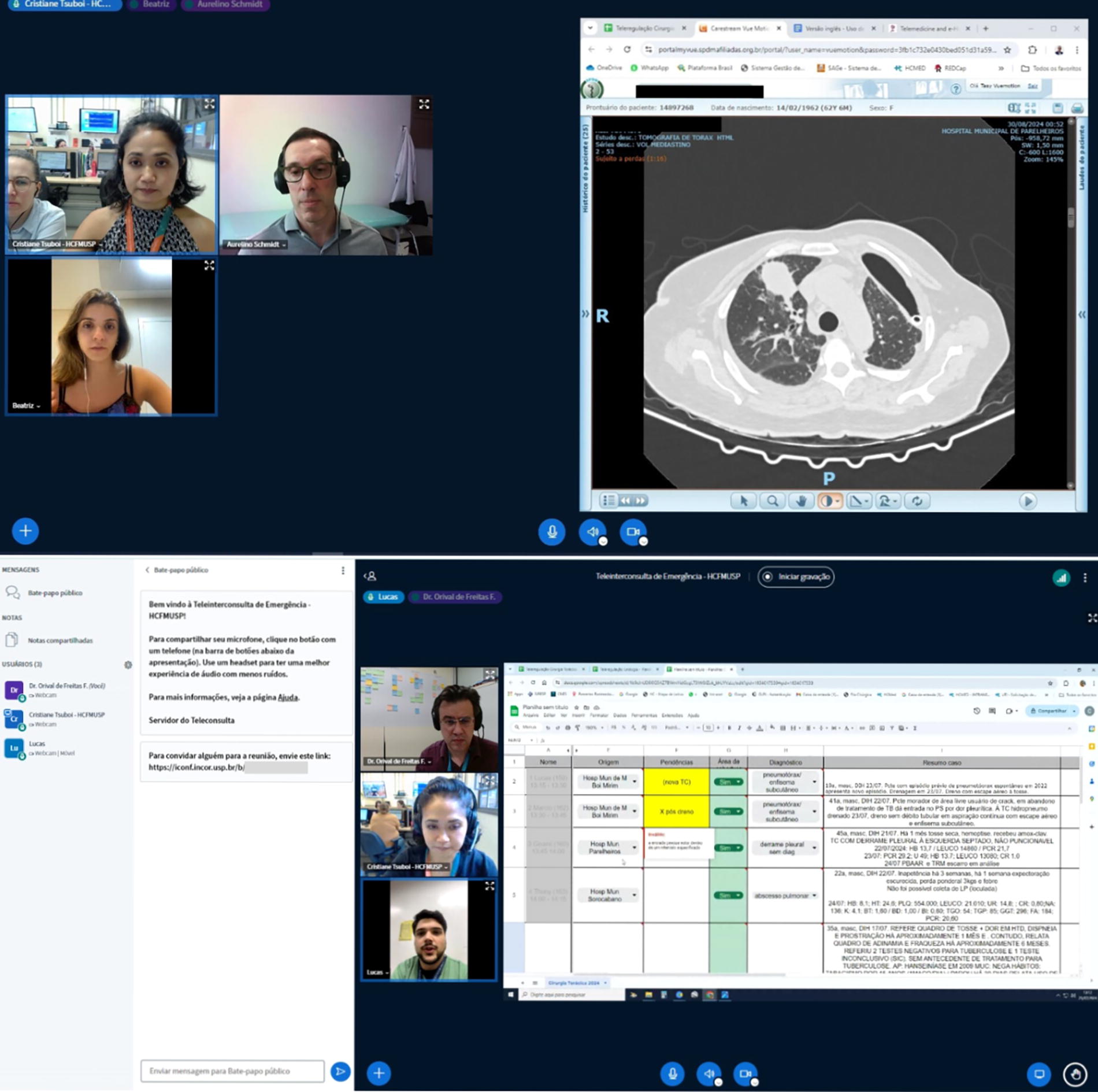
iConf® system interface displaying image and data sharing, enabling synchronous discussions between the thoracic surgeon, facilitator physician, and the physician from the originating service.
