
Abstract
Introduction:
The COVID-19 pandemic necessitated swift, dramatic changes to the delivery of essential health care services. Numerous professional societies recommend telehealth care for contraceptive counseling and provision. We conducted a retrospective analysis of service delivery data from Planned Parenthood of Illinois (PPIL), a large reproductive health care provider with 17 health centers in Illinois, to understand if this model preserved access to contraceptive services during the COVID-19 emergency.
Methodology:
This retrospective analysis compared contraceptive service delivery data 12 months pre-pandemic (March 2019–February 2020) with eight months post-pandemic onset (March 2020–October 2020). PPIL consolidated services to six health centers in late March 2020 and rapidly launched telehealth services in April 2020. Our primary outcome was time to appointment compared with pre- and post-pandemic onset. We also compared access by race/ethnicity, age, and geography.
Results:
Although visit volume decreased (76% decline) and time to appointment increased post-pandemic onset (2.5–4 days higher), telehealth mitigated these changes and was used by patients across the entire catchment area. We observed no disparities among Black and Hispanic patients relative to White patients in the likelihood of using telehealth relative to in-person visits (odds ratio 0.7, 95% confidence interval 0.6–0.9 for both comparisons).
Discussion:
Telehealth can play an important role in preserving access to contraceptive services when the health care system is under strain and in increasing accessibility in underserved communities.
Introduction
In January 2020, Illinois had its first reported case of novel coronavirus, 1 SARS-CoV-2; on March 11, 2020, the World Health Organization (WHO) declared COVID-19 a global pandemic. 2 The WHO, 3 American College of Obstetricians and Gynecologists (ACOG), 4 and other state and national 5 organizations recommended that access to reproductive care be maintained in the pandemic response. Executive orders from the Governor of Illinois declared reproductive health care essential, 6 thereby protecting access during pandemic-related closures of nonessential in-person services.
Rapid declines in contraceptive visit volume at the onset of the COVID-19 pandemic have been reported. 7 –11 Prior to 2020, telehealth was an underutilized modality 11 in health care delivery; the COVID-19 pandemic prompted widespread adoption in short time due to favorable changes in insurance coverage of telehealth 7,12,13 and as a way to allow for safe access to services for patients and staff. 14 Professional groups such as ACOG and the Society for Family Planning published guidance early in the pandemic on telehealth for contraceptive care. 15,16 Comfort et al. surveyed contraceptive providers between April 2020 and January 2021 and reported that 79% of providers were using telehealth modalities post-pandemic onset compared with 11% prior to the pandemic. 17 Qualitatively, providers reported that telehealth was acceptable, allowed them to reach patients they otherwise would not have during the pandemic, and allowed for easier contraceptive method switching, and increased access. 18 –20 Some also felt that telehealth improved patient privacy and reduced the influence of providers’ bias in counseling. 19
Disparities in telehealth access among racial and ethnic minorities, young people, and rural communities have been reported. 13,21 People from racial and ethnic groups disproportionately suffered from COVID-19 infection, hospitalization, and death. 22,23
HEALTH CENTER BACKGROUND AND CONTEXT
Planned Parenthood of Illinois (PPIL) delivered more than 37,000 contraceptive visits per year at 17 health centers in Illinois during the study period. Seven health centers were concentrated in Chicago, four in the surrounding suburbs, and six in the central, rural regions. Approximately 52% of PPIL patients used public programs to cover their services, and a free birth control program was available to eligible uninsured or underinsured patients: PPIL provides a critical safety net for contraceptive care in Illinois. PPIL operates health centers in Healthcare Provider Shortage Areas 24,25 and communities disproportionately impacted by infant 26 and maternal 27 mortality.
Changes to PPIL health center operations were made in March 2020 as a result of the rapidly evolving COVID-19 pandemic. On March 5, 2020, COVID-19 screenings with temperature and symptom checks were started for patients. On March 17, 2020, clinic operations were limited to “essential visits,” which included abortion services, treatment for acute issues (e.g., pelvic inflammatory disease), intrauterine device insertions/removals, and contraceptive implant insertions/removals. Expiring contraceptive prescriptions were extended for three months, and birth control/contraceptive counseling visits were suspended. On March 21, 2020, the Illinois Governor issued a “stay at home” order On March 23, 2020, PPIL consolidated service to six health centers to continue to serve patients and meet essential needs while protecting the health of staff and minimizing health center closure due to COVID-19 exposure. We define March 23, 2020, as the “onset” of the COVID-19 pandemic.
