
Abstract
Background:
The use of virtual care (VC) among individuals with chronic disease is well-documented, yet evidence on quality of care outcomes, such as frequency of subsequent hospitalizations, emergency department (ED) visits, and mortality, is fragmented. This systematic review aimed to synthesize evidence of quality of care outcomes, namely subsequent outpatient encounters, hospital admissions, ED visits, and mortality, associated with VC among outpatients with chronic diseases.
Methods
: A search strategy was developed and applied to six electronic databases (Embase, MEDLINE, the Cochrane Library, PsycINFO, Web of Science, and CINAHL) for articles published between January 1, 2013 and July 6, 2024. Eligible studies included synchronous VC (e.g., live, video, or audio based) between a patient and health care provider. A narrative synthesis compared VC with in-person care, considering types of outpatient care, specialty, VC components, follow-up duration, and outcomes.
Results
: After reviewing 5,679 abstracts, 24 articles were included. Studies were predominantly from the United States (n = 11), followed by Australia (n = 3) and Canada (n = 2). The follow-up durations ranged from 2 weeks to 2 years, with 14 studies having follow-up durations of 6 months or less. Studies predominantly reported no difference or lower rates of hospital admissions (n = 18/20), ED visits (n = 11/12), and mortality (n = 12/14) among outpatients who used VC compared with those who had in-person visits. Half of the studies (n = 3/6) reported more subsequent outpatient encounters for patients using VC for the initial outpatient encounter compared with those who had in-person visits.
Conclusion
: The review indicated that outpatient VC is associated with fewer or no different volume of hospital admissions or ED visits among people with chronic conditions but may be associated with an increased number of outpatient follow-up visits. Robust research at scale that considers the volume of VC consumed and associations with outcomes over longer follow-up periods is required.
Background
Virtual care (VC) is broadly defined as “a health care activity supported at a distance by information and communication technology service(s).” 1 VC encompasses consultations conducted via telehealth (namely, telephone and videoconferencing) or remote monitoring supported by digital patient information, mobile phone applications, patient portals, or wearable devices. 2 VC has existed for several decades and has been tested in a variety of health care settings but rarely as part of a system-level approach. 3 The COVID-19 pandemic created an urgent need to rapidly expand VC across all health care settings (inpatient and outpatient). This widespread use demonstrated the potential opportunities of VC for systematic notable gains in the efficiency of health service delivery, improving equity of access to care across diverse outpatient settings and specialties. 4 –7
VC is now widely adopted in outpatient settings by clinicians and patients across urban, regional, and rural contexts to treat and manage a range of health conditions, particularly chronic disease management. 8,9 VC has recently become an integral component of health care systems. Since, despite the challenges, such as the lack of physical examinations, international studies indicate strong satisfaction including the ability to treat patients and efficient processes among health care providers and cost savings and convenience, with lower clinic wait times and cancellation rates among patients. 10 –13 As a consequence, VC is now being used for preliminary assessments, routine checkups, monitoring, and follow-up care in outpatient settings, especially among patients with chronic diseases. 14,15
In the post-COVID-19 era, outpatient hospital clinics are continuing to adjust to the integration of virtual and in-person care to deliver optimal care quality outcomes. 16 Health administrators and health care providers are uncertain about the impact of VC on the quality of care among outpatients. For outpatient care, key indicators of the quality of care can include subsequent unplanned outpatient visits, unplanned hospitalizations, hospital length of stay (LOS), emergency department (ED) visits, and mortality. 17 Current evidence on quality of care outcomes for outpatient virtual encounters has only focused on specific conditions (e.g., kidney disease) and/or a particular type of outpatient care (e.g., postoperative care and regular checkups). 15,18 –24 Other studies have also sought to determine patient preferences and acceptability of using VC following the acute pandemic period. 23,24 Some investigators suggest that VC results in no difference or even improved quality of care outcomes, with reduced hospital admissions, LOS, and ED visits compared with traditional in-person visits. 18,25 However, others have indicated suboptimal quality of care outcomes. 15 These mixed findings highlight the need for a review of the effectiveness of VC across multiple chronic diseases in outpatient care settings. There has only been one scoping review conducted among adults with kidney disease that considered quality of care outcomes for outpatients receiving video-based telemedicine versus in-person care, which indicated comparable quality of care outcomes (i.e., the number of hospital admissions, LOS, ED visits, and mortality). 4 However, the review has reported the outcomes of VC in the context of a single patient cohort, e.g., those with kidney disease spanning multiple care settings, including inpatient and primary care settings. While this approach enabled a rich understanding of the patterns of VC engagement for a given chronic condition, no reviews have provided an analysis of quality of care outcomes associated with VC use across multiple outpatient chronic disease services.