Data prospectively collected from March 2022 to February 2023 were used, covering the originating hospital, age, sex, admission date, diagnosis, and a summary of clinical data. The calculation of distance savings was based on the estimated costs of transportation by basic ambulance, with emissions of 270 g/km of nonrenewable fossil CO2 for a round trip. Emissions and equivalencies were calculated using the parameters set by the United States Environmental Protection Agency. 10,11 To analyze the number of evaluation requests submitted, data from the public health system’s referral records were utilized.
For patients who required an in-person evaluation, outpatient appointments were scheduled. Patients referred for outpatient care could also have associated procedures planned.
Patients selected for surgical treatment were transferred the day before the scheduled surgery. Following epidemiological safety protocols, polymerase chain reaction tests for coronavirus disease 2019 (COVID-19) and rectal swab cultures for enterococci and enterobacteria were collected at the originating unit. Preoperative preparation was completed prior to the transfer date. Upon admission, chest CT scans, hematological tests, and blood product reservations were performed. After hospital discharge, patients could either return to the originating unit to complete antimicrobial therapy or be discharged home. All patients were scheduled for follow-up outpatient visits.
Data were summarized using frequency distributions for categorical variables. Histograms were created, and the Shapiro–Wilk test was applied to assess the normality of quantitative data. Means and standard deviations were used for normally distributed values, while medians were used for nonnormally distributed values. This study adhered to the recommendations of the Revised Standards for Quality Improvement Reporting Excellence.
Results
From March 2022 to February 2024, a total of 4,386 evaluation requests were submitted, with 1,950 (44%) originating from hospitals within the referral area. After excluding 1,159 (26%) duplicate requests for the same patients, 791 patients (18%) remained.
Of these, 450 (10.3%) were screened by the regulation physician as not suitable for teleconsultation for various reasons. These include (1) low-complexity cases, which are not applicable for specialized evaluation; (2) cases without an urgent or emergency nature; (3) pediatric cases, which, according to institutional protocols, are managed by pediatric surgery; (4) cases relevant to other specialties; (5) patients already under follow-up with the specialty in other services; and (6) legal demands.
Cases considered relevant but where teleconsultation was not conducted were because of factors such as lack of updated clinical data from the originating unit; no response to requests for clarification or submission of additional exams; patients being referred to other services; resolution of the case by the requesting physician with local resources; deaths; discharges; or patient refusal.
A total of 341 (7.7%) cases were brought for discussion with the specialty after being prepared by the regulation team. In this stage, clinical cases are evaluated individually by the regulation medical team, and relevant data, such as patient history and complementary exams like CT scans and pleural fluid analysis, are requested. The cases are then presented to the specialty in a systematic and standardized manner.
In 181 cases, representing 53% of the total cases assessed by the specialty, an in-person patient evaluation was deemed unnecessary. The care was continued by the referring service under the specialists’ guidance. Instructions were provided on the indications and procedures for thoracentesis, and management of chest drains, including the necessary materials and anatomical landmarks. Guidance was also given on clinical treatment when surgical intervention was not indicated or was contraindicated. Additionally, further tests were requested to clarify diagnoses, guide antimicrobial therapy, refer to another specialty, review imaging exams, and address specific questions. If new questions or developments arose, the cases could be resubmitted for re-evaluation. Fifty-three cases (15%) underwent sequential discussions for a reassessment of the proposed medical approach.
Of the 160 patients selected for in-person evaluation, representing 46% of the total cases discussed by the specialty, 28 were not admitted due to factors such as patient refusal, absence from the outpatient evaluation, discharge by the referring service, unavailability of an ambulance for transport, lack of surgical conditions at the time of admission, unavailability of ICU beds, clinical deterioration, or death.
Of the 83 patients assessed in the outpatient setting, 23 were indicated for surgery. Combined with the 43 who required immediate surgery, 66 patients were admitted for surgery, with hospitalization scheduled for the day before the procedure. Cases reclassified as urgent by the specialty were accepted for immediate transfer to ICU beds, when available, or for evaluation in the Emergency Department (Fig. 3).

Diagram of patient triage and management, including requests and evaluation outcomes.
During the study period, 16 cases were referred through the “‘vaga-zero” system, which is used in situations where the medical condition is urgent. In such cases, the hospital is required to admit the patient immediately, prioritizing care over logistical or capacity concerns.
