
Abstract
From September through October 2006, an unknown disease characterized by acute onset of fever, joint pain with or without swelling, and maculopapular rash along with fatigue was reported from three villages of Cuttack and one village of Kendrapara district of Orissa, India, by the State Health Department. Upon learning this, a team from Regional Medical Research Centre (Indian Council of Medical Research), Bhubaneswar, Orissa, conducted an epidemiological investigation in the area. Household survey was carried out and clinical examination of the symptomatic individuals (n = 1289: Kendrapara, 752; Cuttack, 537) undertaken. Based on the recorded chikungunya (CHIK) fever symptoms, a vector-borne viral disease was considered for provisional diagnosis. Blood samples were collected from 217 symptomatic individuals; to confirm the diagnosis, sera were tested for anti-CHIK antibody (immunoglobulin M), which revealed 63% (64/101) and 40% (47/116) seropositivity in the samples from Kendrapara and Cuttack district, respectively. The illness was managed with analgesics like paracetamol. No death was recorded due to the illness. Entomological survey in the areas revealed the presence of Aedes mosquitoes: aegypti, albopictus, and vittatus. The per-man-hour density of Aedes vectors ranged from 0.8 to 7.6. High larval indices, house index >17% and Breteau index >70%, also indicated Aedes breeding in the area. The investigation documented circulation of CHIK in Orissa, India, and helped to take preventive steps in the outbreak area, with the suggested vector control measures.
Introduction
The country then experienced several outbreaks during 2005 and 2006. The total number of cases reported till the end of 2006 was above 1.3 million (CDC Report 2007–2008). Different states and union territories reported to have CHIK cases have been shown in Figure 1. Andhra Pradesh was the first state to report CHIK cases in the country. Beginning with 3 districts in the month of December 2005, 23 districts were affected in this state with a total case report of 77,535 and 20% seropositivity (CDC Report 2007–2008, Chhabra et al. 2008). The number of cases from Maharastra was 34,725 until April 2006, affecting four districts, and that from seven districts of Karnataka