A synthesis of evidence on quality of care outcomes associated with VC use across multiple outpatient settings is required to inform health system investment and planning for the incorporation of VC in outpatient models of care and to inform the health services research agenda on VC. 8 This systematic review aims to synthesize contemporary evidence of the quality of care outcomes (namely, subsequent outpatient visits, hospitalization, ED visits, and mortality) associated with VC consultations compared with in-person care in outpatient settings among patients with chronic disease.
Methods
SYSTEMATIC REVIEW PLANNING AND REGISTRATION
This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA). 26 The review protocol was registered on the Prospective Register of Systematic Reviews (CRD 42023430527).
INCLUSION CRITERIA
Studies were eligible for inclusion that: Had reported VC as utilizing synchronous interactions telecommunication technologies. VC modalities consisted of telehealth (i.e., telephone and video conferencing) and apps (e.g., WhatsApp, Zoom, and health service-specific apps), functioning as a substitute for conventional in-person interactions between clinical health care providers and patients.
27
Were conducted predominantly among adults (age ≥ 18 years). Were conducted in settings with any health care consultation, procedure, or treatment administered through hospital-based services with a hospital stay of 23 h or less—as per the Australian Institute of Health and Welfare (AIHW) definition for hospital admissions.
28
Included outpatients with chronic disease, defined according to the World Health Organization definition: “Chronic diseases are long-lasting conditions, non-communicable diseases, with persistent effects.”
29
This definition aligns with chronic diseases and conditions identified by the Centers for Disease Control and Prevention (CDC), which is also consistent with the classification used by AIHW.
30
Were primary research. Were available in English. Reported at least one of the quality of care outcomes specified by the Australian Commission on Safety and Quality in Health Care
31
(namely, hospital admissions, ED visits, subsequent outpatient care, and mortality) for patients with at least one chronic disease after their outpatient encounter.
EXCLUSION CRITERIA
Since the objective of this study is to report the quality of care outcomes in outpatient settings among those who used VC versus those who did not, noncomparative studies were excluded.
Studies that did not report quality of care outcomes related to chronic disease patients were not included.
Conference abstracts, case studies, editorials, opinions, comments or commentaries, systematic reviews, and protocols were excluded.
DATA SOURCES AND SEARCH STRATEGY
A search strategy was developed by a medical information specialist, using the key concepts of telehealth in outpatient settings and quality of care outcomes by developing keywords, synonyms, and phrases. The search strategy was applied to use six electronic databases: Embase, MEDLINE, the Cochrane Library, PsycINFO, CINAHL, and Web of Science, from January 1, 2013 to July 6, 2024. Snowballing techniques to improve search sensitivity, such as reference list reviews and searching the contents of relevant journals, were applied to locate additional relevant studies.