For comparison purposes, the flow of requests and approvals from the 4 years preceding the start of the teleconsultation project was analyzed. In absolute terms, 537 SIRESP forms were submitted between March 2018 and February 2019, 486 forms from March 2019 to February 2020, 1,069 forms from March 2020 to February 2021, and 1,338 forms from March 2021 to February 2022. The total number of cases accepted per period was 12 patients from March 2018 to February 2019, 40 patients from March 2019 to February 2020, 26 patients from March 2020 to February 2021, 19 patients from March 2021 to February 2022, 67 patients from March 2022 to February 2023, and 93 patients from March 2023 to February 2024 (Fig. 4).
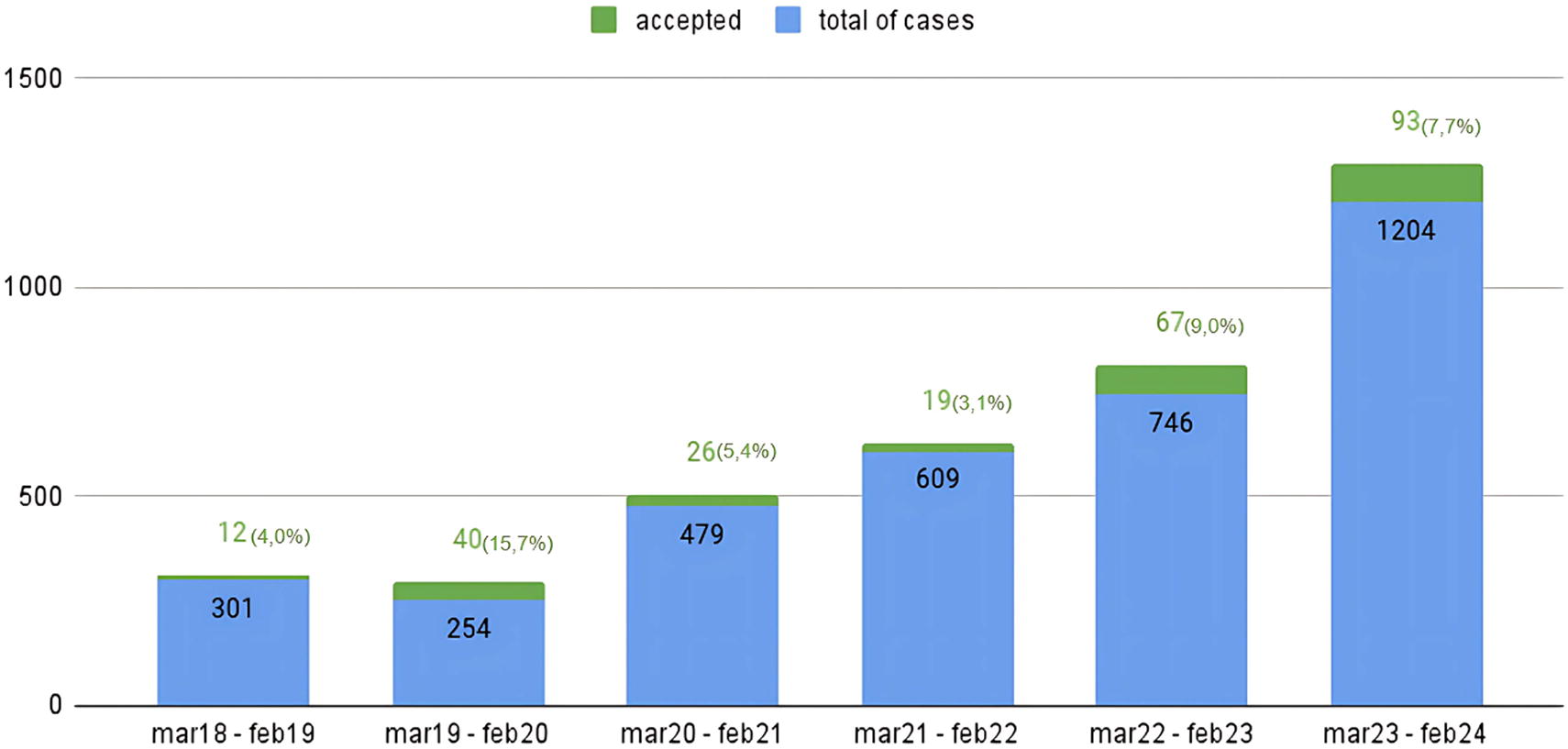
Total number of cases presented and accepted for face-to-face evaluation by period.