was 18,529 during December 2005 to August 2006 (Chhabra et al. 2008). The number of cases from Gujarat was more than 70,000 from July to October 2006 (Mavalankar et al. 2007a). The number of CHIK cases recorded from Tamil Nadu, Madhya Pradesh, and Kerala states in the same year was 64,802, 60,132, and 70,731, respectively. During 2007 and 2008, 59,535 and 1222 CHIK cases were reported from 14 and 3 states, respectively (CDC Report 2007–2008).
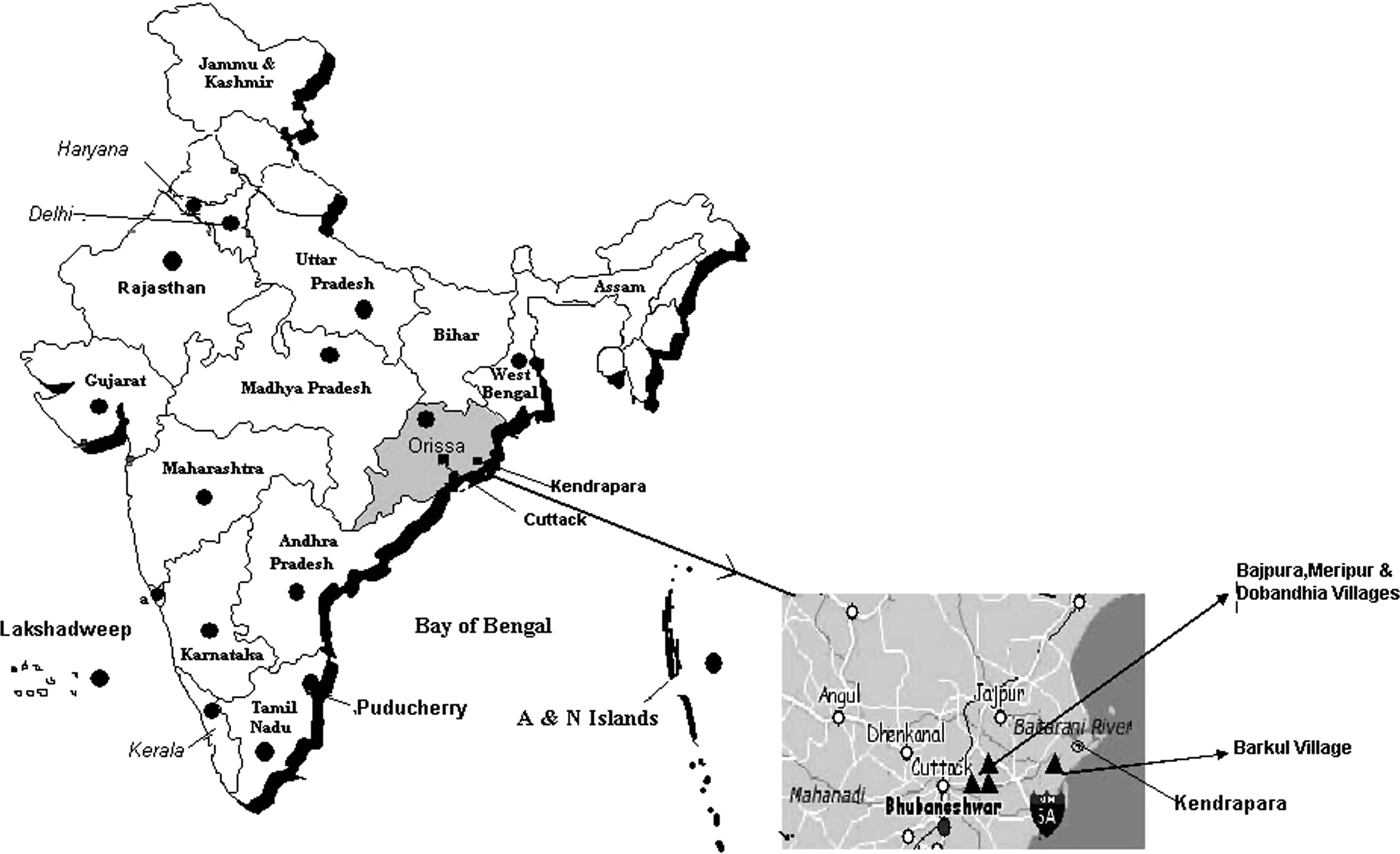
Map of India showing the states and union territories reported of chikungunya outbreak (2005–2008) and the studied outbreak area of Orissa state (2006).
Phylogenetic analysis of the isolated CHIK virus from Andhra Pradesh and Maharastra revealed that the circulating strain was related to the central African genotype (Yergolkar et al. 2006, Naresh Kumar et al. 2007).
There was no previous record of CHIK virus infection in the state of Orissa, India. However, sudden onset of cases with suspicion of CHIK infection appeared in large numbers in the state during 2006. Outbreak investigation was carried out by Regional Medical Research Centre, Bhubaneswar, in two districts of Orissa and confirmed the outbreaks were due to CHIK infection.
Materials and Methods
Outbreak site
Investigation was carried out in three affected villages, namely, Bajapura, Meripur, and Dobandhia, in the Cuttack district and one village, that is, Barkul, in Kendrapara district in the state of Orissa, in the eastern coast of India (Fig. 1). The villages of Cuttack district were contiguous, narrowly separated by river branches, and located about 80 km from the state capital, Bhubaneswar, whereas the affected village of Kendrapara was located on a river delta, approximately 180 km from the state capital. The affected areas of the two districts were around 120 km apart with no regular population movement between them. These villages were situated on the coastal plane land, 15–30 km away from the Bay of Bengal. The affected districts were densely populated, with a population density of 511/km2 and 598/km2 area in Kendrapara and Cuttack district, respectively. The average number of family members per household in the outbreak area of Kendrapara and Cuttack district was 5.9 and 6.1, respectively (Table 1).