SELECTION PROCESS
Relevant studies were exported to reference management software (Endnote 20.2.1), via which duplicates were removed. Covidence systematic review software 32 was used for study screening. Title and abstract screening were conducted independently by six authors (M.S., R.W., E.M., R.M., M.M., and V.M.) in Covidence 32 using the eligibility criteria. Nine reviewers, M.S., M.M., R.C.W., R.H., R.W., E.M., V.M., R.M., and B.C., independently conducted full-text screening of the remaining studies. The core review team (M.S., R.W., R.M., and R.H.) resolved disputes to make a final determination. M.S. conducted data extraction, and the extracted data were reviewed and verified by two senior authors (R.M. and R.H.).
EVIDENCE SYNTHESIS
Data extraction and synthesis were conducted in stages. The following details were extracted for each study in the data extraction table: authors, aims, country, study timeframe, study design, patient cohort, sample size and age, geographical location, type of outpatient care, type of outpatient visit, duration of follow-up, quality of care outcomes, and study findings. Research team members (M.S., R.H., and R.M.) discussed key findings relating to the primary outcomes and VC modalities to identify patterns in the data and consistent and divergent findings. The findings were examined in relation to the study design and setting to develop a rich picture of the findings in context. The study findings were reported based on the quality of care outcomes.
RISK OF ASSESSMENT BIAS
An assessment of potential bias was conducted within a wider assessment of the methodological quality of the included studies using the critical appraisal tools for use in the Joanna Briggs Institute appraisal tool. 33 A specific appraisal checklist was used based on the study design of the included studies. The tools contain a checklist of questions with “Yes,” “No,” “Unclear,” and “Not applicable” responses.
Results
STUDY SELECTION
The study selection process is shown in Fig. 1. The database searches returned 5,679 studies. After removing duplicates (n = 206), the titles and abstracts of the remaining 5,473 studies were screened, and 5,118 were excluded at this stage. From the remaining 355 studies and after full-text screening, 24 studies were included in the review.
