
Abstract
Background:
The COVID-19 pandemic significantly impacted patients with chronic diseases (CDs), disrupting in-person consultations and health care services. In response, telemedicine was rapidly adopted to maintain continuity of care, especially in tertiary hospitals such as the Clinical Hospital of the Ribeirão Preto Medical School at the University of São Paulo, which became a leader in telemedicine in Brazil. The objective of this study was to describe the hospital’s experience with telemedicine for managing CDs during the COVID-19 pandemic and evaluate its impact on hospital admissions and mortality.
Methods:
We conducted a retrospective cohort study analyzing 614,367 consultations from 2020 to 2021. Consultations were categorized as in-person or telemedicine, and patients with more than four consultations annually were included. Data were retrieved from electronic health records, and outcomes of interest included hospital admissions and mortality within 3 days of consultation. Telemedicine intensity was assessed by the percentage of teleconsultations per patient.
Results:
Of the 614,367 consultations, 52% met the inclusion criteria, representing 36,033 patients. The percentage of teleconsultations was 36.1%, with higher rates in 2020 (48.0%) compared with 2021 (28.8%). Psychiatry had the highest rate of teleconsultations (53.5%), while oncology had the lowest (11.2%). Patients with teleconsultations had lower hospital admission rates (0.15% for the Charlson Comorbidity Index [CCI] of 0) compared with in-person consultations. Mortality was inversely related to the intensity of telemedicine use, with teleconsultation rates above 16.7% associated with a significant reduction in mortality across all CCI levels.
Conclusion:
Telemedicine proved to be a crucial tool during the pandemic, restoring access to care and reducing hospital admissions and mortality for patients with CDs. Future studies using artificial intelligence techniques will further explore the impact of telemedicine on chronic disease management across specialties.
Introduction
The COVID-19 pandemic significantly impacted patients with chronic diseases (CDs), affecting both the management of these conditions and the severity of outcomes. Due to the closure of services and the reallocation of resources to the pandemic response, treatment interruptions and limited access to health care worsened the situation for these patients. 1 The adoption of telemedicine technologies played a crucial role in maintaining continuity of care during the pandemic and has shown promise in enhancing patient engagement and adherence. 2
Two distinct phases characterized the COVID-19 pandemic: the first phase (2020 to early 2021) focused on nonpharmaceutical measures such as social distancing and quarantines due to the absence of vaccines. During this phase, there was high mortality and health care system overload, with limited emergency treatments and the emergence of concerning variants such as Alpha. The second phase (mid-2021 to 2022) saw the introduction of vaccines, which reduced hospitalizations and deaths, though new variants such as Delta and Omicron challenged their effectiveness. The easing of restrictions led to new infections, while booster vaccination campaigns sought to curb the more transmissible variants. However, vaccine access inequality prolonged the crisis in distinct regions worldwide. 3
In Brazil, regulation of telemedicine was first attempted before the COVID-19 pandemic through resolution no. 2,227/2018 from the Conselho Federal de Medicina, but some concerns regarding its implementation led to its withdrawal, creating a regulatory gap. 4 During the pandemic, the Brazilian government approved ordinance no. 467/2020, allowing the use of telemedicine on an emergency basis, facilitating the continuity of health care amid restrictions. 5 After that, the Health Ministry regulated telemedicine with ordinance no. 1.348/2022. 6 However, digital exclusion and socioeconomic inequalities, particularly among vulnerable populations, represent significant barriers to accessing telemedicine. 7
The Clinical Hospital of the Ribeirão Preto Medical School at the University of São Paulo, a tertiary reference for 3.5 million individuals in the northeastern area of São Paulo state-Brazil, played a crucial role in tackling the COVID-19 pandemic. With a dedicated, continuously improving electronic medical record (EMR) system, the hospital quickly adopted telemedicine to mitigate the impact of interrupted in-person care, being the Brazilian hospital that had done the most significant number of telemedicine consultations in 2021. 8 This article describes the hospital’s experience managing CDs with telemedicine during the two phases of the COVID-19 pandemic in a Brazilian public tertiary hospital.
