
Abstract
Background:
Increasing carbon dioxide (CO2) in the atmosphere contributes to Earth’s warming, which has negative impacts on human health. The health care system is a major contributor to CO2 emissions. Telehealth has the capacity to reduce health-care-related emissions by eliminating patient travel to in-person appointments.
Methods:
Data were obtained from Nebraska Medicine's (NM) electronic medical record. Parameters included patient zip code, provider location, calendar year of visit, and provider specialty. Euclidean distance from centroid zip code to clinic location was calculated. Environmental Protection Agency estimates were used to convert mileage to CO2 saved.
Results:
During the period January 1, 2019, to January 31, 2022, the NM health care system completed 214,241 telemedicine visits for patients whose home zip code is within Nebraska, resulting in greater than 2,600 metric tons of CO2 avoided. Telehealth appointments increased by more than 22,000% from 2019 to 2020. An average of 12.38 kg of CO2 was avoided with each telehealth visit. Medical specialties that avoided the most CO2 included family medicine, endocrinology, and infectious disease.
Conclusion:
This study demonstrates the capability of the NM health care system to rapidly adjust to an emergency pandemic by drastically increasing the use of telehealth, which also avoided thousands of tons of transportation-associated CO2 emissions. Telehealth appointments increased during the height of the pandemic by more than 22,000%. Telehealth is an effective CO2 emission-reducing strategy and a worthy avenue to further explore reduced health-care-related emissions.
Introduction
Recent increases in greenhouse gases (GHGs) in the atmosphere are the result of numerous processes, such as burning fossil fuels for transportation and electricity. These gases absorb and trap heat in the atmosphere, contributing to Earth’s temperature. 1 Carbon dioxide (CO2) is responsible for approximately 2/3 of the increase in temperature due to GHG-driven anthropogenic climate change, and levels are rapidly rising. 2 Estimates suggest that atmospheric CO2 has never exceeded 300 ppm over the last 800,000 years. 3 However, the recent global levels of CO2 measured in the atmosphere in December 2023 were over 420 ppm and are expected to exceed 900 ppm by the end of the century. 2 The consequences of an increase in Earth’s temperature are widespread, including changes in precipitation patterns, increased frequency of droughts and heat waves, more intense severe weather, and the rise of sea level due to melting ice. 4,5 Numerous reports have identified that climate change worsens physical and mental health and disproportionately harms marginalized communities. 6 Increasing health problems due to climate change also increases the burden on the health care system. 7 Because the health care system operates on the same energy that creates GHG emissions, increasing demand perpetuates the increased GHG emissions cycle.
The health care sector is a significant contributor to GHG emissions. Globally, 4.4% of GHG emissions are from health care. 8 In the United States (U.S.), 8.5% of GHG emissions are from health care alone and continue increasing yearly. 9 GHGs produced by health care equate to a loss of 388,000 disability-adjusted life years. 9 The implementation of adaptation and mitigation efforts in the health care sector can help reduce its adverse impacts on the environment.
Telehealth is a potential mitigation strategy that could effectively lower health-care-related emissions by utilizing technology such as video or phone calls and secure messaging for health care communications instead of or in conjunction with in-person visits. Utilizing telehealth limits emissions produced by patients using cars or public transportation to get to their appointments. On average, 8,887 g of CO2 is produced per gallon of fuel burned in the standard U.S. passenger vehicle. 10 This results in 400 g of CO2/mile. 10 These emissions due to travel are eliminated when a patient engages in telehealth from their home. Additionally, telehealth reduces travel time and costs, which benefits the patients. 11 Telehealth has also been shown to be generally equivalent to in-person care for multiple specialties including mental health care, dermatology, and rehabilitation as well as urgent care and primary care visits. 12,13 Telehealth has also been helpful during the COVID-19 pandemic, as it has allowed for the continuation of health care without additional risk of viral spread, in addition to decreasing CO2 emissions. 14
Previous studies have accounted for CO2 emission savings in subsets of health care systems across the country, but none are published for Nebraska Medicine (NM). This hospital system is unique because it is the largest hospital in the state, an academic medical center affiliated with the University of Nebraska Medical Center (UNMC), and a level-one trauma center. This hospital system serves patients from all 50 states and 47 countries. 15 Unique populations are served by this hospital system, as it holds international acclaim in oncology, transplant, and biocontainment. 15 Being the primary health care system in Nebraska, patients often travel hours from their rural communities to receive health care, which adds to CO2 emissions from travel. Nebraska is a unique state, as most of the population is in the metropolitan areas of Omaha and Lincoln, which are on the eastern edge of the state. Rural populations and smaller communities are spread across the 77,348 square mile state. Populations in the western part of the state are closer to Denver, CO, than to the metropolitan areas of Nebraska. From fiscal year 2019–2021, 85% of NM patients from Nebraska were in urban areas (U.S. Census MSA Definition), while 15% were located rurally. This may not account for patients who see NM outreach providers in rural Nebraska, which means rural populations may be underestimated. Additionally, most previously published studies did not explore the change in CO2 emissions related to travel due to the increase in telehealth use during the COVID-19 pandemic. This study is also unique as it evaluates the entire NM system and use by medical provider specialty, in which studies of this size have previously not done.