The characteristics of the patients accepted during the study period are described in Table 1. The median age was 53 years, with a range from 16 to 97 years. The majority of patients were male (68.6%).
Patients’ Characteristics
The median interval between the date of admission to the originating hospital and the request for evaluation via teleconsultation was 8 days. The time between the discussion and the transfer for surgery ranged from 7 to 136 days, with a median of 25 days. This period includes cases where re-evaluations, either online or in-person, were conducted, as well as cases of surgical rescheduling. When there was no rediscussion or rescheduling, this period ranged from 7 to 63 days, with a median of 24.5 days. The length of hospital stay ranged from 1 to 21 days, with a median of 6.5 days.
The most common conditions were pleural empyema (110 cases), pleural effusion of unknown origin (61 cases), suspected lung neoplasm (33 cases), and pneumothorax (29 cases), among others (Table 2).
Patients’ Characteristics According to Destination: Not Transferred, Out-Patient Clinic, and Surgery
A total of 9,979.6 km in round-trip ambulance transportation was saved, corresponding to the avoidance of 2.7 tons of CO2 emissions. This is equivalent to the amount of carbon sequestered by 40.5 tree seedlings grown over 10 years.
Discussion
This study is the first to focus on teleconsultations between medical services for patient referrals and the first to address pleuropulmonary surgical diseases. It demonstrates the potential to add a new tool to the current interhospital regulation system, with the advantage of avoiding unnecessary transfers in more than half of the preselected cases. This could be particularly useful for organizing the management of relative urgencies in high-demand specialties such as urology, vascular surgery, and neurology, among others.
Telemedicine has been defined as the use of telecommunications technology to provide medical information and services. Its applications include not only direct patient care but also patient education, remote monitoring, and continuing medical education. 12 Teleconsultation is defined as synchronous or asynchronous consultation using communication technology between two healthcare services. 9 In this study, the focus of the interaction was between the medical service directly attending the patient and the specialty referral service, which acted as a consultant and receiver of the cases. Therefore, beyond providing specialist opinions, the patient could be transferred for further evaluation or even surgical intervention.
We found no references either to the prior use of this tool for regulating care or for supporting medical services in issues related to thoracic surgery. A literature review indicates that synchronous teleconsultation has been largely used for strokes in adults and pediatric cardiology. 9 For thoracic surgery, it was used for 56 patients for pre and postoperative care through direct contact with patients 1 and for the follow-up of tracheal diseases. 13 A telemedicine program for training ICU teams in 11 public hospitals on mechanical ventilation was conducted during the COVID-19 pandemic involving 454 patients. The iConf platform was used for contact between health services at prescheduled times, with 10 min allocated for the discussion of each patient, including access to images, educational material exchange, and a whiteboard for free writing. In-hospital mortality was reduced from 88% to 67%. 6
The implementation of the teleconsultation system in this surgical area covered conditions that could be considered for scheduled relative emergency treatment. An increase in the number of cases accepted for referral was observed. However, more than half of the cases in this sample were resolved with local resources, without the need for transfer. This demonstrates the effectiveness of the teleconsultation system in providing the referring services with specialized information. This experience differed from a purely teleconsultation system, as there was a possible flow for patient transfer to specialized care, which maintained the interest of the referring services in establishing a relationship with the reference service and cooperatively following the established management plan.
The facilitator physician plays a crucial role in screening and preparing cases for discussion. In the asynchronous format, they establish contact with the referring service at the appropriate time for dialogue and relay the information from the specialty discussion, supplementing the guidance. In the synchronous discussion, the facilitator schedules case discussion times summarizes clinical and laboratory information, participates in the discussion between the referring service and the specialty, and transcribes it into an electronic system with legal validation.