Methods
TYPE OF STUDY
We conducted a retrospective cohort study. We retrieved all outpatient consultations documented from May 1, 2020, to December 31, 2021, in our institution. We excluded consultations that did not meet the criteria for CDs: they are permanent, leave residual disability, are caused by nonreversible pathological alteration, require special training of the patient for rehabilitation, or may be expected to require a long period of supervision, observation, or care. 9 To ensure that we were dealing with CDs, we determined the number of consultations per patient and limited the analysis to patients with more than four consultations in the year. In addition, we limited the number of consultations to less than 24 per year to exclude cases where more intensive follow-up would not influence the impact of teleconsultation.
DATA RETRIEVAL
Since our EMR follows the structure of relational databases, we first extracted the information related to teleconsultation and merged it with other datasets to prepare the dataset with the final variables of interest.
TELEMEDICINE INTERVENTION
We implemented specific forms to document telemedicine consultations, manuals for doctors and patients, and a patient consent form for using the technology. The hospital also conducted training sessions and launched a communication campaign to inform patients. As part of the protocol, the hospital administration selected “key-doctors” to communicate with central administration and classify both clinics and patients. They categorized clinics and patients into three levels: (1) requires immediate care, (2) can be postponed for a short period, and (3) can be delayed longer without serious complications. 8
A tutorial for using the teleconsultation form guided how to access the form in the EMR, register patient information, document contact attempts, and add relevant clinical data. It also emphasized the need to record all teleconsultations in the patient’s EMR, including information about the responsible party, clinical evolution, and any advice provided. All health care professionals obtained patient consent for data registration, ensuring proper documentation to guarantee the continuity and quality of care. 8
As the intervention variable, we characterized the consultations as in-person and teleconsultation. For those who underwent teleconsultations, we generated a continuous variable representing the percentage of teleconsultations relative to the total number of consultations. Subsequently, we categorized this information into quartiles to create a graph.
OUTCOME
We constructed a binary-derived variable encoding hospital admission within three days after a consultation. We retrieved the available mortality information from our electronic health record, deriving a binary variable.
POSSIBLE CONFOUNDERS
We extracted data related to demographic variables (gender, age, race, and marital status). Based on the International Classification of Diseases 10, we calculated the Charlson Comorbidity Index (CCI). 10 We also classified the patients according to year (2020 vs. 2021) and their follow-up area. Using the patient’s address, we extracted data related to the geographic location of their municipality of origin for geospatial analysis. We extracted data related to the population distribution and the number of hospital beds from Health Department XIII of the State of São Paulo.
STATISTICAL ANALYSIS
The sample size was restricted to a convenience sample. We presented categorical variables as percentages, quantitative variables as means, and standard deviations as measures of central tendency. We use the chi-square test for differences among groups to compare categorical variables. For unpaired continuous variables, we use Student’s t-test or analysis of variance as appropriate, applying the Bonferroni post-test for multiple comparisons. We used STATA version 15 for analysis and graphical plotting.
ETHICAL APPROVAL
The hospital’s research ethics committee approved the study, waiving the need for informed consent due to its retrospective nature. The study is registered in the National Research Ethics Commission, linked to the National Health Council under CAE 64511222.3.0000.5440.
Results
We included 614,367 consultations from January 2020 to December 31, 2021. We excluded 297,695 (48%) consultations for not meeting the inclusion criteria—92,128 (15%) conducted during the first 4 months of 2020 because teleconsultation had not yet been implemented at the institution, 28,756 (5%) that did not meet the criteria for CDs, 105,122 (17%) for patients who had fewer than four consultations in the year, and 71,689 (12%) for patients who had more than 24 consultations. Ultimately, we enrolled 216,672 (52%) consultations, corresponding to 36,033 patients.
There was no difference between the years regarding gender, age, marital status, CCI, or geographic distribution. Only 34.2% of the patients had a CCI greater than or equal to 2. The total percentage of teleconsultations was 36.1%. This rate was higher in 2020 (48.0%) than in 2021 (28.8%)—p < 0.01—Table 1 and Fig. 1. As shown in Fig. 1(A, B), there was a decrease of approximately 40% at the beginning of the first phase of the pandemic compared to the average of the first quarter of 2020.