The purpose of this study was to determine the CO2 emissions saved resulting from a telehealth appointment compared with an in-person appointment. We also evaluated CO2 emissions saved per year due to changes associated with the pandemic, the rate of change per year, and emissions per provider specialty.
Methods
This study was approved by the UNMC Institutional Review Board. Data for this study were obtained from Epic, NM’s electronic medical record, as well as the Data Warehouse housed on NM’s server. The Strata tool was utilized to access the data. Data included patient zip code, year of visit, physical location of physician providing care, and physician specialty. All reports were screened and included if they showed a telehealth appointment (e-consult, e-visit, audiovisual, or audio-only) in the period of January 1, 2019, to January 31, 2022. All departments of appointments were included. The only appointments that may have been excluded by this method were Monroe-Meyer Institute nonphysician visits and any telehealth done outside of NM’s electronic health record system. The age range of participants was 0–103 years old.
In total, approximately 305,000 records were analyzed. Some visits were found to be duplicates and were excluded, resulting in 214,241 total visits analyzed. ArcGIS software was used for handling spatial analysis. The centroids of zip codes were determined, and the Euclidean distance was calculated between clinic locations and each zip code centroid. These measurements provided approximate travel distances in miles from patient locations to their respective clinics. Microsoft Excel and U.S. Environmental Protection Agency (EPA) data, which state that the average passenger vehicle emits 400 g CO2/mile driven, were used to calculate CO2 emissions saved from the mileage.
10
The calculation used was as follows:
CO2 emissions were further categorized into emissions saved per year and emissions saved per specialty.
Results
From January 1, 2019, to January 31, 2022, the NM health care system completed 214,241 telemedicine visits for patients whose home zip code is within Nebraska. This number increased from 517 telemedicine visits in 2019 to 114,435 in 2020 (Table 2). This is a 22,034.43% increase in telemedicine visits from 2019 to 2020 (Table 2). There were 83,586 telemedicine visits completed in 2021, a 26.96% decrease from 2020 (Table 2). Family medicine was the specialty with the greatest total number of visits, with 46,629 in the specified period (Table 1). Infectious disease (21,097 visits), psychiatry (20,966), behavioral health (17,330), internal medicine (IM; 17,119), psychology (13,185), and endocrinology (10,794) were among the other highest utilizers of telehealth (Fig. 2). The lowest visits were completed by occupational medicine, pathology, pediatric hematology–oncology, social work, physician assistant, and pediatric gastroenterology. Each of the specialties recorded just one visit in the period.
