
Abstract
The objectives of this study were to identify and characterize temporal clusters of bovine Salmonella cases at a veterinary medical teaching hospital and to determine which clusters were likely to have involved nosocomial transmission. Data on fecal Salmonella shedding status, serotype, and antimicrobial resistance were collected retrospectively for all cattle admitted to the Cornell University Equine and Farm Animal Hospital between January 1, 1996, and June 1, 2007. Pulsed-field gel electrophoresis (PFGE) was performed on all available isolates. Cluster analysis was used to identify temporal clusters of cases. A total of 5398 cattle were admitted during the study period; the prevalence of fecal Salmonella shedding among clinical suspects was 6.5%, whereas that among nonsuspects tested through routine surveillance was 2.5%. Eight temporal clusters (including 57 cattle) were investigated as possible outbreaks involving nosocomial transmission, ranging in size from 4 to 10 cases. All but one cluster were centered over the month of August or September. A total of 15 Salmonella serotypes were represented, with the most common being Typhimurium (33%), Newport (23%), and Agona (12%). Among the isolates available for PFGE analysis, there were 19 PFGE types represented. The majority of temporal clusters during the study period were not nosocomial in origin. However, two of the clusters were outbreaks directly resulting from nosocomial Salmonella transmission, based on case histories, serotype data, antimicrobial resistance patterns, and PFGE analysis. The clear seasonal pattern exhibited by these clusters underscores the need for heightened Salmonella vigilance during the late summer and early fall. The combination of statistical methods, routine bacteriologic data, and PFGE analysis is an effective means of conducting surveillance and outbreak investigations in a hospital setting.
Introduction
Several studies have been published on salmonellosis in equine hospital patients, and some of these have specifically investigated the epidemiology of nosocomial infections (Hird et al. 1984, Carter et al. 1986, House et al. 1999, Ekiri et al. 2009). Risk factors for nosocomial Salmonella infection among hospitalized horses include admission because of colic (Hird et al. 1984) or large colon impaction in particular (House et al. 1999), abdominal surgery (Ekiri et al. 2009), parenteral antibiotic administration (Hird et al. 1984, House et al. 1999), nasogastric intubation (Hird et al. 1984), an increase in the mean daily ambient temperature (House et al. 1999), and shedding of the same Salmonella serotype by other equine patients in the days before admission (House et al. 1999). In contrast, little has been published on Salmonella infections among hospitalized cattle, and we are unaware of any reports that focus on nosocomial transmission.
In this study, we examined data for cattle admitted to the Cornell University Equine and Farm Animal Hospital in Ithaca, New York, between January 1, 1996, and June 1, 2007. Our objectives were to identify and characterize temporal clusters of Salmonella cases over this duration and to determine which clusters were very likely to have involved nosocomial transmission, using patient histories, serotype data, antimicrobial resistance patterns, and pulsed-field gel electrophoresis (PFGE) analysis. In addition, we sought to fully describe the nosocomial clusters as a means of documenting the factors that we believe in hindsight contributed to the transmission of Salmonella in this hospital; we hope that such information can be used to help prevent nosocomial outbreaks in the future.
Materials and Methods
Study design
As part of a larger project to determine prevalence and risk factors for Salmonella infection in cattle admitted to the Cornell University Equine and Farm Animal Hospital between January 1, 1996, and June 1, 2007, data were collected retrospectively using the hospital's computerized medical records database (Cummings et al. 2009). Information collected for each bovine patient included age, breed, sex, state of origin, date of admission, and diagnoses. If bacteriologic culture for Salmonella was performed, the date of testing, result, serotype, and antimicrobial resistance profile were also gathered from the records. Fecal Salmonella testing took one of two forms. The most commonly used test was the Salmonella surveillance culture, intended to be performed on samples obtained from all admitted cattle that did not have clinical signs consistent with salmonellosis. This test was primarily a biosecurity measure aimed at identifying subclinical shedders that posed a threat to the hospital environment. The second test was used for those cattle presenting with a combination of typical signs of salmonellosis (diarrhea, fever, and dehydration) or for cattle originating from a farm with a history of either endemic or epidemic salmonellosis (based on either voluntary information provided by the referring veterinarian or recollection of the hospital clinician regarding previous admission of confirmed Salmonella-positive cases from that farm). These patients were tested with a specific Salmonella culture or a broad enteric bacteriology culture panel that included Salmonella, depending on the age of the patient (calf vs. adult) and preference of the attending clinician. The specific Salmonella culture was more commonly selected for samples from adult cattle, whereas the enteric culture panel was generally used for samples from calves because Escherichia coli is a common bacterial pathogen within this age group.