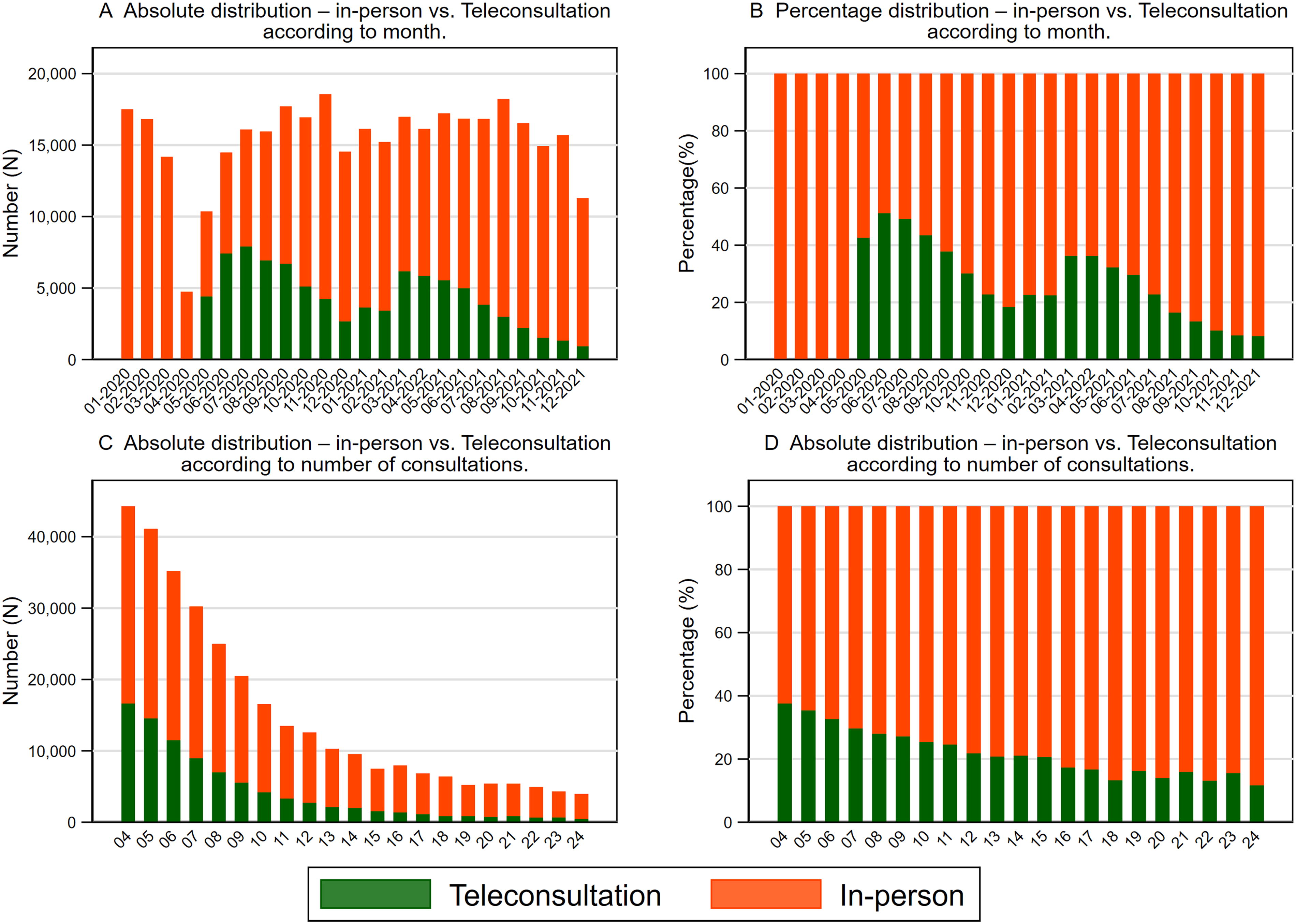
Absolute and percentage distribution according to the type of consultation (in-person vs. teleconsultation) by follow-up period
Socio-Demographic Variables and Type of Consultation for Patients with Chronic Diseases Followed at the Hospital for the Total Number of Patients and According to the Follow-up Year (2020 and 2021)
Psychiatry (53.5%) led the number of teleconsultations, followed by Neurology (38.8%), Pediatrics (35.9%), Genetics (35.6%), Internal Medicine (34.8%), Gynecology (30.8%), Surgery (29.9%), Ophthalmology and Otorhinolaryngology (20.2%), Orthopedics (12.4%) and, Oncology (11.2%). There was no difference between the years (data not shown).