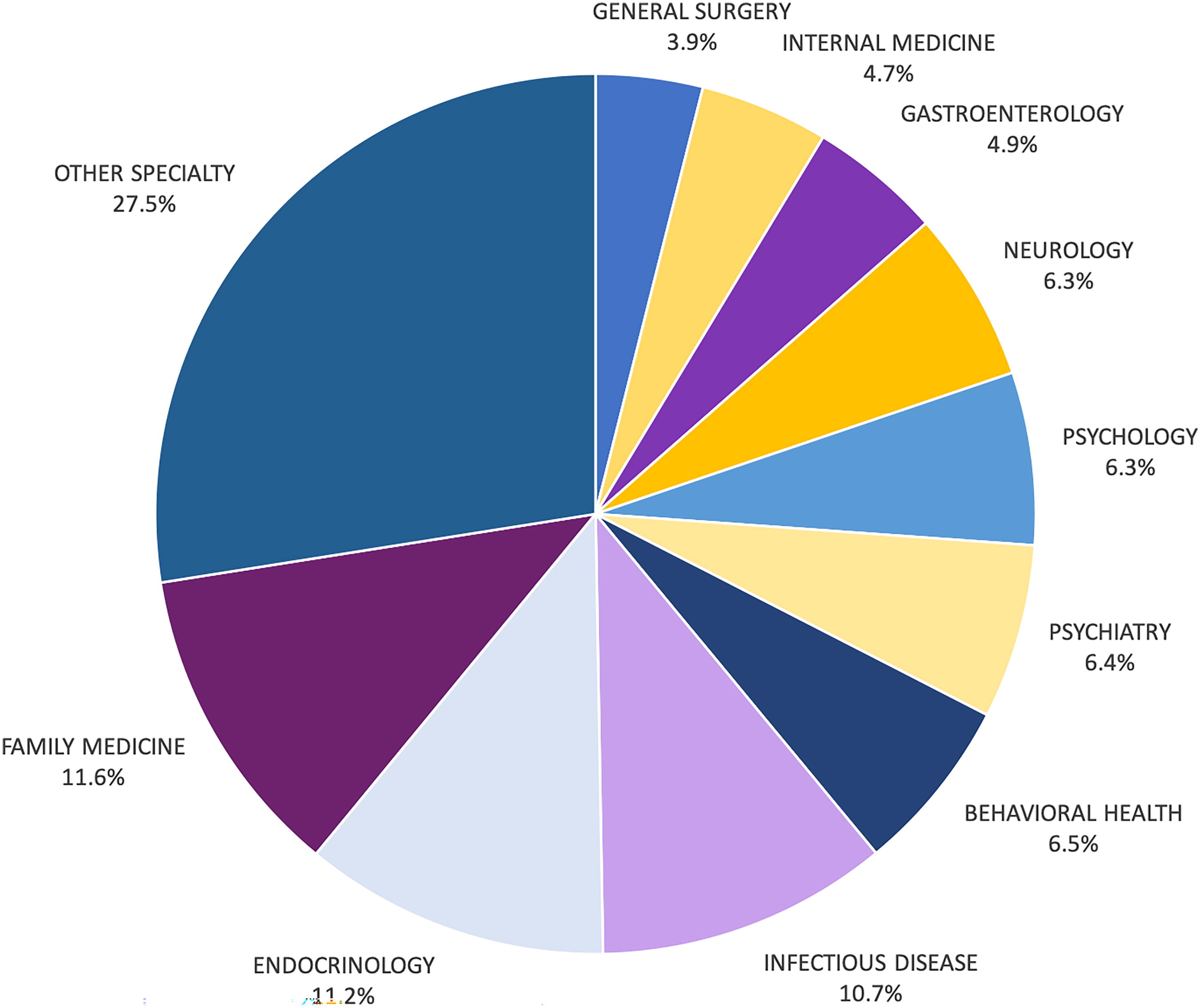
Top 10 specialties’ contribution to the percentage of total CO2 avoided in the study. Family medicine is responsible for the greatest emissions avoided. Approximately 60 other specialties make up the “other” category.
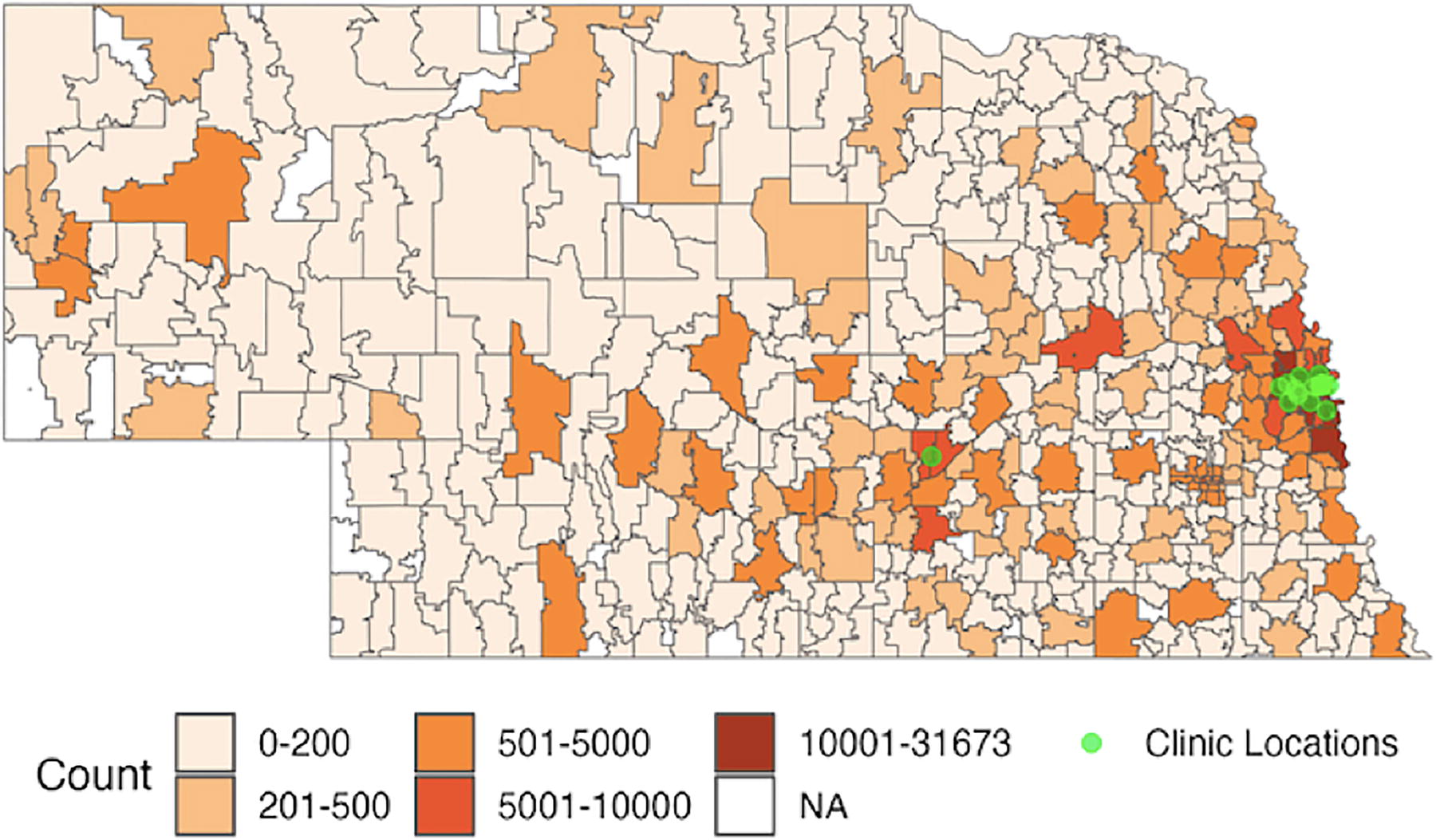
Nebraska map showing visit counts from each zip code utilizing telehealth in this study. e-Visits, e-consults, audiovisual, and audio-only visits are included. Clinic locations are also shown.
Top Specialties Ranked by Total CO2 Avoided
The number of total telehealth visits from January 2019 to January 2022 was calculated per specialty. Patient zip codes were used to estimate the mileage avoided by participating in telehealth, as opposed to traveling to an in-person appointment and converted to CO2 emissions. The top 15 CO2-saving specialties are reported.
Telehealth Appointments and CO2 Avoided per Year
The number of telehealth appointments per year was calculated. CO2 emissions per year and average CO2 emissions saved per trip each year are reported.