On April 6, 2020, telehealth services were initiated, beginning on a limited basis while capacity was increased. Telehealth services included birth control refills, contraceptive/long-active reversible contraceptive (LARC) counseling, depot-medroxyprogesterone acetate (DMPA) reinjection (self-injection was offered), and emergency contraception. Telehealth visits were conducted via synchronous video by clinicians—advance practice nurses or midwives—to patients located in Illinois. On June 15, 2020, the majority of PPIL health centers were reopened and telehealth service continued.
There has been little investigation of the impact of telehealth in maintaining health care quality, its potential role in mitigating acute reduction in contraceptive access resulting from the COVID-19 pandemic or in exacerbating or mitigating racial and ethnic disparities in access to contraception, and access in rural and underserved communities. We present a cross-sectional retrospective analysis of a large reproductive health care provider in Illinois to understand a model of pandemic response in preserving access to contraceptive services.
Methods
A cross-sectional retrospective analysis of PPIL service delivery was performed for 12 pre-pandemic months (March 2019–February 2020) and the first eight months following pandemic onset (March–October 2020). This study was approved by the University of Chicago Institutional Review Board prior to data acquisition.
DATA
Data were extracted by PPIL staff from the NextGen electronic medical record system for all visits occurring from March 2019 to October 2020 at which patients received a new contraceptive prescription, refilled an existing prescription, had a LARC insertion/removal, or received contraceptive counseling. Both in-person and telehealth visits were included. Clinician calls to patients to briefly extend contraceptive prescriptions (a stopgap measure early in the pandemic) were not counted as visits.
Patient demographic characteristics (age, race, and ethnicity), in-person appointment location, date patient scheduled the appointment, appointment date, zip code of residence, final birth control method, and appointment modality (telehealth vs. in-person) were included.
ANALYSIS
Penchansky and Thomas define access as “a concept representing the degree of ‘fit’ between the clients and the system” with five dimensions: availability, accessibility, accommodation, affordability, and acceptability. 28 Here we assess the dimensions of availability, accessibility, and accommodation.
Our primary outcome was mean time to appointment (availability) defined as the original date for which the appointment was scheduled minus the date the patient called or visited the online portal to schedule the appointment. Visits for which the appointment was one month or more after the date on which it was scheduled were excluded (<1% total visits), since these likely represented previously scheduled appointments for routine follow-up. Secondary outcomes included visit volume (availability), distance traveled for care (accessibility), contraceptive method mix, and the likelihood of receiving a telehealth versus in-patient visit (accommodation).
Race and ethnicity were combined into a single variable with categories non-Hispanic white, non-Hispanic Black, Hispanic, Asian, and other/unknown. Contraceptive methods were categorized into four groups: pill/patch/ring, LARC, DMPA, and other. This variable indicates the patient’s contraceptive request; for example, a patient could have a telehealth visit and decide to receive a LARC device requiring a subsequent in-person visit. Visits at which the patient did not decide on a contraceptive method or requested a method not offered were not assigned a value. Two sets of distances were calculated using the Euclidean metric: (1) distance from the centroid of the patient’s zip code to the location of the clinic visited (in-person visits only) and (2) distance from the centroid of the patient’s zip code to the location of the closest open clinic.
The distributions of both the outcomes and covariates were summarized using the mean and standard deviation, median, and interquartile range (distances), or percentages. These distributions were also compared between the pre-pandemic and post-onset periods, as well as between in-person and telehealth visits. Tests of the null hypothesis where the distributions are equivalent were performed using the Wilcoxon rank sum test (continuous variables) or chi-squared test (discrete variables). A kernel-weighted local polynomial smoother 29 was applied to the number of visits per month and the mean time to appointment (in days), and the resulting nonparametric functions were plotted by time. An Epanechnikov kernel was used with a third-degree polynomial and a bandwidth of four months. This analysis was performed separately for all visits (including telehealth) and for in-person visits only.
