
Abstract
Background:
The use of virtual care interventions in correctional facilities has increased in recent years owing to the impacts of the COVID-19 pandemic. However, the literature shows variability in the application and measurement of efficacy, effectiveness, and efficiency of virtual care interventions. This systematic review addresses this gap in evidence and provides an overview and appraisal of the methods and measures used to evaluate these aspects of virtual care interventions in correctional facilities, using a modified conceptual framework by the World Health Organization (WHO).
Methods:
We conducted a systematic review using a narrative synthesis approach. Comprehensive searches were performed in PubMed, Scopus, and Web of Science for peer-reviewed studies published in English between 2014 and 2024. The Joanna Briggs Institute Meta-Analysis of Statistical Assessment and Review Instrument was used to assess the methodological quality of included studies.
Results:
Twenty-one studies were included, and most were conducted in the United States and focused on synchronous modality for adult males. None of the studies explicitly defined the efficacy, effectiveness, and efficiency of virtual care interventions. The concept of effectiveness was the most frequently explored, and aligned best with WHO’s conceptual framework, whereas efficiency was the least explored. The most common evaluation measures were clinical effectiveness, user satisfaction, and interexaminer agreement.
Conclusions:
This review highlights the need for adopting a unified framework for evaluating virtual care in correctional facilities that can standardize evaluation metrics and improve resource allocation, ultimately enhancing patient outcomes by ensuring that virtual care interventions are efficacious, effective, and efficient.
Background
Globally, over 11.5 million people are incarcerated in correctional facilities, 1 with the highest prison population and rates of imprisonment in the Americas, Europe, and Oceania. 2,3 The number of people living in correctional facilities is increasing. For example, since 2000, Oceania has experienced an 82% increase in its overall prison population. 4 The high number of people in custody and the increasing trend of incarceration are major concerns in the public health field.
People in custody bear a substantial disease burden compared with the general population. They experience higher rates of mental illness and substance use disorders, communicable and noncommunicable diseases, and chronic illnesses, such as major depression, hepatitis C, HIV infection, and cardiovascular disorders. 5 –10 These health disparities stem from socioeconomic and demographic disadvantages experienced throughout their life course. In particular, Indigenous, racial, and ethnic minorities are disproportionately impacted by incarceration. 9,10 Despite this increased burden of disease, people in custody have historically been marginalized with respect to health care, as health service delivery in prisons often does not meet the health needs of this group. 9 Some correctional facilities transfer patients to local public hospitals for ongoing care. These transfers pose additional challenges and expenses, including the costs associated with patient transportation and heightened security risks. These risks affect not only the security personnel and hospital staff but also the broader community, particularly during the transfer of high-security prisoners. 11 –13 In an attempt to address the existing health inequities experienced by people in custody, a number of innovative modalities of health care delivery, including virtual care, have been implemented in correctional facilities. 14,15
Virtual care, telemedicine, digital health, and telehealth are terms that are often used interchangeably in the literature. 6,16 –18 According to the Toronto Women’s College Hospital for Health System Solutions and Virtual Care, virtual care is defined as “any interaction between patients and members of their circle of care that occurs remotely, using any form of communication or information technology, to facilitate or maximize the quality and effectiveness of patient care.” 19 It is a broad term that encompasses diverse forms of health services that occur outside traditional face-to-face clinical encounters, including telephone calls, video visits, secure messaging, and email consultations. For this review, we used the term “virtual care” as an umbrella term to encompass all these modalities. 20,21
Virtual care is primarily delivered synchronously or asynchronously. Synchronous modalities involve real-time interaction through telephone, chat, or videoconferencing, whereas asynchronous communication is a store-and-forward method that collects text, audio, or video for later use by clinicians. The concept of virtual care not only covers both synchronous and asynchronous modes of patient–provider and provider-to-provider interactions but also the use of virtual reality to simulate care environments. 5,17,22
In everyday use, efficacy, effectiveness, and efficiency are often misunderstood as synonyms. 23,24 In experimental health research, however, the terms are more strictly defined: efficacy refers to the measure of how an intervention performs in ideal conditions, effectiveness is a measure of the performance of an intervention in real-world (nonresearch) settings, and efficiency is concerned with measuring the relationship between health service inputs, outputs, and outcomes to achieve the best value for money. 24 –26 In the context of virtual care settings, the World Health Organization (WHO) has provided guidance regarding the meaning, application, and evaluation of efficacy, effectiveness, and efficiency. It outlines a life-cycle approach and evaluation measures for assessing virtual care interventions. The WHO’s conceptual framework aligns the developmental cycle of the intervention with the evaluation stage and includes the assessment of the efficacy, effectiveness, and efficiency of virtual care interventions. 27 However, in correctional facilities, there is a variable application of the three concepts and the measures used to evaluate them. In particular, virtual care evaluations do not employ a life-cycle approach to evaluate efficacy, effectiveness, and efficiency. 6,28 –30
The use of virtual care interventions in correctional systems has increased in recent years owing to the impact of the COVID-19 pandemic. 31 –33 A study highlighted that in June 2020, the COVID-19 infection rate in correctional facilities was 5.5 times higher than in the general U.S. population. 32 This heightened incidence was attributed to the challenges of effectively maintaining social distancing in overcrowded spaces, inadequate ventilation, and substandard hygiene practices. The limited health care resources within these centers, coupled with restrictions on transferring patients to external facilities, led to an increased adoption of virtual care solutions. 11,32,33 Given this increase in the use of virtual care in correctional facilities, it is vital that these interventions are evaluated to ensure their efficacy, effectiveness, and efficiency. To facilitate such evaluation, there needs to be a common understanding of the concepts of efficacy, effectiveness, and efficiency in relation to virtual health care delivery in correctional facilities, and the appropriate metrics to measure these in this context. 28,31 Hence, this systematic review aimed to appraise the literature systematically describing the evaluation of virtual health care delivery in correctional facilities to clarify the methods and measures used to elucidate the efficacy, effectiveness, and efficiency of such interventions.