Most patients were from the Health Department XIII of the state of São Paulo (79.9%)—Table 1. In Fig. 2, we present the geospatial distribution of the population, the number of beds, and the percentage of teleconsultations performed. The highest concentration of teleconsultations was from the Vale das Cachoeiras (III in Fig. 2) sector, the region with the lowest population density and the minor distribution of hospital beds.
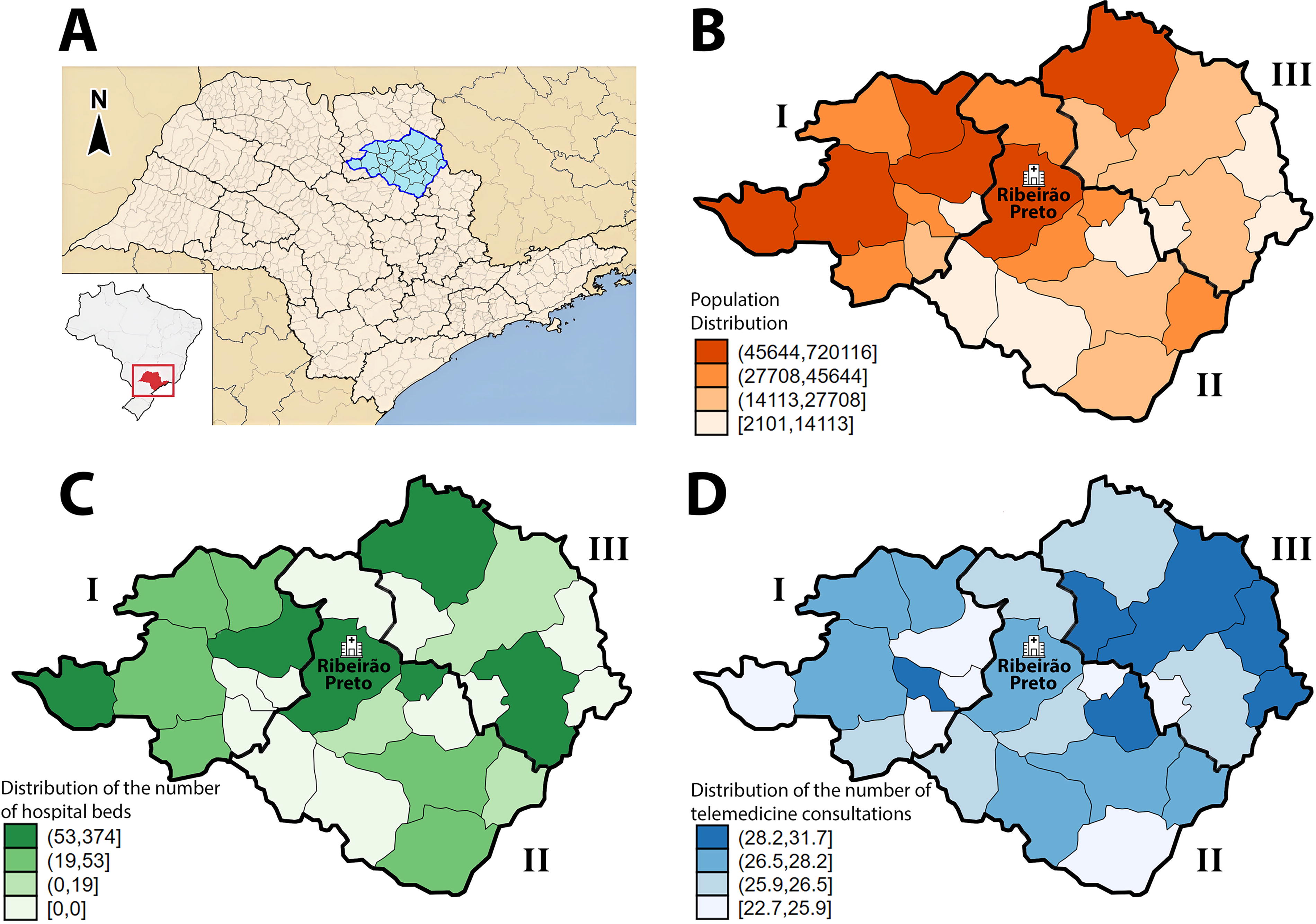
Geographic distribution of parameters of interest—
The percentage of hospital admissions within three days following a consultation varied according to the type of consultation and the CCI. Patients seen through teleconsultation had a hospital admission rate of 0.15% when the CCI was zero. This rate increased to 0.5% when the CCI was 2—Fig. 3.