Outbreak occurred in September and October 2006, which coincided with postmonsoon period (monsoon rains from mid-June to August) preceded by a bout of rainy days. The average humidity was 80–85% in both the districts during the outbreak period. During this season the villages were surrounded by growing paddy fields and houses with green gardens.
Clinicoepidemiological survey
During the second week of September 2006, local news papers reported about the occurrence of a large number of undiagnosed fever cases with or without joint pain in some villages of the state. Simultaneously, the Surveillance Cell of the State Health Department received information through its peripheral network and this center was informed.
The outbreak was investigated by a team that included epidemiologists, clinicians, entomologists, laboratory technicians, census takers, and insect collectors in the affected villages during September and October 2006 upon earliest report from the State Health Department. A house-to-house survey was conducted in the reported villages to search for affected individuals. An individual with any of the symptoms of fever, joint pain, joint swelling, rash, conjunctival congestion, or myalgia during the outbreak period was recorded as a clinical case. Individual respondents were interviewed and examined by clinicians. Data on sociodemography, history of illness, and physical signs (general and systemic) were recorded. Symptomatic individuals were provided domiciliary treatment with paracetamol and/or cetrizine. Blood samples were drawn for serological investigation from symptomatic individuals who provided informed written consent for intravenous collection. Consent was obtained from the parent or guardian for children below 18 years of age before examination.
The samples were subjected to serological investigation for detection of specific immunoglobulin M (IgM) antibody to dengue and CHIK virus infection, which were the two differential diagnoses.
Detection of anti-CHIK IgM antibody by enzyme-linked immunosorbent assay
Anti-CHIK IgM antibody in the serum was detected by enzyme-linked immunosorbent assay (ELISA) using test kit produced by National Institute of Virology, Pune, India, after the instruction provided. Serum samples (1/100-fold) were added to anti-human IgM–precoated ELISA plate and incubated at 37°C for 1 h in a humid chamber. Positive and negative control samples were also included to validate the assay system. Then, the plate was washed three times with wash buffer (phosphate-buffered saline containing Tween 20), and 50 μL of CHIK antigen (African genotype) was added to each well and incubated for 1 h at 37°C in a humid chamber. The plate was washed again and 50 μL of biotynilated anti-CHIK monoclonal antibody added to each well. The plate was further incubated at 37°C for 1 h in a humid chamber; after washing, peroxidase-conjugated Avidin was added to each well and kept for 1 h at 37°C. After final wash, tetramethyl benzidine (TMB) substrate was added. The reaction was stopped after 10 min by adding 1 N H2SO4 and read at 450 nm using an ELISA reader (Bio Rad, Richmond, CA). The test was considered valid when the optical density (OD) values of positive and negative controls were within the prescribed limit.
The sample was considered positive for IgM antibody if the OD value of the test sample/OD value of negative control was ≥2.1
All the samples were also tested for dengue IgM using test kit (Dengue serotype 2 antigen) developed by National Institute of Virology, Pune, India.
Entomological survey
Entomological survey was conducted to determine the presence of vector mosquitoes (adult and larvae) possible for CHIK virus transmission. Purposive sampling was adopted, and every fifth house from both sides of the lanes was inspected for resting mosquitoes and water containers for larvae (Teodulfo et al. 2008). Resting adult collection of Aedes was carried out during day time from 7 am to 2 pm from the houses (dark humid places, underside of furniture, hanging objects such as clothes and curtains, and the walls) and cow sheds (Christophers 1960). Adult mosquito species were collected by trained insect collectors using sucking tube and mechanical aspirator. Adults were then brought to the laboratory and identified using keys of Barraud (1934). The per-man-hour density (PMHD) for each species was calculated as the number of mosquitoes collected by a person in 1 h.