Methods
A systematic narrative synthesis was conducted, and the findings were reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 34 The protocol for this systematic review was registered on the International Prospective Register of Systematic Reviews (CRD42023454115).
LITERATURE SEARCH
We searched three electronic databases (PubMed, Scopus, and Web of Science) for peer-reviewed studies that evaluated virtual care interventions in correctional facilities. The databases were searched in May 2024. An additional literature search was performed using an internet search engine (Google Scholar, limited to the first 10 pages) to improve the overall coverage of the review. However, a gray literature search was not performed.
While a variety of terms are used in the literature, in this review, the major search concepts that defined the Subject Heading terms and keywords used for the search were virtual care, correctional facility, efficacy, effectiveness, and efficiency. The key search terms and Medical Subject Headings (MeSH) relevant to each concept were developed through an initial review of articles and in consultation with a health sciences librarian at the University of Newcastle. For the purposes of this review, the terms virtual care and telemedicine were used interchangeably to produce an inclusive list of studies. To ensure comprehensive coverage of all the literature, we combined key concepts using Boolean operators and applied relevant truncations (Table 1).
Search Strategy
STUDY SELECTION
Inclusion criteria
Publications were eligible for inclusion if they: (i) were published in peer-reviewed journals; (ii) described primary quantitative, qualitative, or mixed-methods research; (iii) reported on methods and measures used to evaluate the efficacy, effectiveness, or efficiency of virtual care in correctional facilities; and (iv) were published within the last 10 years (since 2014).
While no restrictions were placed on the region where the study was conducted, only articles published in English were eligible for inclusion. Publications describing synchronous or asynchronous (store-and-forward) virtual health modalities were eligible for inclusion. Publications that described studies examining virtual consultations among health professionals were also included. There were no restrictions on the age, sex, ethnicity, or health conditions of the patients included in the studies. Studies conducted in correctional facilities were included. In this review, the definition of “correctional facility” is used broadly to include a range of institutions designated for the confinement of individuals serving sentences, awaiting trial, or otherwise detained. This encompasses prisons, pretrial detention centers (such as jails and remand facilities), and juvenile correctional institutions. 35 We included publications that evaluated the efficacy, effectiveness, and efficiency of virtual care interventions in correctional facilities based on the terminology used by the authors (i.e., if the authors used these terms, the study was eligible for inclusion whether or not the authors’ understanding of these terms corresponded with the WHO definitions).
Feasibility and pilot studies were also included, as we interpreted these as evaluations of efficacy. Similarly, cost-effectiveness studies were included, as we interpreted them to be evaluations of efficiency. Studies that assessed the impact or quality of virtual care in correctional facilities were also included, as we interpreted these as evaluations of its effectiveness. Note that we restricted eligibility to studies published in the last 10 years due to the dynamic nature of the technological applications used in virtual health care delivery.
Exclusion criteria
We excluded literature describing virtual care interventions that were delivered to individuals or groups within the community (i.e., noncorrectional settings); people on probation, parole, or postrelease follow-up; individuals undergoing home detention monitoring; individuals and groups in immigration detention facilities; and prisoners of war. We excluded studies that were limited to a description of a virtual care intervention or model of care but did not provide a comprehensive evaluation of the intervention or clearly articulate the measures used to assess its efficacy, effectiveness, or efficiency. We also excluded studies that used simulations or focused primarily on future intentions, attitudes, and willingness to use virtual care interventions. Non-English literature, secondary research (systematic, scoping, and literature reviews), commentaries, abstracts, editorials, letters, books, posters, protocols, conference proceedings, and opinion pieces were also excluded.