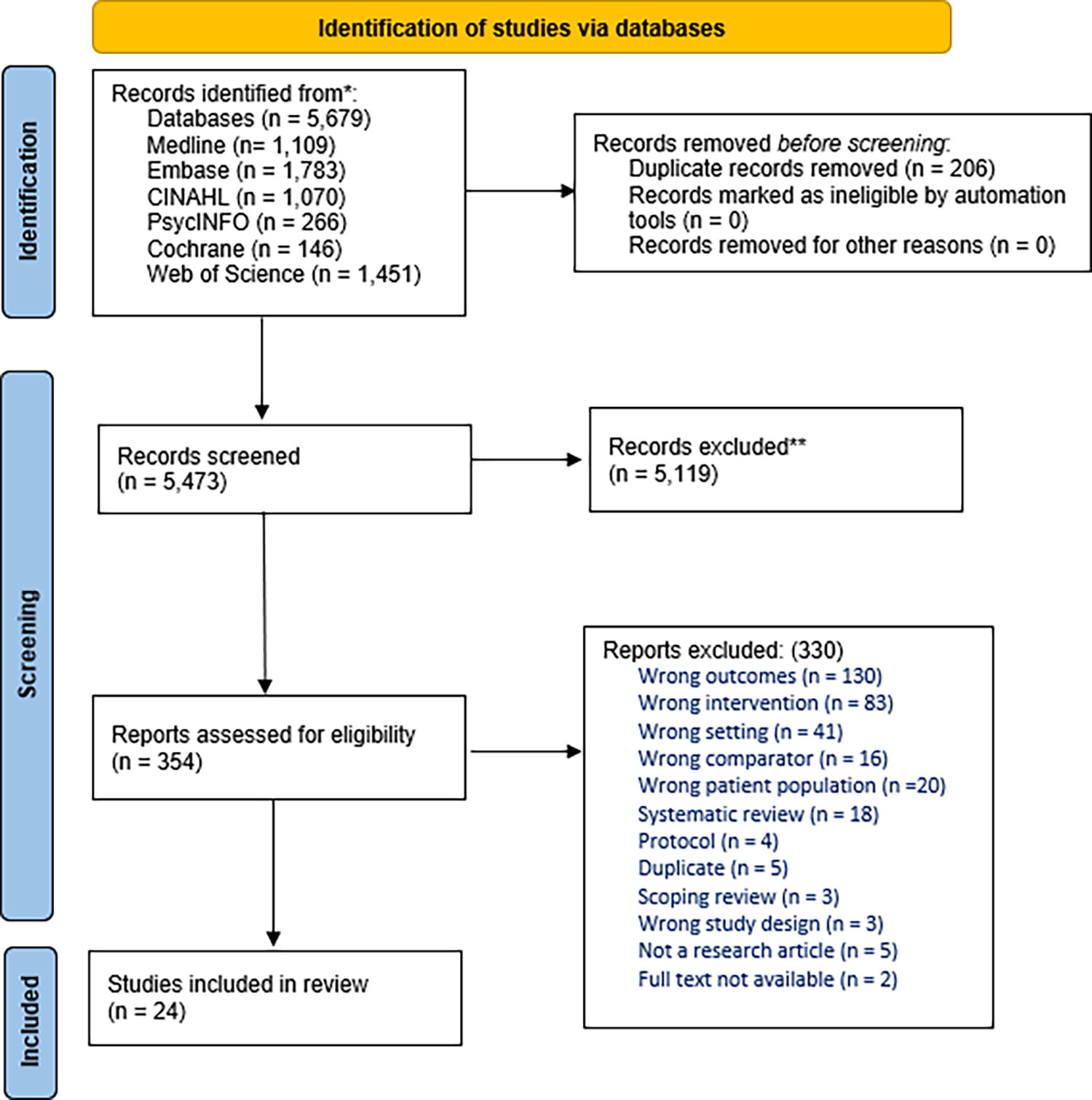
PRISMA 2020 flow diagram included searches of databases, registers, and other sources. *Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers). **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021:372:n71. doi: 10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/. PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis.
CHARACTERISTICS OF THE INCLUDED STUDIES
Almost half of the included studies (n = 11) were conducted in the United States. 6,13 –15,19,20,34 –48 The remaining studies were conducted in Australia (n = 3), 49 –51 Canada (n = 2), 18,52 and one study each from China, 53 Germany, 21 Denmark, 54 Norway, 55 Finland, 56 Poland, 57 Spain, 58 and Japan. 59 Over half of the studies (n = 16) were cohort studies. 15,18,19,36,42,45 –47,50,52,58,60 –62 The remaining studies were randomized controlled trials (RCTs) (n = 7) 20,42,54,55,57 and case–control studies (n = 1). 50
Over half of the studies (n = 14) had follow-up durations of 6 months or less from the outpatient encounter; of these, 10 studies had follow-up periods of 3 months or less. The types of outpatient care were regular checkups (n = 7) and follow-up care after hospitalization or operations (n = 7). Several studies were not specific on the type of outpatient care (n = 10). Hospitalization was the most frequently reported quality of care outcome (n = 18), followed by ED visits (n = 12), mortality (n = 12), and subsequent outpatient visits (n = 6).
Study participants were predominantly aged 50 years and older (n = 15). 6,13 –15,18 –20,36,41,42,44 –47,49 –51,53,55,57,62 –66 Almost one-third of the studies (n = 10) included a subsample of nonmetropolitan patients. 14,15,18,37,43,46,51,52,55,63,64 The sample sizes of cases (VC group) and the comparator groups varied substantially between studies, ranging from 16 to 2,807,604 participants in the VC groups and 25 to 2,684,694 participants in the comparator groups (Table 1).
Characteristics and Quality of Care Outcomes of the Included Studies
*ED, emergency department; HF, heart failure; IQR, interquartile range; RCT, randomized controlled trial; RR, relative risk; SD, standard deviation; VC, virtual care.