The number of in-person visits by patients from each zip code was plotted on a choropleth map of Illinois, separately for March 23, 2019 through June 14, 2019 (pre-pandemic) and March 23, 2020 through June 14, 2020. Corresponding maps restricted to the Northeastern region consisting of Chicago and the surrounding collar counties were also generated to provide greater resolution for this area. The locations of each open and closed health center are also shown. A similar map for the entire state was generated showing the number of telehealth visits from April 2020 through October 2020.
Finally, regression models were fit to the weekly visit volume (Model 1), the time to appointment (Model 2), and the likelihood of receiving a telehealth visit (Model 3, April 2020 through October 2020 only). Model 1 was a generalized linear model 30 with log link and Poisson variance function. Covariates included an indicator for post-pandemic onset and dummy variables for calendar month (January, February, etc.), age-group (<18, 18–29, 30–39, and 40+), and racial/ethnic group. In addition, interaction terms between the post-pandemic indicator and each of month, age group, and racial/ethnic group covariates were included. This permits determining whether the overall change from March–October 2019 to March–October 2020 differed according to age or race and ethnicity while permitting the overall outcome to change arbitrarily over time. To do this, predictive margins 31 for the periods March–October 2020 (post-onset) and March–October 2019 (pre-pandemic) were calculated and compared in the form of a rate ratio, separately by age-group and racial and ethnic group. Similarly, predictive margins were used to compare each post-onset month to the average over the period March–October 2019. Model 2 was similar but with identity link and Gaussian variance function (i.e., a standard linear regression), and a contrast between telehealth and in-person visits (post-onset only) was also included. Predictive margins were compared using differences (i.e., March–October 2020 minus March–October 2019). Robust (i.e., sandwich) variance estimates 32 were obtained for both models, and Wald tests were used to test individual contrasts or multiple interaction terms (joint test).
Model 3 was a logistic regression fit to the likelihood that a post-onset visit was conducted via telehealth versus in-person. Covariates included age group, racial/ethnic group, calendar month, and the log (base 2) of the distance in miles to the closest open center. Coefficients are presented as odds ratios, and predictive margins (i.e., percent of visits conducted via telehealth) are also presented.
Data management and analyses were performed using Stata Release 17.0. 33 Plotting for maps was performed using Altair 4.2. 34 Significance was set at p < 0.05 for all analyses.
Results
A total of 23,648 visits were included, with 26% of post-onset visits being conducted via telehealth (Table 1). As expected, telehealth visits were primarily for pill/patch/ring (82%) followed by DMPA (16%), as compared with post-onset in-person visits, which were primarily for LARC (57%) followed by pill/patch/ring (40%). Post-onset time to appointment was significantly shorter for telehealth than for in-person (5 vs. 11 days, p < 0.001), similar to the mean time to appointment for in-person prior to the pandemic (6 days). Those attending in-person visits post-onset traveled only slightly longer, on average, than they did pre-pandemic (5.2 vs. 4.9 miles, p < 0.001).
Distributions of Selected Variables (Means, Medians, or Percentages) Shown Separately for Pre-Pandemic In-Person Visits (Prior to March 23, 2020), Post-Pandemic Onset In-Person Visits (March 23, 2020, and After), and Telehealth Visits (Starting in April 2020)
Wilcoxon rank sum test (continuous variables) or chi-squared test (discrete variables) comparing pre-pandemic in-person visits with post-onset in-person visits.
Wilcoxon rank sum test (continuous variables) or chi-squared test (discrete variables) comparing post-onset in-person visits with telehealth visits.
Mean (SD).
Missing for 196 in-person visits (pre-pandemic), 60 in-person visits (post-onset), and 23 telehealth visits.
Median (interquartile range).
SD, standard deviation.