Two reviewers (C.N. and A.L.) independently screened each title and abstract, and the full text of all publications deemed potentially relevant for inclusion after title/abstract screening. Consensus meetings were held after title and abstract screening and later after full-text reviews to finalize the selection of articles to be included in the review.
DATA EXTRACTION AND SYNTHESIS
The following data items were extracted from each article to a data charting form by one of the reviewers (C.N.): title; authors; year of publication; country where study was conducted; study population (age, sex, ethnicity); medical service/condition or discipline; study design; sample size; technological intervention description (synchronous/asynchronous); study aim/objective; duration of study; study timeline; evaluation method; measures of efficacy, effectiveness, and efficiency; other evaluation measures; outcomes; technology used; and additional notes.
ASSESSMENT OF STUDY QUALITY
The methodological quality of each included study was independently appraised by two reviewers using standardized critical appraisal instruments from the Joanna Briggs Institute Meta-Analysis of Statistical Assessment and Review Instrument (JBI-MAStARI). 36
Using the different evaluation checklists in the JBI as a guide, the studies were grouped into the following categories: cross-sectional (n = 11), pre–post (n = 2), qualitative (n = 2), cohort (n = 2), quasi-experimental (n = 1), and economic evaluations (n = 3). Each checklist criterion required a “yes,” “no,” “unclear,” or “not applicable” response. “Yes” meant the criterion had been established through the report description, “No” meant the criterion had not been applied appropriately, and “unclear” meant the criterion was not clearly identified in the report and it was not possible to acquire clarification from the author. The primary reviewer (C.N.) compared the two sets of appraisals. Discordant responses were first discussed by two reviewers. Note that we did not exclude any study based on its methodological quality.
CONCEPTUAL FRAMEWORK AND DATA SYNTHESIS
The included studies were heterogeneous with substantial variability in the measures used to evaluate the efficacy, effectiveness, and efficiency of virtual care interventions in correctional facilities. Therefore, conducting a meta-analysis was not feasible. Considering the diversity of the reported measures, we determined that a conceptual framework was necessary to synthesize the available evidence. Hence, we adapted a conceptual framework developed by the WHO to monitor and evaluate virtual care interventions creating a framework to categorize the concepts and measures described in the included studies. 27 The WHO conceptual framework was deemed most suitable for this systematic review, as it aligns the different stages of intervention maturity with specific evaluation stages, thereby providing a structured approach to assessing the efficacy, effectiveness, and efficiency of virtual care interventions (Table 2). 27
WHO Conceptual Framework Stages
WHO, World Health Organization.
Within the WHO conceptual framework, efficacy corresponds to the pilot stage of a virtual care intervention (Table 2). Within this framework, “Efficacy” is defined as the assessment of whether a digital health intervention achieves the intended results in a controlled research setting. 27 The evaluation stage primarily addresses the question, “Can it work?” The five measurement targets for this stage are user satisfaction, workflow fit, learning curve, performance errors, and reliability. 27
Within the WHO framework, the evaluation of the effectiveness of virtual care aligns with the demonstration stage of digital health maturity (Table 2). “Effectiveness” is defined as the assessment of whether the digital health intervention achieves the intended results in an uncontrolled, nonresearch, or clinical setting. 27 The key question at this stage is, “Does it work?” 27 The two main measurement targets for this stage are changes in process (e.g., time to x), and changes in outcome (e.g., system performance). 27 For this review, changes in process are associated with service delivery improvements in terms of coverage and scale (availability), as well as quality and utilization of services at the client, provider, and system levels. 27 Changes in outcome, on the other hand, relate to improvements in system performance or health outcomes attributable to the intervention.
For this review, the scale-up stage from the WHO conceptual framework was adapted to evaluate efficiency, focusing on the cost measurement targets. “Efficiency” is defined as the measurement of whether health care resources are being used to obtain the best value for money. It addresses the question,” Has the digital health intervention reduced costs associated with the delivery of health services?” The measurement targets for this stage include changes in process and outcome, evaluation of costs (cost reduction and implementation costs), error rates, and the learning curve of users. 27
By employing this as “a priori” framework for our data synthesis, we aimed to assess whether the evaluations described in the included studies aligned with the criteria outlined in the adapted WHO conceptual framework. This structured analysis would determine whether the array of measures discussed in the studies is adequate to successfully evaluate virtual care programs and interventions.