The majority (n = 22) of VC modalities were telehealth, comprising telephone or video consults. Almost half of the telehealth modalities were via telephone (n = 10), of which several offered video as an alternative (n = 7), and two involved sending images via emails or an application. 22,42,53 A number of studies (n = 13) included only video consultations; the remaining two studies used web-based communication systems. 46,57
A range of chronic condition cohorts were represented, with adults with a cardiac-related condition most highly represented (n = 7), followed by cancer (n = 4), mental health (n = 4), diabetes (n = 3), kidney disease (n = 3), pulmonary disease (n = 1), rehabilitation (n = 1), and obesity (n = 1). 15,18,19,36,50,52,54,57,59 –62
Over half of the studies (n = 14) compared telehealth during the acute COVID-19 period (from January 2020 until July 2021) 67 with in-person visits that occurred before the onset of COVID-19 (n = 13) or after (n = 2) the acute pandemic period. From the remaining 10 studies, the majority (n = 7) included both types of encounters (VC and in-person) before the onset of COVID-19 (before January 2020). One study assessed telehealth compared with in-person care entirely postpandemic (April 2021 to February 2022; Fig. 2).
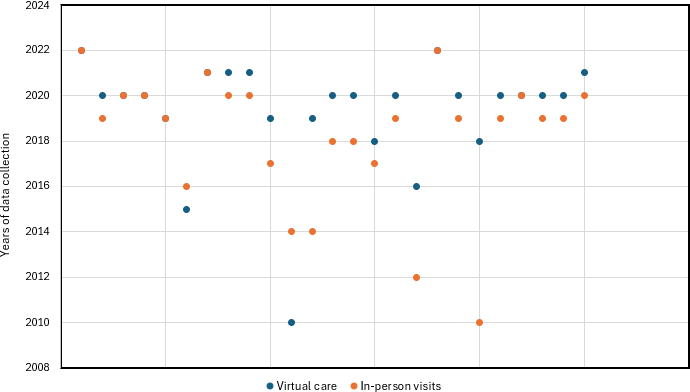
Years of data collection of the included studies.
STUDY QUALITY
Supplementary Tables S1 and S2 provide the findings of the quality appraisal for each of the studies. Overall, studies were considered relatively good quality (>70% “yes” responses to the quality appraisal criteria). Strong features were having appropriate exposure and outcome measurements, sound study design, and sufficient follow-up duration. In several studies, confounding factors were not incorporated into the analysis, and the types of analyses were also considered inappropriate for the study designs as comparisons of quality of care outcomes between VC and in-person groups were only conducted using univariate analyses. Some studies had a small sample size. 21,42,45,55
QUALITY OF CARE OUTCOMES
Of the 24 studies reviewed, the majority (n = 19) reported two or more eligible outcomes. The majority included subsequent hospital admissions (n = 20) followed by mortality (n = 14), ED visits (n = 12), and subsequent outpatient encounters (n = 6).
The results of the studies with multiple types of quality of care outcomes were generally consistent for hospital admissions and ED visits. 15,52 For instance, a study by McAlister et al. 52 suggested lower odds of 30- and 90-day hospital admissions and ED visits but higher odds of mortality at both the 30-day and 90-day follow-up for outpatients with telehealth compared with those who had in-person visits. This study was conducted among adults with cardiovascular conditions who had video or telephone consultations compared with those who had in-person visits. Similarly, three studies that evaluated ED visits, hospital admissions, and subsequent outpatient encounters 46,49,68 reported comparable trends: lower rates of hospital admissions and ED visits but higher numbers of subsequent outpatient encounters in the telehealth groups than in in-person groups.
The only pattern observed between the outcomes and participants’ demographic and clinical characteristics (such as age, geographic location, and telehealth modality) was seen among older individuals in studies where telephone consultations were the primary form of consultations, and using other virtual devices was optional. 49,52 Those studies reported a higher mortality rate and subsequent outpatient encounters among outpatients who had telehealth encounters. No other patterns were identified between the outcomes and participants’ demographics, the severity of their chronic conditions, follow-up periods, or the timing of data collection relative to the pandemic. Similarly, no patterns were identified by the modality of VC encounters (telephone vs. video vs. web-based system) and the quality of care outcomes.