The total amount of estimated mileage saved through the utilization of telehealth was 6,634,263.02 miles. This accounts for the distance to and from the location where an in-person appointment would have occurred. The average estimated mileage saved per telehealth visit was 30.96 miles. Specialties with the highest amount of estimated mileage saved were family medicine (766,606.19 miles), endocrinology (744,374.61 miles), infectious disease (711,413.95), behavioral health (428,258.83), psychiatry (425,336.09), and psychology (420,727.64; Table 1). The specialties with the lowest mileage avoided were occupational medicine, pathology, pediatric hematology–oncology, social work, physician assistant, and pediatric gastroenterology, all with <100 miles avoided.
An estimated 2,653.704 metric tons of CO2 were saved over this period due to telehealth usage. An average of 12.38 kg of CO2 was avoided with each telehealth visit. The medical specialty that saved the most CO2 with telehealth visits was family medicine, saving an estimated 306.64 metric tons (Table 1, Fig. 1). Other top specialties included endocrinology (297.75 metric tons), infectious disease (284.57 metric tons), behavioral health (171.30 metric tons), psychiatry (170.13 metric tons), and psychology (168.30 metric tons; Table 1, Fig. 1). Neurology, gastroenterology, and IM were also among the highest CO2-saving specialties (Fig. 1).