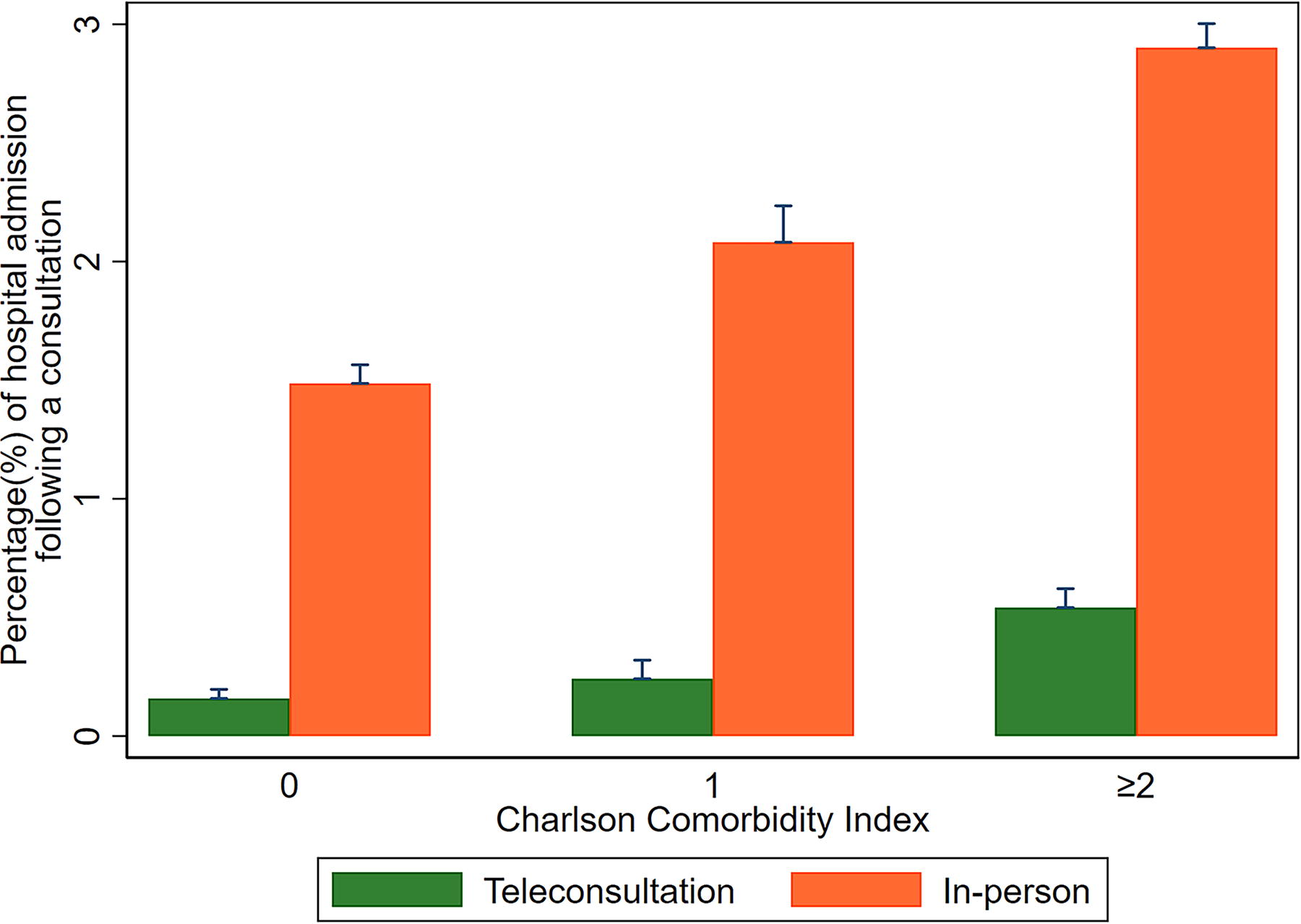
Percentage of hospital admissions according to the type (in-person or teleconsultation) and the Charlson Comorbidity Index.