For each study, we assessed whether the evaluation strategy adhered to the relevant measurement targets associated with the evaluation stage, as described in the WHO conceptual framework. For each target measure, we assigned one of the three outcomes: “yes,” “no,” or “unclear.” “Yes” indicated that the criterion had been observed in the study description, while “no” meant the criterion had not been observed in the study description. “Unclear” indicated that the criterion was not clearly identified in the study description. However, four studies 37 –40 that explored more than one concept were not scored against the WHO framework. These studies lacked clarity regarding their evaluation stage, making it difficult to determine whether they were measuring efficacy, effectiveness, or efficiency.
Results
The literature search identified 1,063 articles from electronic databases, of which 382 were duplicates. After excluding duplicates, the titles and abstracts of the remaining 681 articles were screened by two independent reviewers (C.N. and A.L.) in Covidence, and 562 studies were found to be irrelevant. Of the remaining 119 studies, the full text of one study could not be located. After screening 118 full-text studies, 97 were excluded as they did not meet the inclusion criteria for this review. Overall, 21 studies that met the inclusion criteria were included. The study selection process is summarized in the PRISMA flow diagram presented in (Fig. 1).
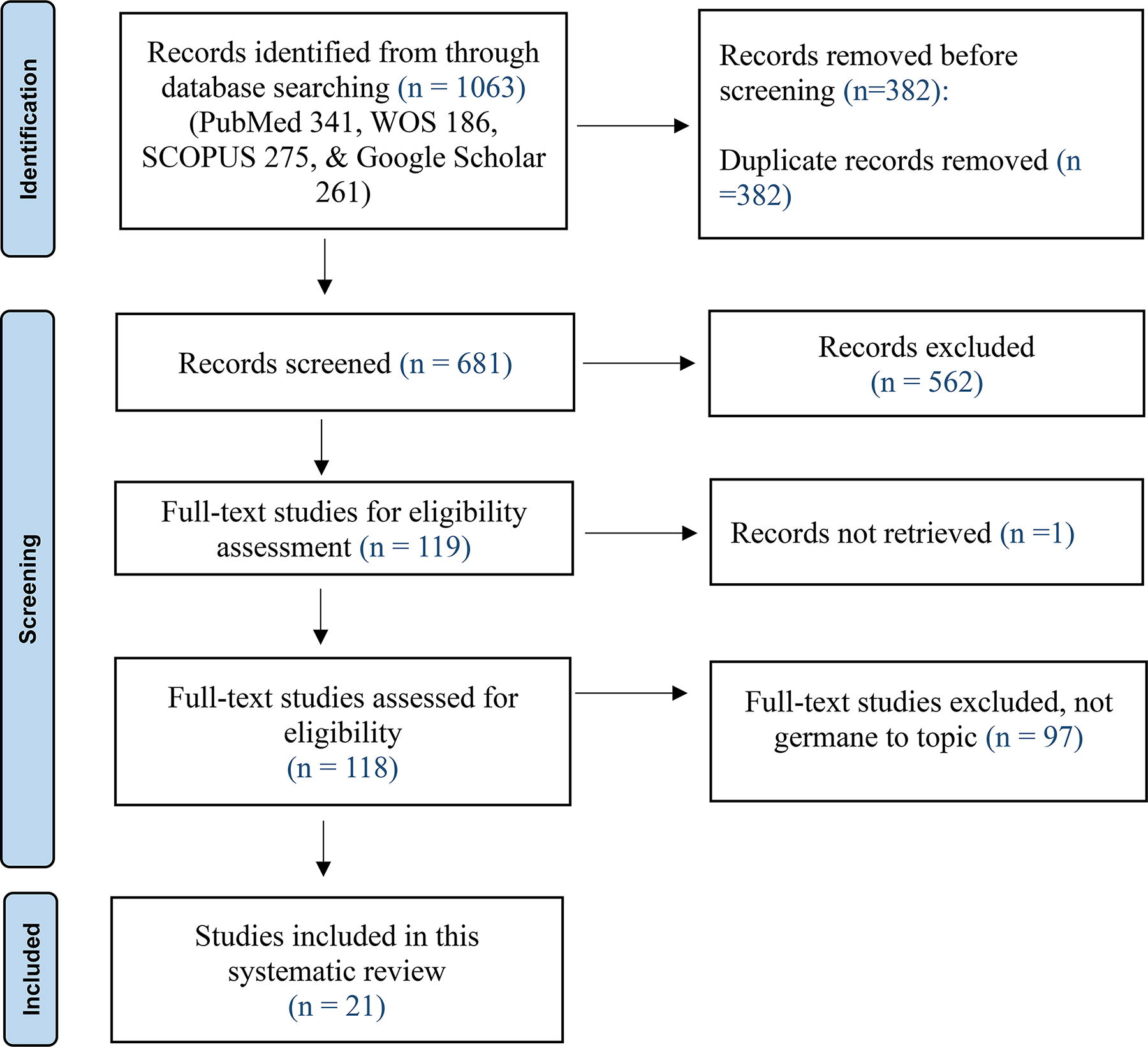
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
STUDY CHARACTERISTICS
The 21 publications included in this review were published between July 2014 and November 2023 and described 10 different types of medical services implemented across nine countries. Most studies (n = 8) were conducted in the United States. 39,41 –47 Three studies were from Australia, 48 –50 three from Spain, 38,51,52 and two from France. 53,54 One study each from Colombia, 37 China, 55 Brazil, 56 South Korea, 57 and Italy 40 was included. All publications retrieved for this review described observational primary research studies, of which 19 37 –47,50 –57 comprised quantitative and two 48,49 comprised qualitative study designs. The most commonly identified modality was synchronous virtual care (n = 14), 38,39,41 –43,45 –51,55,57 followed by asynchronous virtual care (n = 5) 40,52 –54,56 ; two of the studies were hybrid in nature. 37,44 The number of patients in the included studies ranged from 20 to 687, and participants were aged between 15 and 76 years old. Only one study had a female majority, 48 whereas the rest focused primarily on males. Similarly, only one study focused on young people aged 15–19 in custody. 56 The 10 different medical services described in the 21 studies were all related to the delivery of specialist consultations and are presented in (Table 3).
Medical Services Evaluated in the Included Studies (N = 21)
Virtual care services described in the included studies primarily targeted patient care (n = 17). 37 –39,41 –48,50 –52,54,55,57 However, two services were aimed at mentoring and advising primary care providers, 40,49 while two were aimed at providing a second diagnostic and treatment perspective in addition to face-to-face care. 53,56