Monthly visit volume declined sharply following pandemic onset (Fig. 1A). We estimated a 76% (95% confidence interval [CI] 72–80%) decline in April 2020 relative to the period from April to October 2019 (Table 2, Model 1). Telehealth visits mitigated this decline and contributed substantially to recovery (Fig. 1A). Overall, the decline in volume was greatest at lower ages and varied significantly by race/ethnicity: among non-Hispanic white patients (35%, 95% CI 28–43%) as compared with non-Hispanic Black (17%, 95% CI 7–27%) and Hispanic (24%, 95% CI 14–33%) patients. Not surprisingly, the decline in volume of in-person visits was greatest in the areas around health centers that were closed and where an open health center was not available nearby, and this was especially true in the western and southern parts of Illinois that are less populated with longer distances between health centers (Fig. 2).
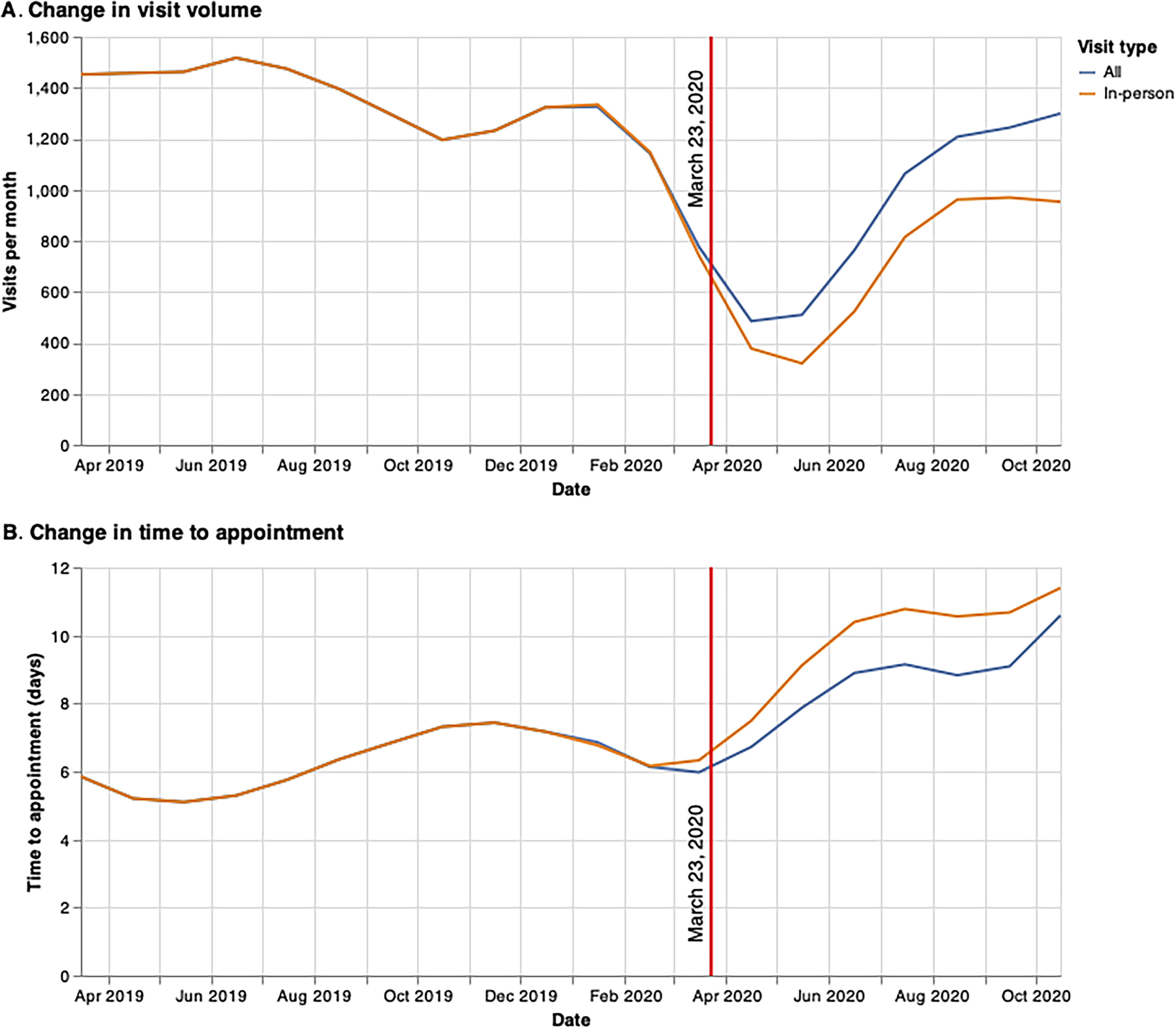
Mean visit volume per month
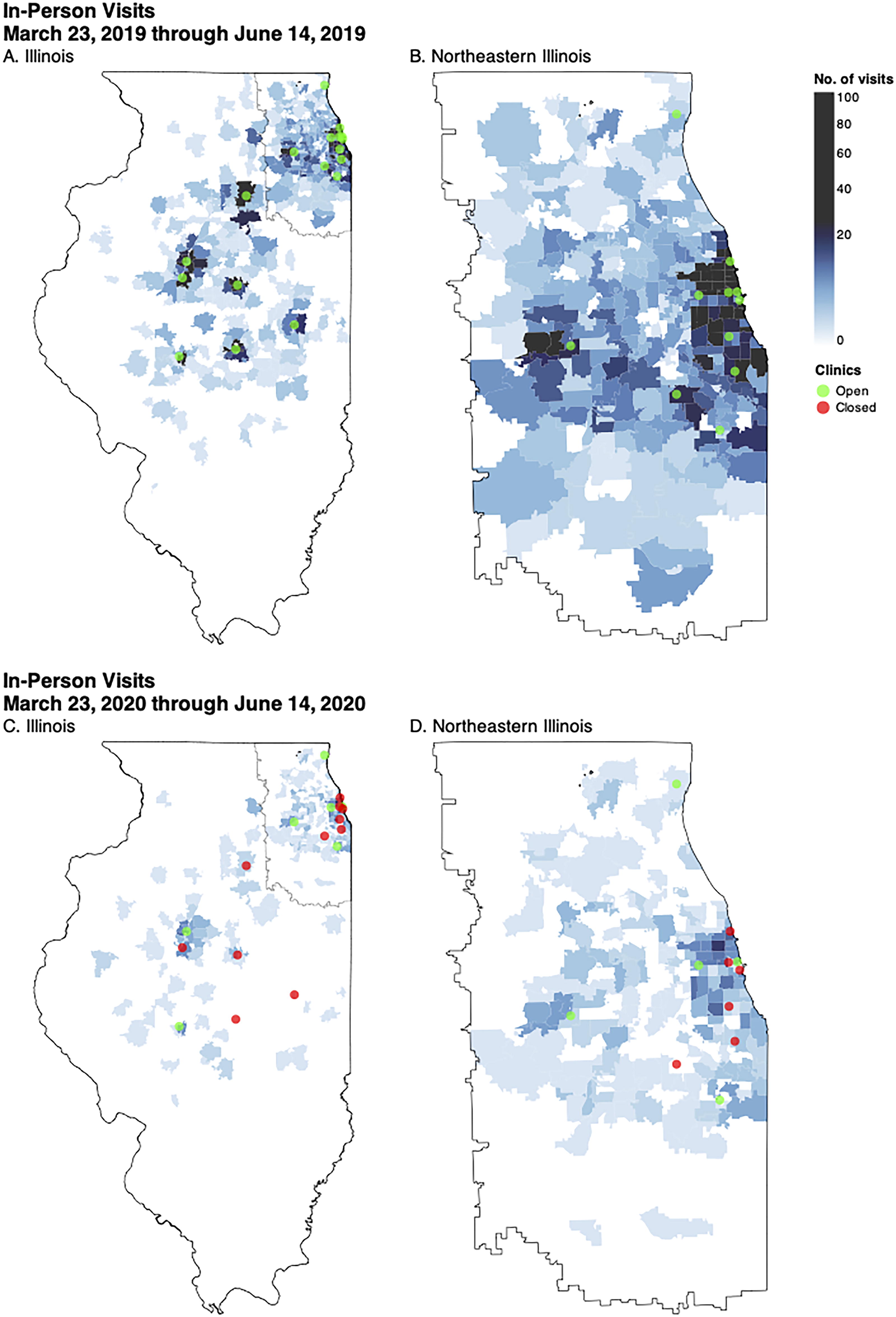
Number of in-person visits by zip code of patient residence, separately for the periods March 23, 2019, through June 14, 2019
Regression Models Fit to Weekly Visit Volume (Model 1) and Time (in Days) to Appointment (Model 2) for the Period March 2019 Through October 2020 and to the Likelihood of Having a Telehealth Versus In-Person Visit for Contraceptive Management (Model 3) for the Period April 2020 Through October 2020
Generalized linear model (GLM) fit to weekly visit volume using log link and Poisson variance function (n = 1,681). Estimates represent ratio of pre-onset rate to post-onset rate. CIs based on robust standard errors.