In Fig. 4, we present the mortality percentage according to the CCI and the quartiles of teleconsultation percentage. We observed that levels above 16.7% of teleconsultations are associated with mortality reduction—from 2.9% to 1.7% with CCI 0, 7.6% to 4.7% with CCI 1, and 17.1% to 10.8% in CCI 2.
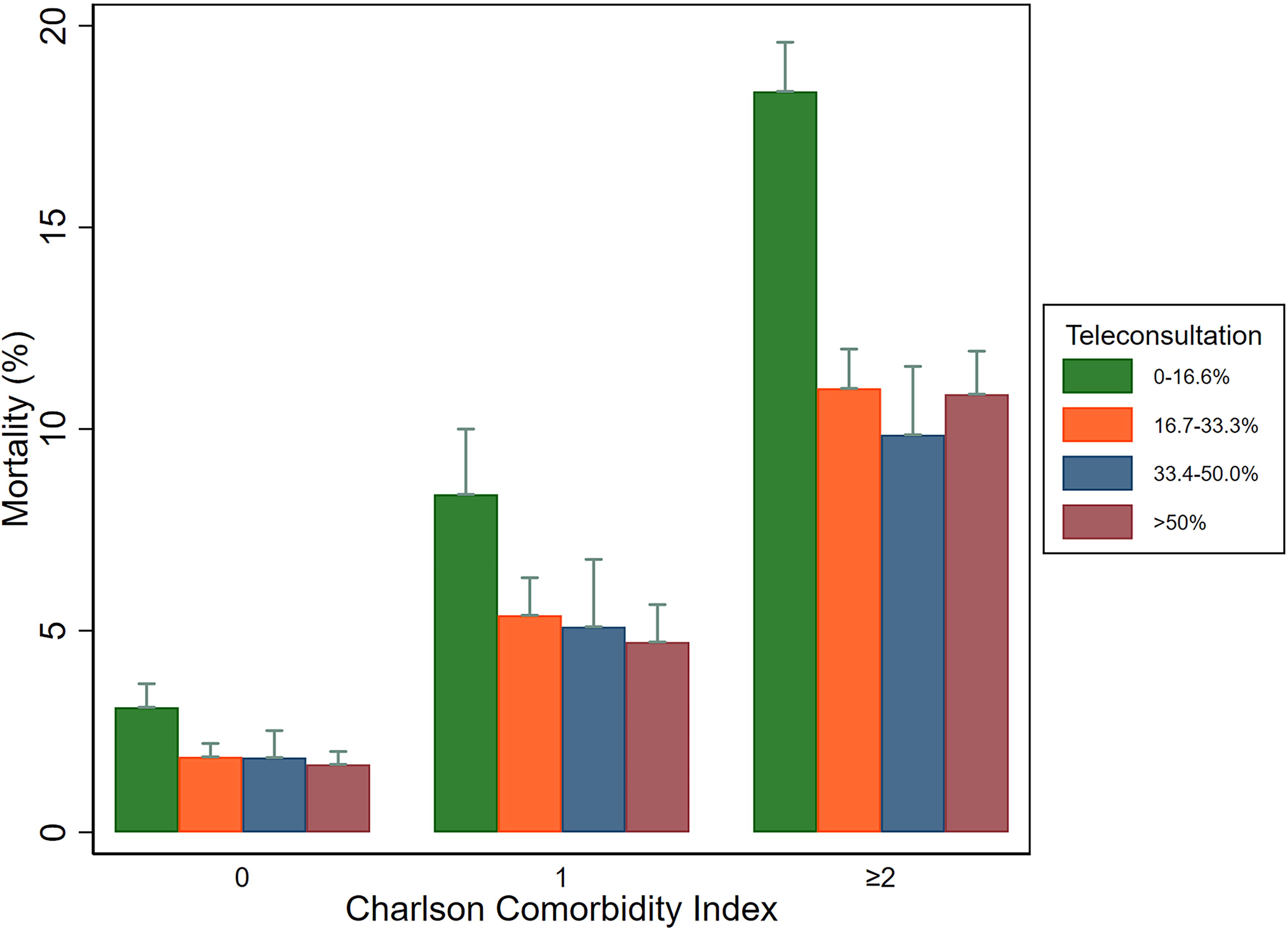
Percentage of mortality according to the intensity of teleconsultation and the Charlson Comorbidity Index.