For collection of larvae, almost all containers with water were searched inside and outside of each sampled household and larvae collected using dip method or by a Pasteur pipette in case of small containers (WHO 1975). The searched Aedes breeding sites included drum, earthen pot, cemented tank, bucket, tire, tin/plastic container, coconut shell, cut bamboo, and banana axil. Collected larvae were brought to the laboratory, reared to adults, and identified as above. Larval collection data were used to calculate House, Container, and Breteau indices using following formulas: A. House index (percentage of houses positive for larvae of Aedes mosquito) = (Number of houses positive for Aedes larvae/number of houses inspected) × 100 B. Container index (percentage of containers positive for Aedes breeding) = (Number of containers positive for Aedes larvae/number of containers inspected) × 100 C. Breteau index = (Number of containers positive for Aedes larvae/number of houses inspected) × 100
Results
The investigating team observed that the present outbreak started during the second week of September 2006 and it declined toward the second week of October in Cuttack, whereas it persisted till the end of October in Kendrapara district. The number of households affected and clinical cases in the affected villages are shown in Table 1. It was noted that 83% of households in Kendrapara and 68% in Cuttack district had clinical cases. About 30.1% and 29.3% of the total population were sick in outbreak area of the above districts during the present outbreak. All ages and both sexes were affected (Table 2). Individuals of higher age group were significantly affected than the younger age group in Meripur (χ 2 = 17. 4), Barkul (χ 2 = 47.0), and Bajpura (χ 2 = 15.9), but not at Dobandhia (χ 2 = 8.2) village. Mantel–Haenszel summarized chi-square test to see the difference between the sexes in different age groups was significant (p < 0.05) in Dobandhia and Meripur, but not significant in Bajpura and Barkul villages. Figure 2 shows the epidemic curves based on the onset of illness of clinical cases in Barkul village of Kendrapara district and Bajapura, Dobandhia, and Meripur villages of Cuttack district, respectively. The curves revealed multiple peaks, which indicated that the epidemic was propagative in nature (Page et al. 1995).