Linear regression fit to time (in days) from scheduling to appointment (n = 23,551). CIs based on robust standard errors.
Logistic regression fit to the likelihood of having a telehealth versus in-person visit for contraceptive management from April 2020 to October 2020 (n = 3,030).
For Models 1 and 2, changes in average outcome from April–October 2019 (pre-pandemic) to April–October 2020 (post-onset).
For Models 1 and 2, changes from average value for April–October 2019 (pre-pandemic) to current month (post-onset).
Difference between telehealth and in-person visits during April–October 2020 (post-pandemic).
CI, confidence interval.
The average time to appointment increased post-onset and remained roughly 2.5–4 days higher than its pre-pandemic value through October 2020 (Table 2, Model 2). During this post-onset period, the time to telehealth visits was 5.5 days (95% CI 5.2–5.8) shorter than for in-person visits, which reduced the mean time to appointment for all visits by roughly 1.5 days (Fig. 1B). The increase in time to appointment was smallest for patients <18 or 40+ years of age and was less for white (2.7 days, 95% CI 2.4–2.9) than for Black (3.7 days, 95% CI 3.3–4.1) and Hispanic (3.9 days, 95% CI 3.6–4.3) patients.
The percentage of post-onset visits conducted via telehealth peaked in May 2020 at 91% (95% CI 87–95%) and then dropped to 49% (95% CI 47–51%) during July–October 2020 (Table 2, Model 3). Patients younger than 18 were less likely to use telehealth (odds ratio [OR] 0.5, 95% CI 0.3–0.6) as were those 40 and older (OR 0.6, 95% CI 0.5–0.9). Both non-Hispanic white and Hispanic patients were less likely to use telehealth than non-Hispanic Black patients (OR 0.7, 95% CI 0.6–0.9 for both comparisons). Patients living further from an open health center were slightly more likely to use telehealth, with a doubling of the distance required to travel being associated with a 9% increase (95% CI 4–14%) in the odds of a telehealth visit. Patients using telehealth visits were distributed across the entire pre-pandemic catchment area but were concentrated in the areas immediately surrounding each clinic whether open or closed (Supplementary Fig. S1).
Discussion
To balance the competing demands of maintaining access to care while reducing in-person contact for the safety of patients and health care workers, PPIL consolidated services into six sites, reducing in-person availability for contraceptive services dramatically. This decline in service availability mirrored abrupt, dramatic, and sustained national declines in access to contraceptive services following the onset of the COVID-19 pandemic. 8 –11
Our analysis demonstrates that telehealth played an important role in preserving access to contraceptive services while PPIL health centers were closed and in restoring availability to services during the seven months post-pandemic onset. The average time to appointment for telehealth visits was 5.5 days less than for in-person visits during this period. While the overall time to appointment remained elevated seven months after onset, the data suggest that this would have been even higher in the absence of telehealth services.