SUBSEQUENT OUTPATIENT ENCOUNTERS
A total of six studies reported the difference in the number of subsequent outpatient encounters between outpatients who had the initial encounters virtually compared with those who had in-person visits. 46,47,53,55,61,68 Video was the primary type of VC in almost all the studies (n = 5). In the remaining study, telehealth modality was solely telephone, with the results indicating no difference in the number of subsequent outpatient encounters. 68 Three studies reported a higher number of subsequent outpatient encounters among the VC group, two of which were conducted in mental health settings 46,68 and one among patients with diabetes. 49 Notably, in all three studies, telehealth users were predominantly older adults who used the telephone during COVID-19 and were compared with those who had in-person visits outside of COVID lockdowns. 46,49,68
Three studies, which reported lower or no difference in the number of subsequent outpatient encounters in telehealth groups, were conducted in cancer, diabetes, and peritoneal dialysis. 47,53,55 Of these, one study compared both telehealth and in-person groups during the pandemic in 2020, and two studies compared outcomes for both groups prepandemic. 47,53,55
ED VISITS
Of the 12 studies, 11 indicated fewer (n = 8) 13,18,19,42,47,58,61,62 or no difference (n = 3) 21,36,52 in the proportions of ED visits after telehealth encounters compared with in-person visits. Of the 12 studies, in half of the studies (n = 6), telehealth encounters were conducted via video, with the remainder having video as an optional mode.
In the sole study that reported a higher proportion of ED visits, the telehealth group tended to be younger (mean age = 59) and had the encounter during the pandemic period (2020), as opposed to the comparison group who were slightly older (mean age = 62) and had in-person visits before the pandemic (2019). 15
SUBSEQUENT HOSPITAL ADMISSIONS
Of 20 studies, almost all indicated no difference (n = 10) or fewer (n = 8) admissions in the telehealth groups. 18,42,50 –52,58,62 These studies were among patients accessing mental health (n = 4), cardiology (n = 3), rehabilitation (n = 2), cancer (n = 3), pulmonary (n = 1), diabetes (n = 1), and obesity (n = 1) care. 13,18,19,45,46,52,53,57,62 The two studies that reported the higher proportions of hospital admissions were both in cardiology settings, one of which had video consultation as an option to the telephone, and another had video as the main component of VC. 15,60 In the studies that reported no difference or fewer hospital admissions between the telehealth and in-person groups, video was the predominant modality of telehealth encounters (n = 7). 15,22,47,49,65 Several studies had video as an option for contacting their health care provider (n = 6). 15,18,52 Only one study was restricted to telephone, one had a monitoring system in addition to the telephone, 62 and one had a web-based service as a means of communication. 53
MORTALITY
Among all studies (n = 14) that reported mortality as an outcome, the majority (n = 13) found no difference (n = 9) or lower proportions of mortality (n = 4) for outpatients who had VC compared with adults who had in-person visits. 6,14,15,18,36,50,51,55,57,66 The type of telehealth used was the telephone, among the studies that reported higher mortality risk. 52,54 In one of these studies, adults with a record of mortality were older (≥70 years) and had advanced chronic diseases (such as chronic heart disease, chronic kidney disease, and cancer) plus other conditions, including sepsis, pneumonia, and gangrene. 54 Though, in that study, age and number of comorbidities were adjusted for as confounding factors, the author 54 indicates that the difference in severity of comorbidities among those who had mortality in the telehealth group may not have been controlled by adjusting the statistical models.
Discussion
The results of this systematic review synthesizing 24 studies indicated that patients who used VC predominantly had no difference or fewer numbers of hospital admissions, ED visits, and mortality compared with patients who had in-person visits in outpatient settings across a range of chronic diseases. To our knowledge, this is the most recent and first literature synthesis on quality of care outcomes between virtual and in-person care, including studies across multiple chronic diseases in outpatient settings.