Discussion
The rigorous criteria for selection, training, and documentation for the teleconsultation strategy of our institution were well adhered to by the health care professionals involved. It ensured access for patients from less populated areas with fewer hospital resources. In addition, it allowed the institution to maintain an outpatient consultations capacity similar to the average recorded in the quarter preceding the pandemic’s start. It proved safe, presenting much lower hospital admission rates than in-person consultation. Finally, a percentage exceeding 16.7% of teleconsultations was associated with lower mortality.
Luciani et al. analyzed the impact of the COVID-19 pandemic on CD services in the Americas, revealing that over half of the countries lacked comprehensive guidelines, essential medicines, and technologies in primary care. The pandemic significantly disrupted services, with only 34% of countries reporting normal outpatient functions, as many health care staff were redirected to COVID-19 efforts. Countries employed mitigation strategies such as telemedicine, but challenges such as limited access to technology persisted. 11 Byun et al. showed a 13.4% reduction in outpatient visits in 2020, with pediatric departments seeing a 37.5% drop and internal medicine consultations falling by 10.2%. Visits for infectious diseases decreased by nearly 50%, while non-infectious diseases such as cancer and circulatory conditions experienced smaller declines. 12
Our institution adopted teleconsultation to minimize harm and prioritize safety for patients with CDs. In this context, it is essential to note that the intervention involved defining which patients would be candidates based on the clinic they attended and their profile, as determined by our “key-doctors”. In addition, we trained all professionals to use a dedicated teleconsultation tool integrated into the EMR. This characterization of the patients implies caution when comparing our findings with other data in the literature, as it is necessary to assess whether there was a preselection of the patient profile for those who would be treated using this technology. 7
As expected, adherence from the patient follow-up areas was variable, likely reflecting the nature of the clinical condition. For example, we had a higher percentage of teleconsultations in the Psychiatry department (53.5%) and a lower percentage in the Oncology department (11.2%), though there was no variation across the years. We also evaluated the specialties within each area. As previously demonstrated, some cardiology (internal medicine) conditions had a higher percentage of teleconsultations than others, but again, there was no variation over the years. Initial analyses are already being developed for each area and specialty, taking their specific characteristics into account, and will be the subject of future communications. 13
Our data indicate that the acceptance of teleconsultation by health care professionals was higher during the first phase of the pandemic when the risk was more significant. The advent of vaccination characterized the second phase and our institution guaranteed vaccination for all health care professionals by our institution. 8 Gonçalves et al. systematically reviewed the use of telehealth for managing CDs during and after the COVID-19 pandemic. They concluded that it has been well-received by health care professionals, with ease of use being a critical factor for adoption. 14 These findings align with our experience, as all efforts made for staff training and structured teleconsultation forms in the institutional EMR were undoubtedly responsible for the acceptance.