Thirteen studies reported the technology and peripherals used for delivering virtual care services, 38,42,44 –46,48,50,51,53 –57 which included videoconferencing systems and software for virtual consultations with secure video communication and administrative systems. The peripherals included cameras (intraoral, retinal, general examination, digital, high-resolution close-up cameras), high-definition monitors, personal computers (PCs), tablet PCs with lockdown software, electronic stethoscopes, digital pulse oximetry, electrocardiogram (EKG), and light-emitting diode (LED) illumination systems.
A summary of the characteristics of the included studies is shown in Table 4. The measures included in this table reflect the terminology used by the authors (whether or not it corresponds with the WHO framework).
Summary of the Characteristics of Studies Included in the Systematic Review (N = 21)
CG, control group/comparison group; C-GHQ-12, Chinese version of the 12-item General Health Questionnaire; CVL, community HIV viral load; DAAs, direct acting antivirals; DM, diabetes mellitus; DMFT, Decayed, Missing, and Filled Teeth score; FFC, face-to-face consultations; GP, general practitioner; HCV, hepatitis C virus; HDRS, Hamiliton Depression Rating Score; HIV, human immunodeficiency virus; IG, intervention group; IS, intervention site(s); LDL, low-density lipoprotein; LITD, live interactive teledermatology; MAST, model for assessment of telemedicine; NHS, National Health Systems; OPD, Out-Patient Department; ROI, return on investment; SD, standard deviation; SSA, Stay Strong App; SVR, sustained virological response; SVR12, sustained virological response week-12; TCP, telemedicine clinical practice; TPP, testicular pain and pathology; TSQ, Telehealth Satisfaction Questionnaire; TM, telemedicine; UCP, usual clinical practice.
EFFICACY, EFFECTIVENESS, AND EFFICIENCY OF VIRTUAL CARE INTERVENTIONS
Defining efficacy, effectiveness, and efficiency of virtual care interventions
Analysis of the 21 studies included in the review revealed a lack of consensus regarding the definitions of efficacy, effectiveness, and efficiency. Notably, none of the 21 studies provided explicit definitions of these terms within the context of their evaluation. Three studies 40,47,56 employed these terms interchangeably in the text without differentiation. In 11 studies, the concepts of effectiveness 37,39,42,43,48 –51,57 and efficiency 38,46 were used in relation to the specific outcome measure used in the study. Another seven studies did not define the terms or provide clear explanations of their use in the methodology, but instead referred to the terms efficacy, effectiveness, and efficiency in the abstract of the study 52 or in the discussion, 44,53 –55 or conclusion. 45,56
What included studies purported to evaluate and the methods and measures employed
Of the 21 included studies, the majority (n = 10, 47.6%) were described by their authors as evaluating the effectiveness of virtual care interventions, 42 –44,49 –52,54,55,57 while six (28.6%) were stated to be evaluating the efficacy, 41,45,47,48,53,56 and one (4.8%) reported on efficiency. 46 The remaining four (19.0%) studies were described by their authors as evaluations of a combination of efficacy and effectiveness, 40 as well as efficiency and effectiveness (Table 5). 37 –39
Concepts Observed in the Literature as per Stated by Authors (N = 21)
The measures used to evaluate virtual health interventions described in the included studies are presented in Table 6. The most frequently explored concept in the studies analyzed in this review was effectiveness, and the least was efficiency. Clinical effectiveness was the most common measure, followed by user satisfaction, and interexaminer agreement.