As technology continues to advance and integrate into health care systems, it is increasingly important for health systems to identify areas where VC can not only sustain but also enhance the quality of care outcomes. 69 National data from Canada and Australia show that over half of patients prefer VC as a primary point of contact with their health care providers, 70 a trend that aligns with the potential opportunities for VC use reported in this review. However, these benefits should be considered alongside the disparities in access to telehealth and VC in a broader concept, which are influenced by social determinants of health and the “digital divide.” Addressing these challenges will require ongoing scrutiny to ensure equitable access and outcomes.
As the results showed, more outpatient encounters after the initial VC encounter were observed in studies where the participants were from older age groups. All three studies compared outpatient visits during the COVID-19 lockdown to prepandemic in-person visits, with telephone consultations and supplementary devices (e.g., video and image sharing) as alternatives. The higher number of outpatient encounters may stem from older adults’ difficulty transitioning to VC during the pandemic, as they struggled with tasks like logging in, uploading images, and troubleshooting technical issues. 71 As a result, they primarily used the telephone, which lacks nonverbal cues and can be challenging for both patients and providers, leading to increased outpatient encounters. 72 Previous studies have also found that older outpatients using VC tended to have more outpatient encounters than younger groups. 73,74 However, as this review showed, the higher number of outpatient encounters did not worsen other quality of care outcomes.
Beyond the factors discussed above, notably, data collection pre-, during, and post-COVID-19 pandemic is a critical factor to consider in interpreting these findings. Over half of the included studies (n = 15) reported outcomes collected during the pandemic, a period marked by complexity in routine preventive care and uncertainty about the health care capacity, which could have influenced ED visits and unplanned hospital admissions. 75 –77 This may have created hypervigilance in monitoring for symptoms and health concerns, promoting greater health service use. This may have shaped the findings somewhat, although the results on all the included outcomes, except for outpatient encounters, remained consistent across studies conducted before, during, and after the pandemic. As the health system moves beyond the pandemic, emerging research to provide further insight into the relationship between VC and subsequent health care use is required.
The results of this systematic review are consistent with the only existing systematic review, focusing solely on kidney diseases, showing no difference or even a lower number of subsequent hospital admissions, mortality, and ED visits among patients who had outpatient VC versus in-person care. 4 The findings of this review should be encouraging, considering the benefits of VC on subsequent quality of care outcomes (smaller number of subsequent hospital admissions, ED visits, and outpatient encounters and mortality).
Strengths and Limitations
Synthesizing the results of the included studies showed that establishing the quality of care outcomes associated with telehealth consultations is challenging. This is due to the heterogeneous component of VC as well as the diversity in models of care in which VC and in-person visits have been integrated. One of the strengths of this review was the process of the systematic search strategy developed in consultation with a medical information specialist, involving multiple data sources with reporting using the PRISMA guidelines. The findings of this review do, however, require consideration in light of the limitations of the included studies. Most of the included observational studies and RCTs were often limited to short follow-up durations, which could inhibit understanding of the true association between the VC and subsequent outcomes, such as mortality in the long term. 6,20,42 Furthermore, as the quality appraisal showed, almost all the studies with longer follow-up times (i.e., ≥1 year) did not have any strategies (such as using an appropriate statistical analysis) to account for the follow-up time or loss of follow-up, which could recall for a risk bias. 78 Lastly, many studies did not incorporate important confounding factors, such as age, distance from the clinic, and severity of the condition, in their analyses, resulting in overestimating the reported point estimates.
