
Abstract
A 53-year-old woman presented with an enlarging mass in the medial aspect of her right thigh. Magnetic resonance imaging suggested an intramuscular hydatid cyst. The cyst was surgically excised. Although muscular hydatidinosis is rare, its resemblance to soft tissue tumors warrants careful diagnosis since any invasive diagnostic measures may lead to fatal complications.
Introduction
Case Report
A 53-year-old woman presented with a 4-month history of a painless, progressively enlarging mass in the medial aspect of her right thigh. She had no history of trauma, fever, or chills. On physical examination, a 15 × 15 cm mobile, nontender mass with soft tissue consistency was palpated on the medial aspect of her right thigh. There was no erythema, heat production, edema, ecchymosis, or hyperemia on the overlying skin. No regional lymphadenopathy was noted. She had a normal range of motion of her right hip and palpable symmetrical pulses of her lower extremities. The remainder of the physical examination was unremarkable. Complete blood counts and serum electrolyte values were all within normal limits. Magnetic resonance imaging (MRI) of the right femur and hip demonstrated multicystic changes within a well-defined mass occupying the medial aspect of the right femur (Fig. 1A, 1B). The diagnosis of a solitary hydatid cyst within the right adductor brevis muscle was entertained. Since Hydatid disease was high on the differential diagnosis, fine-needle aspiration was not performed. Indirect hemagglutination test revealed a titer level of <1:16, which was negative as per our laboratory value.
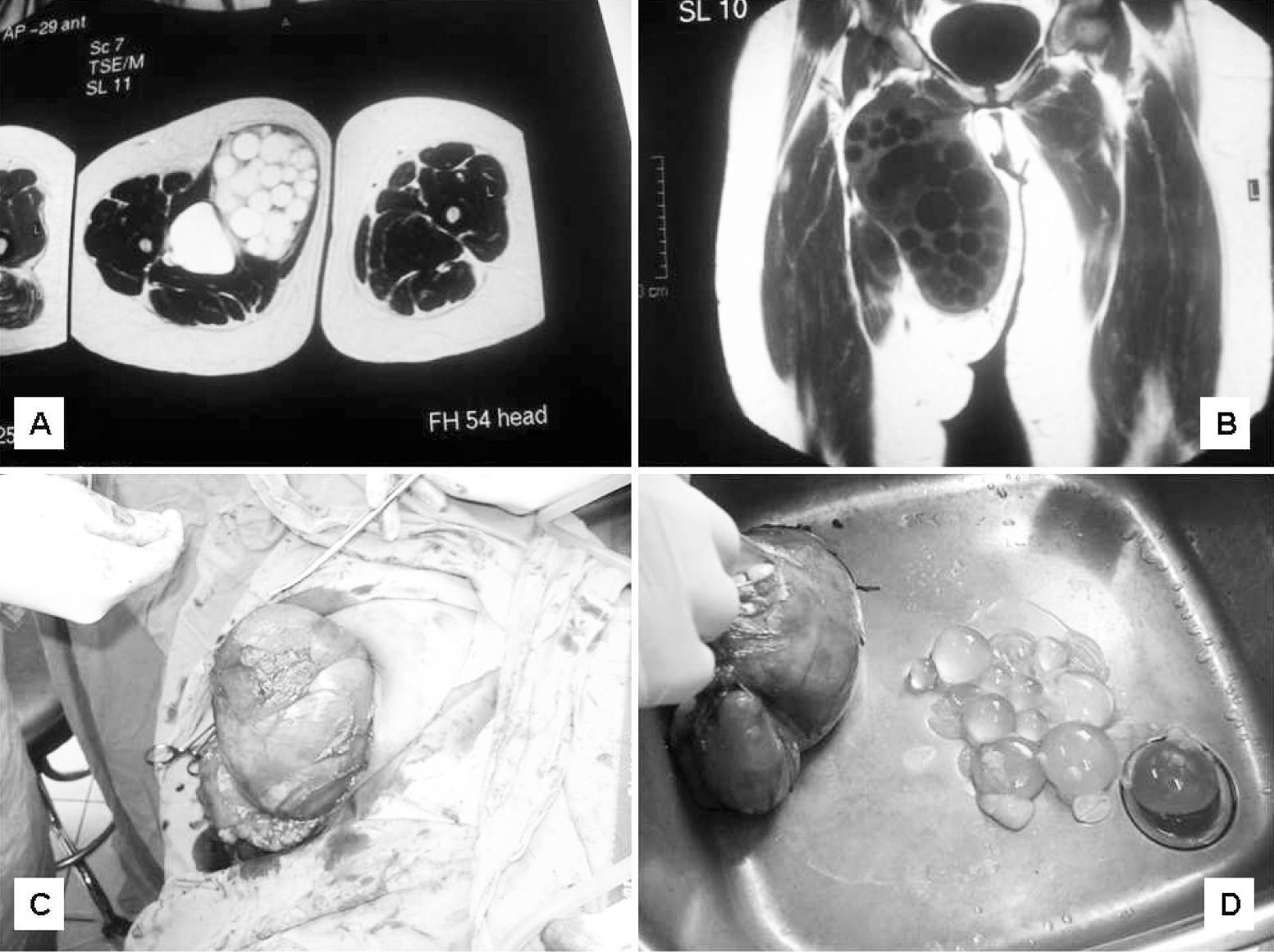
The patient was then taken to the operating room and a vertical incision was made down the right medial aspect of the thigh to reach the lesion. Cetramide was used as a scolicidal agent to irrigate around the cystic cavity. Subsequently, complete excision of the large cyst was performed with careful attention to avoid rupture and spillage (Fig. 1C, 1D). Pathologic evaluation of the excised cyst confirmed a 130 g intramuscular mass in the medial thigh, measuring 22 × 19 × 6.5 cm with a fibrolamellar chitinous membrane accompanying pericystic resorptive inflammation. The patient was maintained on albendazole at a dose of 400 mg twice a day for a period of 6 weeks.