A Summary of the Measures Reported by the 21 Studies a in the Order of Most Used to Least Used
Multiple studies used more than one measure and therefore the total count of measures used is more than 21.
The details of the measures used to evaluate the efficacy, effectiveness, and efficiency of interventions are presented in (Table 7) efficacy measures (Supplementary Table S1), effectiveness measures, and (Supplementary Table S2) efficiency measures. Clinical effectiveness, user satisfaction, and interexaminer agreement are the most commonly explored measures. No common measures have been explored under efficiency.
Description of the Measures Used to Evaluate the Efficacy of a Virtual Care Intervention
Assessment of “efficacy” as per WHO conceptual framework
Of the six studies that purported to evaluate efficacy, only one 41 study explicitly categorized the stage of maturity as the pilot stage. Furthermore, only one study 53 satisfied the criteria described in the WHO conceptual framework (Table 8). The remaining five could not be classified as efficacy studies according to the WHO criteria.
Comparison of Included Studies’ Assessment of Efficacy to WHO Conceptual Framework
N, no; UC, unclear; Y, yes.
Four of these documented performance errors, 41,45,53,56 three reported on user satisfaction, 41,45,53 and less than half reported on workflow fit, 45,53 reliability, 53,56 and learning curve. 45,53 A summary of the analyses is presented in Table 8.
Assessment of “effectiveness” as per WHO conceptual framework
Of the 11 studies 37,42 –44,49 –52,54,55,57 that purported to investigate the effectiveness of virtual care interventions, all documented changes in outcome while six 37,42,49,50,52,54 documented both changes in process and changes in outcome as specified in the WHO framework (Table 9). Notably, one study that explored effectiveness categorized the intervention’s developmental stage as the pilot stage.
Comparison of Included Studies’ Assessment of Effectiveness to WHO Conceptual Framework
Assessment of “efficiency” under the WHO conceptual framework
The evaluation of virtual care efficiency was the least reported concept in the studies included in this review. Only one study purported to assess the efficiency of a virtual care intervention, 46 which did not satisfy the WHO criteria, as it only assessed cost reduction and changes in process/outcome in less controlled environment components, while failing to assess the total cost of implementation, error rates, and the learning curve of users (Table 10).
Comparison of Included Study’s Assessment of Efficiency to WHO Conceptual Framework
QUALITY OF STUDIES
The appraisal of methodological quality was carried out using standardized critical appraisal instruments from the Joanna Briggs Institute Meta-Analysis of Statistical Assessment and Review Instrument (JBI-MAStARI). 36 The studies were grouped into the following categories: cross-sectional (n = 11), pre–post (n = 2), qualitative (n = 2), cohort (n = 2), quasi-experimental (n = 1), and economic evaluations (n = 3). The majority of studies, 15 (71.4%), 39,41 –44,47 –49,51 –57 had strong methodologies and appropriate measures that met the recommended quality standards (Supplementary Table S3-S3e). Notably, the quality of the economic analysis among the three studies, 37,38,46 categorized as economic evaluations, was low. The studies failed to meet the recommended quality standards; they did not clearly report cost adjustments for differential timing, incremental analysis of costs and consequences, sensitivity analysis, or relevant costs for each alternative identified (Supplementary Table S3f).
Discussion
Our systematic review evaluated 21 studies that assessed virtual care interventions in correctional facilities and revealed several significant insights. First, no single study included in the review provided explicit definitions of the concepts of efficacy, effectiveness, and efficiency. Second, studies evaluating the effectiveness of virtual care interventions aligned best with the evaluation stage criteria outlined in the modified WHO conceptual framework. Third, the most frequently explored concept in the studies analyzed was effectiveness, followed by efficacy and efficiency, and the most common measures employed were clinical effectiveness, user satisfaction, and interexaminer agreement.