Discussion
This study demonstrates the capability of the NM health care system to rapidly adjust to an emergency pandemic by drastically increasing the use of telehealth, which also avoided thousands of tons of transportation-associated CO2 emissions. These data are unique as they evaluate CO2 emissions avoided by specialty across an entire hospital system in a primarily rural state. NM, the major health care system for the state of Nebraska, increased telehealth appointments during the height of the pandemic by more than 22,000%. This demonstrates that the infrastructure is in place for rapid expansion of telehealth services.
Expansion of telehealth services occurred across the country during the pandemic, similar to the patterns observed at the NM system. One large study of 16.7 million insureds found that the weekly number of telemedicine visits increased 23-fold compared with prepandemic times. 16 Telehealth expansion at NM far exceeded this, with a 221-fold increase from 2019 to 2020 (Table 2). The use of telemedicine was one factor contributing to reduced vehicles on the road, alongside general pandemic precautions. Nationwide telehealth utilization likely contributed, in some form, to the 5.4% reduction in CO2 emissions seen during the leading months of 2020. 17 Additionally, a 25.5% reduction in nitrogen dioxide (NO2) was seen during the COVID-19 pandemic, largely attributed to reduced vehicular traffic. 18 A decrease in fine particulate matter was also observed during this time, which was more pronounced in urban areas. 18 Increased levels of NO2 and particulate matter are associated with adverse health outcomes. At a local level, this has been shown to disproportionately affect non-Hispanic black and Hispanic/Latino children, who experience higher exposure to pollutant concentrations and higher rates of asthma exacerbation. 19
The ability to conduct telehealth in a state like Nebraska is a considerable advantage to patients. Nebraska is the 16th largest state in the country by square miles but 37th when ranked by population, leaving many rural counties sparsely populated. With a lack of population comes a shortage of physicians. For example, as of 2020, there were 13 counties in the state without a primary care physician, which includes family medicine, IM, obstetrics/gynecology (OB/GYN), and pediatrics. 20 For patients living in these counties, telehealth may be a realistic avenue to receive high-quality health care while cutting down travel expenses and CO2 emissions. This also means more accessible health care as patients would not have to leave their daily responsibilities to travel for an appointment. Chair of the American Telehealth Association, Dr. Joseph Kvedar, identifies telehealth as a potential bridge to overcome barriers to health care, such as transportation. 21 A barrier specific to telehealth is access to the internet and the capability to operate necessary equipment. In 2021, 11.9% of Nebraskans lacked access to a home internet subscription. 22 This has decreased since 2019 but still represents a significant barrier to engaging in telehealth.
In total, over an estimated 2,500 metric tons of CO2 were avoided from January 2019 to January 2022 by Nebraska residents utilizing NM health care services. For reference, the average passenger vehicle in the United States emits approximately 4.5 metric tons of CO2/year. 10 The CO2 saved by telehealth at NM is approximately equivalent to removing 585 passenger vehicles from Nebraska roads for a year. For additional reference, the typical American household produces 3.58 metric tons of CO2/year. 10 The CO2 emissions prevented by NM telehealth from 2019 to 2022 are equivalent to the CO2 produced by 741 households using natural gas annually.
While vehicular transport is a producer of CO2 emissions associated with telehealth, there are other aspects of the practice that also contribute to total emissions. Emissions associated with the use of computer equipment and internet bandwidth also contribute, although they were not assessed in this study. A large United Kingdom meta-analysis found that the carbon footprint of telemedicine equipment is much smaller than the carbon associated with travel. 23 One study from Sweden found that telemedicine equipment was responsible for 1.86–8.43 kg CO2. 24 In this study, the upper and lower bounds differ due to additional video equipment being utilized for the larger emissions. In either case, the CO2 production is offset by mileage saved when the patient had to travel over 2.24 (lower bound) and 4.47 miles. 24 Using this study and the other referenced as a rough estimate, the average mileage saved of 15.48 miles outweighs the CO2 that would be produced from the videoconferencing and computer equipment.
As shown in this study, telehealth is an effective CO2 emission-reducing strategy. However, telehealth cannot replace in-person medicine and is more applicable to some specialties than others. Telehealth lends itself more readily to specialties that rely less heavily on an in-person physical exam. For example, behavioral health, psychiatry, and psychology, where physical exam is less critical, were all in the top 10 highest CO2-reducing specialties in our study. When considering telehealth as a patient and physician, one may be concerned that the quality of care could suffer. A large meta-analysis studying eight systematic reviews found that telemental health services generally did not significantly differ from in-person interventions. 12 The general efficacy of transitioning in-person mental health care to telemental health care is likely a contributing factor to the results of this study, in which three mental health specialties appear in the top 10 CO2 savers.