Discussion
Echinococcus granulosus is present in nearly all countries of the Middle East region, while Echinococcus multilocularis infection is limited to a few countries (Battelli et al. 2002). In the Middle East and North Africa, the reported incidence ranges between 2 to 4 cases per 100,000. Highest rates of human infection are recorded in cattle-, camel-, and in sheep-rearing countries (Eckert et al. 2001).
Voluntary muscles are rarely affected in human hosts, for it is believed that parasite survival in musculoskeletal tissues is unfavorable due to the presence of lactic acid and muscular contractions preventing fixation of larvae to the muscular tissue. However, proximal muscles of the lower limbs might be involved due to the volume occupied by muscle mass and its rich blood supply (Durakbasa et al. 2007). To our knowledge, our report is the first in the literature that describes hydatid cyst involvement of the adductor brevis muscle and the fifth report to describe involvement of the thigh (Durakbasa et al. 2007, Orhan et al. 2003, Kocakusak et al. 2004, Ozkoc et al. 2003) (Table 1).
IHT, indirect hemagglutination test; US, ultrasound; CT, computerize tomography scan; MRI, magnetic resonance imaging.
Hydatid cysts resemble soft tissue tumors in their presentation in the thigh region; therefore, their diagnosis has to be ruled out, both clinically and radiologically, prior to any invasive diagnostic intervention. Fine-needle aspiration of the cyst might lead to dissemination and anaphylactic shock. This observation is further recommended in regions where Echinococcus is highly prevalent. As radiologic imaging should precede any biopsy or surgical intervention, they may aid in defining the suspicion. Ultrasonography is a useful first diagnostic tool for the detection of hydatid disease of soft tissue, through evidence of a multicystic mass; it has a sensitivity of 95% that increases to 100% in the presence of vesicular fibrils (Comert 2003). However, MRI remains the best modality for identification of intramuscular hydatid cysts, differentiating it from other soft tissue tumors by the detection of daughter cysts and multivesicular lesions with hypointense peripheral rings (rim sign) and serpiginous septate-like pericysts (water-lily sign) (Comert 2003). Serologic tests, namely indirect hemagglutination assays, are also helpful and can be used to complement the diagnosis. The various serologic tests have a 64% to 87% sensitivity rate and a false-negative is seen in half of the primary intramuscular hydatidosis cases. Nevertheless, negative serology does not exclude the diagnosis. In addition, Casoni skin test can also be utilized but has a low specificity and a 40% false-positive rate possibly due to encapsulation of the lesion (Orhan et al. 2003).
Treatment is best achieved by complete excision of the intact cyst following irrigation using cetramide, hypertonic saline, or hydrogen peroxide. It is imperative to avoid any rupture or spillage of its contents intraoperatively due to the increased likelihood of anaphylactic shock and hydatidinosis causing recurrent infestations. Postoperatively, reaginic immunoglobulin E antibody titers start to decrease, and recurrence of hydatid disease should be considered if still positive after 2 years (Orhan et al. 2003).It has been suggested that preoperative and postoperative treatment with imidazole compounds, such as albendazole and mebendazole, is beneficial in minimizing recurrence and permitting safer management of the cyst during surgery. Complete cure can be achieved pharmacologically in as many as one-third of the patients. A decrease in the cyst size has been observed in 40% to 70% of patients with the administration of albendazole (10 mg/kg/d for 4 weeks with 14-day intervals) or mebendazole (40–50 mg/kg/d continuously).
In summary, echinococcus should be included in the differential diagnosis of cystic masses of soft tissues, especially in endemic areas. Differentiation from a soft tissue tumor is paramount in order to avoid fine-needle aspiration with subsequent complications. Adequate clinical and radiologic workup will lead to confirmation of the diagnosis and appropriate preoperative, operative, and postoperative intervention with a favorable outcome.
Footnotes
Disclosure Statement
No competing financial interests exist.