There was no common understanding of the concepts of efficacy, effectiveness, and efficiency in the included studies, and none of the studies provided a definition of the concept. Rather, the majority used measurement parameters linked to the outcomes as an implicit definition. For example, effectiveness is typically defined by measuring improvements in mental or clinical health parameters, such as sustained virological response rates for hepatitis C and HIV management, stabilization of vital signs or symptomatic relief. Roine et al. 58 also highlighted the common use of clinical terminology to define effectiveness, and that often studies that purport to measure effectiveness are, in fact, pilot studies measuring efficacy. Other studies either applied the terms interchangeably or merely referred to them in the abstract, discussion, or conclusion of the study. The varied application of these concepts is consistent with findings from other studies examining their use within the health care sector. 23,24,28,58 For instance, Burches and Burches 23 noted that these variations are unique to health research, where explicit definitions of efficacy and effectiveness are primarily applied to treatment evaluations in clinical trials. In these trials, a stage-based approach was employed, commencing with the evaluation of efficacy, which refers to the performance of a treatment in ideal conditions, followed by the evaluation of effectiveness, which gauges an intervention’s success in real-world settings. However, they pointed out that according to dictionary definitions and common usage, these three concepts remain synonymous in an everyday context. Labrique et al. 28 also noted a lack of a unifying language to guide the analyses and synthesis of virtual care interventions. This varied application underscores the importance of developing standard definitions and a guiding framework to ensure consistent and comparable assessment of virtual care interventions in correctional facilities.
Studies evaluating intervention effectiveness ranked highest in terms of conformity to relevant measurement targets associated with the evaluation stage outlined in the adapted WHO conceptual framework. For instance, all studies exploring intervention effectiveness measured changes in outcomes, and close to half measured changes in the process. Only one of the six studies evaluating efficacy adhered to the outlined measurement targets, and the one study exploring efficiency did not satisfy the criteria. Additionally, despite the distinct measurement targets for effectiveness and efficacy outlined in the WHO conceptual framework, the review findings indicated that similar measures were used to assess both the effectiveness and efficacy of an intervention. For example, user satisfaction and interexaminer agreement (reliability) are common measures explored by studies purported to evaluate effectiveness, even though these are measurement targets that are classified under efficacy. Studies that evaluated more than one concept did not permit the scoring of the framework to be performed. Of the studies explored in this review, only two explicitly identified the stage of intervention maturity as the pilot stage, even then, one of these studies explored the effectiveness of the intervention instead of its efficacy.
The WHO conceptual framework employed in this review illustrates the interrelationships between efficacy, effectiveness, and efficiency, as well as chronology, with efficacy requiring investigation during the early stages of the intervention’s maturity, followed by effectiveness and efficiency. Stage-based approaches to virtual care assessment have been proposed by other studies that emphasize the importance of a life-cycle approach to capture the varying needs that need to be accounted for at each developmental stage. 28,30,58 –60 Herbert 59 argued that a stage-based approach with distinct milestones for each evolutionary stage is necessary, as virtual care interventions often impact health care systems beyond their initial intended purpose. Roine et al. 58 highlighted this issue and acknowledged the need for studies to address not only the initial stages of virtual care interventions but also the full lifespan, system scale-up, and sustainability. Similarly, Vis and colleagues, 60 after reviewing frameworks for virtual care implementation, determined that the sector would benefit significantly by adopting phased approaches when evaluating virtual care interventions.
In correctional facilities, the effectiveness of virtual care interventions was the most frequently explored concept, whereas the least explored concept was efficiency. The measurement components used to evaluate effectiveness included clinical effectiveness, which is the most common measure, followed by user satisfaction. Other measures included interexaminer agreement, the diagnostic quality of images, pre–post intervention differences, the availability of a complete treatment, and whether radiological and medication orders were completed prior to in-person visits. Evidence on the popularity of studies on virtual care effectiveness in community and correctional facilities is mixed 58,61,62 ; for example, a review by Roine et al. 58 on the effectiveness and cost-effectiveness of virtual care in community settings revealed that most of the studies assessed the clinical effectiveness of virtual care interventions. However, the study also pointed out that the assessment of effectiveness was in fact, at times, an assessment of efficacy. Aoki and colleagues found clinical effectiveness to be the least reported measure. Even so, the growing popularity of studies on the effectiveness of virtual care is reportedly driven by the interests of stakeholders who prioritize real-world data on virtual care performance over controlled settings. This preference stems from the difficulty in conducting randomized controlled trials (RCTs) owing to the small sample size. 59,63,64 The efficacy of virtual care interventions is the second most frequently explored concept. Common measurement components used to evaluate efficacy include user satisfaction and interexaminer agreement (reliability).