A systematic review assessed the impact of two distinct models for reducing mortality in ICUs: the first level, “decision-making authority,” included studies where most investigations were conducted with the complete delegation of decision-making responsibility to the tele-ICU intensivist. The second level, “specialist teleconsultation,” included studies where most investigations involved minimal delegation, such as allowing tele-ICU intensivists to intervene only in life-threatening situations or having a strictly consultative role during interventions. The “decision-making authority” model showed a more significant reduction in mortality and length of stay in the ICU. In contrast, the “specialist teleconsultation” model demonstrated a decrease of the in-hospital mortality and an improvement in length of stay compared to traditional care. 7 Thus, in the asynchronous format, this instrument fits as the expert opinion model, while in the synchronous format, it is a joint discussion model.
The entire process is free from conflicts of interest. The contact between services enables continuous education, and the guidance from the specialty is documented for accountability.
For the referral service, there was a decrease in the number of patients admitted for evaluation in the outpatient clinic, but not in the cases directly referred between hospitals. Therefore, this tool was more applicable for relative urgencies that can be scheduled and was less suitable for cases requiring resolution within 24 h. New models of care organization, more patient-centered, would be necessary for these situations. A weak point of the tool was the time for admitting patients with surgical indications, which had a median of 25 days, considered excessively long.
Regulating cases through this system allows for a single queue, ensuring equitable opportunities for patients. For the referral service, it reduces unnecessary in-person consultations and allows for resource planning, enabling the integration of demands into their schedule.
The lack of need for patient transport brings various advantages. It avoids exposing the patient to the risk of transport on a stretcher. By not utilizing the entire transport logistics, the referring team’s time is freed up for other care, and the daily care of the patient is not disrupted. No additional costs, CO2 emissions, or transport time are incurred.
It enables conditions to avoid the duplication of radiological and laboratory tests through the exchange of reliable information between institutions. This can reduce the social and economic impact on families who, by legal obligation, must accompany patients during interinstitutional transfers, by eliminating costs related to transportation, meals, and work absenteeism.
Estimation of indirect cost savings through the use of telemedicine in cancer patient care demonstrated a reduction in both patient time and transportation costs. 14 A systematic review on the use of telemedicine in diverse patient care settings indicated cost reductions when patient or physician transportation could be minimized or avoided. It also highlighted potential productivity gains, reduced reliance on specialist care or tertiary centers, and cost savings resulting from the use of telementoring in specific clinical situations where specialist input improved cost-effectiveness. 15
Potential benefits include reduced queues and waiting times, expanded access, and welcoming, effective care based on risk criteria, without overburdening the care team and infrastructure, while maintaining the quality of services.
The referral service ceases to act merely as a procedure provider but, by enabling interaction, equips the referring services with pertinent information and ultimately disseminates knowledge. It promotes closer collaboration between medical teams, bridging the gap between specialists and general practitioners through individualized treatment discussions and aligning outcomes more closely with the patient’s reality. This approach reduces language barriers and shortens the time to final decision-making, enhancing its effectiveness. Additionally, it encourages skill development in managing pleuropulmonary diseases. This enhances the work of both nonspecialist and specialist professionals.
The ability to absorb relevant cases for specialized treatment ensures that patients are attended to at the appropriate level of complexity. It reduces unnecessary transfers and, consequently, the wastage of resources and adverse events related to transport. Since there is scheduling, integrated with secondary hospitals, it is possible to optimize the use of beds in high-complexity services, reducing the length of stay in the pre and postoperative periods.
Conclusions
This is the first report of a telemedicine program aimed at adding a new tool for the interhospital regulation of patients with thoracic surgical diseases. It shows that a structured program can reduce unnecessary transfers while providing the referring service with useful information to resolve specialty-specific situations. This could prompt the implementation of similar tools in reference institutions.
Footnotes
Authors’ Contributions
A.F.S.J.: Conceptualization, methodology, formal analysis, investigation, data curation, writing-review & editing, supervision. O.F.F.: Conceptualization, methodology, investigation, supervision. C.E.T.: Methodology, investigation, formal analysis, data curation, writing-original draft. T.A.G.C.: Methodology, investigation, formal analysis, data curation, writing-original draft. M.B.M.P.: Supervision, project administration. E.M.U.: Supervision, project administration. P.M.P.F.: Supervision, project administration.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.