Evidence for racial and ethnic disparities in the impact of the pandemic was mixed. While visit volume declined less among non-Hispanic Black and Hispanic than among non-Hispanic white patients, the increase in time to appointment was approximately one day more among these groups than among non-Hispanic white patients. Importantly, this was not due to disparities in the use of telehealth, since non-Hispanic Black patients were more likely and Hispanic patients equally likely to use telehealth during this period compared to non-Hispanic white patients. While this analysis does not permit us to determine the factors underlying the decision to use telehealth, the data do suggest that neither race/ethnicity nor geographic location presented barriers to access and that in the absence of telehealth, the disparity in time to appointment among non-Hispanic Black relative to white patients may have been even greater during this period. In addition, telehealth appeared to mitigate the disparity in access among rural communities, especially in areas where the local health center had closed.
While in principle, telehealth was open to anyone in Illinois, our data indicate that during seven months post-onset, those using it tended to live close to an existing health center (whether open or closed), consistent with these being patients who had previously visited or had knowledge of that health center. This suggests an opportunity for telehealth providers to extend their reach into new communities not previously served and where access to services such as contraception and sexual and reproductive health services may be limited. Targeted outreach to these communities should be considered.
Our study is unique in examining the potential value of telehealth services in a few notable ways. We analyzed a large dataset consisting of all eligible visits statewide over a continuous 20-month period, including the first eight months following the pandemic onset extending into October 2020. We were able to assess the impact telehealth had in maintaining pre-pandemic access to contraceptive services, in addition to reporting volume. This dataset allowed for assessment of quality measures: availability, accessibility, and accommodation. The Institute of Medicine’s Crossing the Quality Chasm identifies time to appointment as an important measure of health care quality, 35 and this was a key feature of our analysis. Our patient population consisted of racially and ethnically diverse patients from the largest sexual and reproductive health provider in Illinois that serves patients from both urban and rural health care provider shortage areas.
A limitation to our study is that we included only one organization located in a single state, and therefore, our results may not be generalizable to other contexts. Also, we did not include visits delivered by telehealth apps, thereby likely undercounting the number of people who accessed virtual contraceptive services. Finally, our period of observation ends in October 2020, preventing examination of longer trends in service recovery and telehealth usage as the pandemic continued.
More research is needed to better understand factors affecting patient decision to use telehealth and implications for attempts to prevent disparities in availability, accessibility, and accommodation of care. Despite our results indicating that overall, non-Hispanic Black and Hispanic patients were no less likely to use telehealth than their white counterparts, qualitative research from our team identified a perception among providers in Illinois that white patients were more likely to access telehealth during this period. 19 This perception may have been due in part to racial and ethnic differences in preferred contraceptive method and in the ability and willingness to change methods in response to the limitations of a telehealth visit, as well as differences in the extent to which lack of safe and reliable transportation alone limited a patient’s options to telehealth. There may also be important disparities in access that we could not account for, such as in the ability to make full use of the telehealth platform (e.g., working camera, stable and reliable connection, and privacy).
Contraceptive care is important for maintaining health and autonomy, but access is far from universal. 36,37 Despite the Affordable Care Act’s contraceptive coverage mandate, and long-standing public funding for contraceptive services through the federal Title X program, many U.S. communities remain without comprehensive contraceptive care providers. 38 Telehealth is a crucial access point to contraceptive care, as such, policymakers should maintain access to all telehealth modalities, including audio-only services as a variety of modalities is important for patient access. 19,20 Telehealth enabled patients to access contraceptive services from the relative safety of home during the COVID-19 pandemic, thereby mitigating disruptions to contraceptive access brought on by the pandemic.
Footnotes
Acknowledgments
The authors thank the Society of Family Planning for their generous support of this project.
Authors’ Contributions
D.Y.: Conceptualization, formal analysis, resources, writing—original draft, and review and editing. L.P.S.: Methodology, formal analysis, and visualization. A.M.: Writing—review and editing and project administration. A.K.W.: Conceptualization, resources, and writing—review and editing. D.S.: Conceptualization, writing—review and editing, supervision, and funding acquisition.
Consent to Participate
This study was approved with a waiver of consent.
Data Availability
These data constitute a limited dataset and may only be accessed with permission under a data use agreement. As the principal investigator, D.S. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily reflect the views of Planned Parenthood Federation of America, Inc.
Disclosure Statement
The authors report no conflicts of interest.
Funding Information
This project was funded by the Society of Family Planning Research Fund.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.