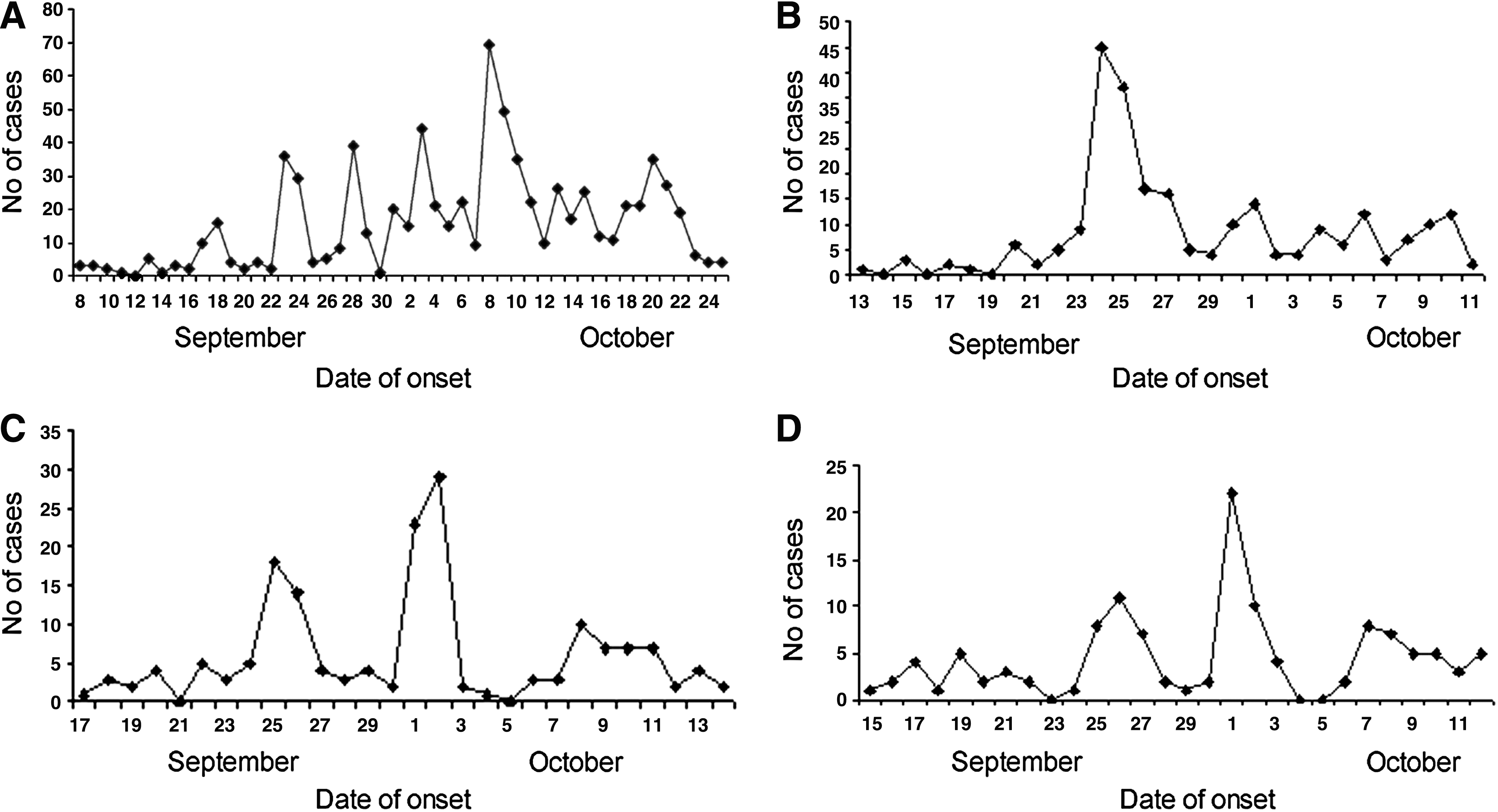
Epidemic curve showing day-wise onset of clinical cases of CHIK in the study villages (2006). (
Sex distribution expressed as the percentage of individuals from the particular sex out of total population in the respective age group.
Acute onset of fever or joint pain was observed to be the usual symptoms to start with. Common symptoms noted were fatigue (91.9%), fever (89.1%), headache (74.4%), head reeling (79.1%), joint pain with/without swelling (63.8%), maculopapular rash with/without itching (33.9%), and conjunctival ingestion (21.4%). Hemorrhagic manifestation (3.3%) was unusual. Epistaxis and purpuric hemorrhages on both trunk and extremities were observed. Anorexia, nausea, and pain in abdomen were the other associated minor symptoms. Majority of symptoms (fever, headache, head reeling, conjunctival ingestion, and rash) subsided within 3–5 days, whereas joint pain and swelling was persisting beyond a week. All the individuals were successfully treated symptomatically with common analgesics and antihistamines like paracetamol and cetrizine. Antihistamines were used when the rash was associated with itching. No death was noted due to the illness from the affected areas during the outbreak. CHIK and dengue virus infection was considered for the differential diagnosis based on the individual symptoms and epidemic form of presentation (Chhabra et al. 2008).
Serum samples were collected from 101 and 116 symptomatic individuals from Kendrapara and Cuttack district, respectively, which were tested for the presence of anti-CHIK IgM antibody. The seropositivity rate was 63.3% (64/101) and 40.5% (47/116) in the respective samples. Dengue IgM antibody was not detected in any of the samples.
Travel history of index cases was recorded from the villages. Two adult men from the village Bajpura gave history of recent travel to Chennai, Tamil Nadu, India, during September 2006, and there were reports of CHIK outbreak in the state of Tamil Nadu during that period (Selvavinayagam 2007). They had the symptoms of illness already started at Chennai and were subsequently confirmed serologically as CHIK infected. They were the initial cases from that village. In other villages the index cases did not reveal any relevant history of movement.