Many additional opportunities for health care systems to reduce GHG emissions exist. One of these is the recycling of single-use procedural material. One study found potentially recyclable waste in the operating room in laparoscopic cases varies from 2.7 to 4.25 pounds. 25 Longer and more complex surgeries can generate upwards of 200 pounds per case, and the operating rooms and labor and delivery suites account for over 50% of all hospital waste. 26 Waste reduction in the health care settings offers a worthwhile avenue to further augment the health care sector’s contribution to GHG emissions.
In this study, the family medicine specialty was responsible for the most telehealth visits, the most mileage saved, and thus the most CO2 emissions avoided. Family medicine is a broad specialty that covers acute and chronic illness, as well as pediatrics and OB/GYN. The diversity of the specialty itself may account for the high number of telehealth visits. Also, in Nebraska, there are 838 family medicine/general practice physicians per 100,000 population, the highest general practice specialty per capita rate in the state, likely a contributing factor to the family medicine telehealth numbers. 20
Interestingly, IM, another primary care specialty, was among the leader in telehealth visits with 17,119 in the defined period, which ranks 5th among the specialties. However, the mileage and CO2 saved were ranked 9th in these compared with other specialties. One explanation is that patients engaging in IM telehealth visits live closer to the location where they receive in-person care. Likely, there were more visits in the Omaha and Lincoln areas, as this is where most IM physicians practice. In fact, there are only four counties in Nebraska that have more than 20 IM providers per 100,000 population. 20 These counties are Brown, Hall, Holt, and Douglas County, where Omaha is located. 20 These data suggest that rural patients access telehealth medical care through family medicine physicians at a higher rate compared with IM physicians.
Limitations
There are limitations of this study that must be acknowledged, as they would influence the results. Distances calculated are estimates, as centroid zip codes were used as starting points instead of home addresses, and Euclidean distance was calculated as opposed to road distance. As previously stated, the emissions associated with computers and videoconferencing were not calculated in this study. Additionally, we assumed equal emissions based on mileage for all vehicles. This may overestimate CO2 emissions in some cases such as electric vehicles and may underestimate in other cases such as diesel-powered vehicles. Another factor that may result in an underestimation of emissions avoided is that this study did not consider physicians engaging in telehealth from their homes, instead of driving to their health care facility.
In this study, patients whose home zip code was out of state were not included. This may affect the overall results in conflicting ways. For one, out-of-state patients may have driven to their appointments, which would add to CO2 emissions avoided, leading to an underestimate of CO2 saved. However, some may have flown by plane, which is responsible for 53 pounds of CO2/mile, as compared with 400 g/mile driven in a standard passenger vehicle. 27 This means patients who would otherwise fly to an NM appointment account for a much larger reduction in CO2 emissions avoided.
Conclusions
In conclusion, this study demonstrated the ability of NM to rapidly expand telehealth services in the face of a global pandemic. This practice was beneficial to decreasing the spread of disease and reducing the CO2 emitted by transportation to appointments. Additional NM/UNMC goals for reducing emissions include cutting emissions by 154 K metric tons of CO2 to achieve net zero building emissions, net zero water use, and increasing waste diversion to achieve net zero. 28 Reducing CO2 emissions created by health care is a worthy goal, as the Earth’s warming is attributable to rising CO2 levels. Increases in global temperature and unpredictable weather patterns, caused by CO2, are detrimental to human health. Telehealth proves an invaluable health care tool that can improve care access while mitigating CO2 emissions, slowing global warming, and reducing its harm to Earth’s inhabitants.
Footnotes
Authors’ Contributions
A.B. (corresponding author): Conceptualization, methodology, project administration, visualization, writing—original draft, and writing—review and editing. S.M.: Investigation, methodology, software, formal analysis, visualization, and writing—review and editing. E.K.: Conceptualization, project administration, supervision, and writing—review and editing. H.L.: Investigation, formal analysis, software, visualization, and writing—review and editing. C.S.: Data curation and writing—review and editing. N.T.: Data curation and writing—review and editing. J.E.B.: Conceptualization, funding acquisition, methodology, project administration, resources, supervision, and writing—review and editing.
Author Disclosure Statement
No conflicts of interest to disclose.
Funding Information
This project was funded by the Claire M. Hubbard Foundation.