Other measures assessed the achievement of health-related outcomes, such as improvement in clinical parameters, pre- and postintervention differences, diagnostic quality of pictures, access to care, and savings related to cost and in-person visits. The efficiency of virtual care interventions was the least explored concept; as a result, no common measurement components were identified in this review. Instead, efficiency was mainly measured using cost analysis, as the benefits were predominantly estimated as savings, particularly in relation to patient transfers, compared to in-person consultations. Additionally, only one study provided a cost perspective. Although research in community settings has noted a paucity of studies evaluating the efficiency of virtual care interventions, 30,58 a review focused on the correctional facilities revealed the availability of efficiency studies within this context. 6
GAPS
Overall, there is a paucity of studies focusing on women, youth, asynchronous modes of delivery, and primary health care in this setting. These studies predominantly concentrated on single medical specialties, with the majority evaluating real-time modes of virtual care delivery. A clear male sex bias and adult focus were observed when the sex and age of the study population were captured. Similar findings have been reported in related systematic reviews and ongoing studies of virtual care in correctional facilities. 5,6,65,66 Although studies have demonstrated the feasibility, effectiveness, and efficiency of asynchronous virtual care 5,37 in correctional facilities, adoption of this modality remains limited.
Future research should provide explicit definitions of efficacy, effectiveness, and efficiency to reduce variability and improve harmonization in the use of these terms and the evaluation of virtual care interventions in correctional facilities. Adoption of the WHO conceptual framework would help address this gap. Future research should also incorporate more comprehensive studies on virtual care efficiency given the significant investment in resources required for their deployment. Additionally, studies should explore the benefits of asynchronous modality for this demographic, the potential of virtual care in primary health care, and the specific virtual health care needs and obstacles faced by women and youth in custody.
This systematic review aims to enhance the clarity, shared understanding, and evaluation of three key concepts within correctional facilities. This will foster improved dialogue among health technology stakeholders and decision-makers facing public and commercial pressure to implement new virtual care initiatives in these settings. Additionally, this review provides valuable insights for custodial health stakeholders, as it not only provides a comprehensive overview of the most commonly used measures, but also offers a structured approach to evaluating the efficacy, effectiveness, and efficiency of virtual care interventions using a simplified life-cycle methodology.
LIMITATIONS
This review had several limitations. A broad and systematic search of published literature was undertaken; however, gray literature, which may have provided alternative insights into the examination of virtual care in correctional facilities, was not included. Several details were not reported in some studies, including age, sex, and ethnicity of the study population, as well as the duration of the study and the technology used. Owing to the observational nature of the included studies, nine articles utilized retrospective methods to collect data, which may have introduced misclassification bias. Additionally, not only were the studies primarily conducted in developed countries, but the small sample size may not be adequate to draw meaningful comparisons or generalizations. Non-English literature was not included in this review, which may have resulted in publication bias owing to the exclusion of potentially pertinent articles that were published in other languages.
Conclusions
The potential of virtual care to alleviate the high burden of disease experienced by highly vulnerable populations within correctional settings, particularly where face-to-face model of health care are limited is a growing area of interest in research and evaluation studies. This review offers valuable insights into the evaluation of virtual health care delivery in such settings. Foremost, the lack of standardized definitions for efficacy, effectiveness, and efficiency underscores the pressing need for an international consensus on a unifying language and framework. Establishing such standards is essential to facilitate consistent and comparable evaluation across studies. To enhance the evidence base, we advocate for the adoption of the modified stage-based conceptual framework by WHO.
Furthermore, tackling the current variability in how these key concepts are evaluated, considering the limited resources in correctional facilities, requires a paradigm shift in research priorities. Specifically, there is a need to expand the research focus from solely evaluating real-world applicability of virtual care interventions to also include more studies on virtual care efficiency within these contexts. To date, the nature of virtual care research in correctional facilities has predominantly focused on specialist synchronous health care for adult men. This emphasis underscores the need to explore new frontiers in virtual health care delivery in correctional facilities. Promising areas for further study include primary health care, store-and-forward technology, and the health needs of women and young people.
Footnotes
Acknowledgments
The authors would like to thank Jessica Birchall, Research Liaison Librarian, University of Newcastle Australia, for assistance with the development of the search strategy.
Authors’ Contributions
C.N., T.M., E.S., and M.R. conceived of and designed the study. C.N. defined the search terms and performed the initial literature search. C.N. and A.L. appraised the search, screening, full-text review, and assessment of the study quality. C.N. wrote the draft article. C.N., E.S., T.M., M.R., L.H., and X.D.G. contributed to the revision, editing, and approval of the final article.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was provided for the research.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.