Mosquito collection from the two studied districts during the survey is shown in Table 3. Twelve species of adult mosquitoes belonging to four genera, that is, Anopheles, Aedes, Armigeres, and Culex, were found in outbreak areas of both the affected districts. A total of 507 and 529 mosquitoes were collected from the Cuttack and Kendrapara sites, out of which Aedes vector population (Ae. aegypti and Ae. albopictus) was 19.3% (98/507) and 21.4% (113/529) in the Cuttack and Kendrapara sites, respectively. The density (PMHD) of Ae. aegypti, Ae. albopictus, and Ae. vittatus was 4.2, 7.6, and 1.28 in the Kendrapara and 3.7, 6.2, and 0.8 in Cuttack sites, respectively (Table 3). Adult mosquitoes were found both in the living rooms and cattle shed. The test of proportion was carried out to see the difference in the density of Ae. albopictus, Ae. vittatus, and Ae. aegypti in human dwellings and cowsheds. The difference was nonsignificant (p > 0.05) for all the three species from the villages of Cuttack district and Ae. aegyppi from Kendrapora district. However, the difference in density was significant for Ae. vittatus (Z = 2.90, p < 0.001) and Ae. albopictus (Z = 4.169, p < 0.001) in Kendrapara district. There was no difference in the density of adult mosquitoes between the two districts (t = 0.784, p = 0.441).
Larvae were collected from 121 households and 488 breeding containers in the Kendrapara site, out of which 23 houses and 92 containers were positive for Aedes larvae. In the villages of Cuttack district, 15 out of 87 households and 64 of 377 containers showed the presence of Aedes larvae. The House, Container, and Breteau indices calculated were 19, 18.9, and 76 in Kendrapara and 17.2, 16.9, and 73.6 in Cuttack, respectively (Tables 4 and 5).
Discussion
The present study confirmed the outbreak of CHIK in Kendrapara and Cuttack districts of Orissa, India, during September–October 2006. CHIK outbreaks were reported from other parts of the country since December 2005, especially in states like Karnataka, Tamil Nadu, Maharastra, Gujarat, and the bordering state of Andhra Pradesh (Mavalankar et al. 2007b, CDC Report 2007–2008, Sudeep and Parashar 2008). In the present outbreak 24–35% of the population of the villages suffered from the illness during the outbreak period, and no sex or age differences could be observed (prevalence ratio, 0.82; 95% CI: 0.75–0.90). This was similar to the epidemics during 2006 affecting other states of the country, where case rate reached up to 45% in some areas (WHO, SEARO 2006). The 1973 Barsi outbreak also reported 37.5% morbidity affecting all ages and both sexes (Padbidri and Ganeswar 1979). However, the outbreak investigation has shown greater involvement of higher age groups in three villages and female population in two of the four villages, but the factors influencing this could not be ascertained from the study. The serological tests conducted on samples from symptomatic individuals in the affected areas of Kendrapara and Cuttack districts have shown anti-CHIK IgM antibody positivity of 63% and 40%, respectively, which indicated recent infection due to CHIK virus (Porter et al. 2004, Sergon et al. 2007). The seropositivity rate was similar to other CHIK outbreaks investigated in the past. In the serosurvey of CHIK infection on Grande Comore island, Union of Comoros, in the year 2005, prevalence of IgM antibody was found to be 60% (Sergon et al. 2007). Senegal outbreak in 1996–1997 has shown antibody prevalence of 35.3% (Thonnon et al. 1999). Such a high rate of morbidity might indicate lack of immunity due to previous exposure to CHIK infection in the affected region, which favored occurrence of epidemic (Ravi 2006). Although there were no reports on seroprevalence of CHIK antibody from the state of Orissa, suggesting absence of herd immunity, few studies in India have shown a low prevalence of CHIK antibody in the general population in the absence of an epidemic. A community-based serosurvey conducted at Calcutta a decade ago revealed a low CHIK IgG prevalence of 4.37% (Neogi et al. 1995), and that in Andaman and Nicober island was 15.3% (Padbidri et al. 2002). In another survey antibody positivity was found to be 10.8% in Chennai city in 1956, where majority of seropositives were of higher age group (>40 years), but the city experienced another outbreak during 1964, which supports waxing immunity as the cause of outbreak (Banerjee 1965).