Implications
The results of this review indicated that most studies reporting increased outpatient encounters after the initial outpatient telehealth consults primarily included older adults with multiple chronic conditions. Older patients often require health care across several health sectors, such as primary and acute care and aged care. Providing such care requires innovative solutions, technology, and new models of care to successfully respond to this integration. 79 Since older patients are more likely to have multiple complex chronic diseases, they tend to have poorer quality of care outcomes (e.g., higher risk of mortality and/or higher numbers of hospital admissions). 15 Therefore, a hybrid model of care that enables clinicians to have hands-on assessments is an optimal option for this population group.
Furthermore, due to the limited information available on the impact of the type of telemedicine modality on the quality of care outcomes, this systematic review is unable to identify potential patterns between these aspects. Nonetheless, results of a recent systematic review indicated that video consultations are either superior or on par with telephone consultations for outpatients with chronic disease. 80 Compared with telephone consultations, video consultations showed better patient engagement and retention, improved transfer decisions, and reduced the use of downstream subacute care. 80 Their results also suggest that the effect of telemedicine modality on consultation time, completion rates, failure-to-attend rates, and acute care utilization is inconclusive. Despite having a higher incremental cost, video consultations are generally more cost-effective than telephone consultations. 80 Future research should address the variations in quality of care outcomes and costs across different telemedicine modalities.
Results of this study indicated that the change from in-person to VC over the pre-, during, and post-COVID-19 periods, VC did not lead to higher numbers of hospital admissions, ED visits, and mortality. This is encouraging, while policymakers need to understand whether VC is providing needed services that were not previously being delivered, replacing similarly effective in-person services. As we transition from the pandemic, the emerging body of literature increasingly focuses on the role of digital health in health care delivery. The findings of this review provide important evidence supporting the use of telehealth in outpatient settings for chronic disease management among adults, which can guide policymakers and decision-makers in developing strategies for effectively integrating telehealth into routine care.
Recommendations for Future Research
Further studies with longer follow-up periods in which the modality of outpatient care and patterns of use of VC versus in-person visits are considered would provide valuable insight into the impact of VC on long-term outcomes, including mortality. Additional studies to assess VC and quality of care outcomes among outpatients across a range of settings pre, during, and postpandemic are required to provide further insight into the scale of the longer-term use of VC in outpatient settings and associated outcomes. The Smarter Hospitals Project 81 provides one such analysis that may advance the understanding of the quality of care outcomes associated with VC use among outpatients accessing cancer, renal, mental health, and rehabilitation services. The results of such studies will enable the health care system to allocate appropriate types of VC in outpatient settings.
In addition, the flexibility and convenience of VC present significant opportunities for further research into its application across various chronic disease environments, such as cancer, mental health, rehabilitation, and kidney disease. While existing literature provides strong evidence for the effectiveness of VC in areas such as cardiology, diabetes, and mental health, there remains a gap in research concerning specialties such as oncology, rehabilitation, and nephrology, which warrant further exploration.
Finally, future studies that examine factors such as frequency and patterns/volume of contact within hybrid care models and their impact on quality of care outcomes could be beneficial. The results of such studies inform the health system to potentially define benchmarks for a “safe” number and patterns of VC interactions among outpatients with chronic diseases. Emerging programs 82 of work are progressively looking at the data across major health areas, e.g., renal, cancer, rehabilitation, and mental health, with long-term follow-up. The findings from these studies could guide health services in making informed decisions about the optimal volume and point of care for integrating VC, ensuring safety and effectiveness.
Conclusions
The results of this review indicated that the current literature predominantly suggests no significant difference and even smaller numbers of hospital admissions, ED visits, and mortality after having a VC encounter compared with in-person visits in outpatient settings. As technology continues to advance, and as patients report positive experiences with VC, its benefits to patients and health care providers are likely to become evident over time. Moving forward, continuing research will be essential in shaping a sustainable and adaptable VC model that meets the evolving needs of health care systems and patients. As health care settings become increasingly flexible and amenable to virtual integration, a long-term strategy for VC’s role in chronic disease management is becoming increasingly clear.
Footnotes
Author Disclosure Statement
No interests to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.