The patients’ CCI reflected the “key-doctors” priority classification. The CCI has already proven suitable for other studies conducted within the institution. 15,16 The association of the CCI with the classification performed by our “key-doctors” opens the possibility that it could be a quick and practical tool for prioritizing patients for teleconsultation, especially in disaster situations such as COVID-19, which may occur again.
We evaluated the geospatial behavior of population density, the number of hospital beds, and the percentage of teleconsultations performed, to characterize the population’s access to continued care. The pandemic exposed and deepened the region’s vast health care inequalities, particularly affecting the poorest populations who depend on fragile public health systems. 17 Bernal Lara et al. examined how the COVID-19 pandemic disrupted non-COVID-19 health services in Brazil, Ecuador, Mexico, and Peru, focusing on CDs. In Brazil, while the reduction in hospitalizations was less pronounced than in Ecuador, Mexico, and Peru, mortality rates for CDs, such as cardiovascular diseases, diabetes, and renal failure, surged by 27%. The poorest states in Brazil were disproportionately affected, experiencing more significant increases in mortality compared to wealthier regions, underscoring existing health care inequalities. The study estimates that approximately 96,000 deaths across these countries could have been prevented with better access to timely care. 18 Our data show that less populated areas with fewer resources had access to care ensured through teleconsultation.
Telemedicine was crucial in restoring the capacity to provide care to levels close to those observed before the pandemic. According to Stachteas et al., telemedicine offset about two-thirds of the decline in total consultation volume in the United States, allowing a significant recovery in outpatient care during the health crisis. 19 Meanwhile, Byun et al. found that, in South Korea, internal medicine outpatient care returned to prepandemic levels. 12 Herrera et al. reported that Latin America and the Caribbean faced significant disruptions in routine health services during the pandemic, especially in primary care. However, several strategies were implemented to recover these services, including telemedicine. The recovery varied across countries, with some services for noncommunicable diseases being restored, but the overall pace of recovery was slow, especially in underserved areas. 20
We demonstrated that hospital admissions following teleconsultation are lower than in-person despite CCI. Teleconsultation consistently demonstrated reduced hospital admissions, with effects ranging from a 40% decrease in specific populations (e.g., diabetic patients) to two-thirds of overall expected admissions prevented by telemedicine in chronic disease management. 12,14,19
Our data show a reduction in mortality when the percentage of teleconsultation is higher than 16.7%. We should evaluate mortality carefully, considering that we studied overall mortality, which includes those related to COVID-19 infection. Despite the limitation in estimating a mortality rate related explicitly to CDs, the finding of a cut-off in the intensity of teleconsultations, independent of the CCI, can be an argument to support causal inference.
LIMITATIONS
Our study has several limitations, starting with the retrospective nature of its design. However, the careful documentation of teleconsultations and the training of health care professionals mitigate this effect. It is also important to emphasize that the aim of this study is to describe the institution’s experience, which has the most significant impact on telemedicine when considering a single hospital. Future studies will be needed to characterize initiatives pertinent to each area and specialty, whose initial results are already underway. The use of artificial intelligence techniques could contribute to a more in-depth analysis. It is also worth noting that we could only analyze overall mortality, as it is complex to attribute mortality to specific diagnoses (CDs).
Despite the positive feedback on telehealth’s ability to provide continuous care without face-to-face contact, several barriers remain, including technological challenges, low digital literacy, connectivity issues, and difficulties in performing comprehensive physical exams remotely. The Brazilian Health Ministry is addressing these barriers, enhancing infrastructure to telehealth’s continued success through ordinance no. 4.160/2024. 21 According to the São Paulo State Health Department, although our institution operates at the tertiary level, it plays a role in encouraging the structuring of the entire health care network. Our telemedicine initiative is another successful experience in this context. 16,22,23
In summary, our experience with telemedicine for the follow-up of specific diagnoses (CDs) was significant, ensuring access and restoring the institution’s capacity to provide care during the COVID-19 pandemic. In addition, the intensity of telemedicine follow-up was associated with low percentages of hospital admissions and mortality.
Authors' Contributions
All authors contributed to the conception of the project, the conduct of the research, data analysis, and the writing of the manuscript.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.