The major symptoms observed were fever (89.1%) and joint pain (63.8%), along with other constitutional symptoms, which were similar to those present in other investigated CHIK outbreaks (Thaikruea et al. 1997, Porter et al. 2004, Ravi 2006, Peyrefitte et al. 2007). In our study, the symptoms were short lasting (3–5 days) except pain and swelling of joints, which were persisting beyond a week. In the Comore Island outbreak, 2005, it was similarly noted that the mean duration of joint pain was 9 days (Sergon et al. 2007). Although morbidity was high, no case fatality was noted in the reported outbreak. Similarly, in the other affected states of India, millions were affected with morbidity but sporadically with mortality. Reports suggested few deaths especially from Telengana region of Andhra Pradesh (Krishna et al. 2006). The disease was found to be self-limiting with minimal supportive and symptomatic medication. Most cases were treated with paracetamol at home. Other studies also reported use of the above drug for symptomatic relief (Sergon et al. 2007). In the absence of specific antiviral remedy, this information would be useful for outbreak management.
Ae. aegypti and Ae. albopictus are known vectors of the CHIK virus (Delatte et al. 2008). In our study the Aedes vector (Ae. aegypti and Ae. albopictus) population in Cuttack and Kendrapara districts comprised 19.3% and 21.4% of the total vector population, respectively, suggesting a high prevalence of the Aedes vectors in the study area. The PMHD of Ae. aegypti was 3.7 and 4.2, for Ae. albopictus it was 6.2 and 7.6, and for Ae. vittatus it was 2.6 and 0.8 in Kendrapara and Cuttack districts, respectively. Ae. vittatus may also be a potential vector for CHIK virus transmission in the study area besides other species (Lahariya and Pradhan 2006). Larval indices were used to find out the population at risk due to exposure to mosquito bites. High values of the larval indices (House index >17%, Container index >15%, and Breteau index >70%) were observed in both study areas, which were much higher than the recommended indices (House index >5% and Breteau index >20%) that reflected the intensity of vector breeding which facilitated transmission of CHIK in the study area. Similar observations of higher values of these indices were also reported in other CHIK-affected areas (Sang et al. 2008, Teodulfo et al. 2008).
This investigation confirmed the emergence of CHIK infection in the state of Orissa. It could be due to the import of cases through population movement from other states with reported CHIK circulation, which was supported by the travel history of index cases recorded in one of the study villages. This also warrants likely spread of the virus to other parts because of the wide prevalence of the transmitting vectors in the region (Nagpal and Sharma 1983, 1985) and population movement (Plaloux et al. 2007). The presence of all three species of Aedes, that is, aegypti, albopictus, and vittatus, along with the anophelines and culicines, also indicated potential threat of arboviral infections besides CHIK, which necessitates public health measures in the region.
Footnotes
Acknowledgment
The authors wish to acknowledge Dr. A.S. Acharya for supporting in statistical analysis, and the team members Mr. K. Dhal, Mr. T. Moharana, Mr. R.N. Nayak, and Mr. S.K. Mishra of Clinical and Epidemiology Division and Mr. G.D. Mansingh, Mr. S.S. Beuria, Mr. C.S. Tripathy, Mr. B. Pradhan, and Mr. G. Simachalla of Entomology Division for their support and activities during the field survey and laboratory investigation. The authors are also thankful to the Indian Council of Medical Research, New Delhi, India, for providing financial assistance.
Disclosure Statement
No competing financial interests exist.