Sample collection
For the purpose of Salmonella testing, clinicians and students in the Equine and Farm Animal Hospital were asked to routinely collect at least 10 g of fecal matter from each patient on the day of admission, using an examination glove. The sample was packaged in a plastic specimen cup with a tight lid and then transported directly to Cornell's Animal Health Diagnostic Center for bacteriologic culture. Fecal samples collected after 5:00
Microbiologic procedures for Salmonella detection
Personnel at the Animal Health Diagnostic Center utilized standard bacteriologic culture methods to isolate Salmonella from feces. Salmonella culture procedures for both the surveillance and clinical suspect samples included selective enrichment as an initial step. Individual fecal swabs from sample containers were added to 10 mL of Tetrathionate broth (10% w/v; Difco, Detroit, MI) containing 0.2 mL of iodine solution, and the mixture was incubated at 42°C for 18–24 h. After incubation, the sample–broth mixture was streaked onto Brilliant Green agar with novobiocin (BGN; Becton Dickinson and Company, Franklin Lakes, NJ) and xylose lysine tergitol 4 (XLT-4) selective media, and both plates were incubated at 37°C for 18–24 h. Red colonies (lactose nonfermenting bacteria) on BGN and black colonies (H2S-producing bacteria) on XLT-4 were inoculated into Kligler iron agar slants and then incubated at 37°C for 18–24 h. XLT-4 plates without suspected colonies were reincubated at 37°C for an additional 18–24 h before checking again for characteristic black colonies. Colonies on Kligler iron agar slants that exhibited the biochemical properties of Salmonella were then serogrouped by slide agglutination using standard protocols and grouping sera. Those colonies that were positive by slide agglutination were subsequently identified as Salmonella using the Sensititre Automated Microbiology System's A80 panel (TREK Diagnostic Systems, Cleveland, OH). Serotyping of confirmed Salmonella isolates was performed at the U.S. Department of Agriculture, Animal and Plant Health Inspection Service (APHIS) National Veterinary Services Laboratories in Ames, Iowa. Antimicrobial susceptibility of Salmonella isolates was determined by use of the broth dilution method; minimal inhibitory concentrations (MIC) were established for each isolate against a standard bovine panel in use at the Animal Health Diagnostic Center (AHDC) at the time of submission (Sensititre; TREK Diagnostic Systems). Depending on the panel, we selected seven to nine drugs that are relevant to Salmonella and that represent a broad range of antimicrobial classes, although not all have practical applications in bovine medicine. Clinical and Laboratory Standards Institute guidelines were used to interpret MIC values (Clinical and Laboratory Standards Institute 2008).
In addition to the enrichment process described above, direct culture of all clinical suspect samples (but not surveillance samples) on solid media was concurrently performed, regardless of whether the animal was tested with a specific Salmonella culture or an enteric culture panel that included Salmonella. This was intended to permit a quicker diagnosis when clinicians were suspicious of Salmonella infection. Individual fecal swabs were directly inoculated onto trypticase soy blood (TSB) agar with 5% sheep blood, Levine eosin methylene blue (EMB) agar, and BGN.
Statistical analysis
Data were imported into SAS (version 9.1; SAS Institute, Cary, NC) for analysis. The prevalence of Salmonella fecal shedding among tested bovine patients was calculated; cattle tested for Salmonella more than once were considered positive if at least one fecal culture was positive. Using PROC FASTCLUS, a cluster analysis of cases was performed to search for cattle with positive Salmonella results grouped by test date. Consideration as a potential outbreak cluster involving nosocomial transmission required at least three positive cattle within a 30-day period.
Pulsed-field gel electrophoresis
PFGE was performed on all study isolates that were archived in the Animal Health Diagnostic Center's culture collection, using the standard CDC PulseNet protocol for Salmonella subtyping (Ribot et al. 2006). XbaI was used as the restriction enzyme. XbaI-digested Salmonella enterica serotype Braenderup (CDCH9812) DNA was used as a reference size standard (Hunter et al. 2005). Electrophoresis was performed for 21 h using the CHEF Mapper apparatus (Bio-Rad Laboratories, Hercules, CA). Pattern images were captured with a Bio-Rad Gel Doc and Quantity One 1D Analysis software (Bio-Rad Laboratories). PFGE patterns were then analyzed and compared using the BioNumerics version 3.5 software (Applied Maths, Saint-Matins-Latem, Belgium). Similarity clustering analyses were performed with BioNumerics using the unweighted pair group method with arithmetic mean and the Dice correlation coefficient with a tolerance of 1.5%. PFGE patterns differing by one or more bands were considered different.
Classification of Salmonella infections as nosocomial
The decision to categorize a Salmonella infection as nosocomial was conditional on the following information: recovery of an isolate with a serotype, antimicrobial resistance pattern, and PFGE type that matched those of the index strain, development of diarrhea or fever at least 48–72 h after admission, and, if applicable, having positive Salmonella culture results following an initial negative culture.
Results
During the study period, 5398 bovine patients were admitted to the Cornell University Equine and Farm Animal Hospital. Among these, 2020 (37.4%) were tested with the Salmonella surveillance culture, and the prevalence of fecal Salmonella shedding was 2.5% (50/2020) within this group. A total of 768 bovine patients (14.2%) were classified as clinical salmonellosis suspects and therefore were tested with either a specific Salmonella culture or an enteric bacteriology culture panel that included Salmonella; the prevalence of fecal Salmonella shedding within this group was 6.5% (50/768).
Cluster analysis of cattle with positive Salmonella results revealed 23 temporal clusters ranging in size from 2 to 10 cases. Eight of these clusters included three or more positive animals within a 30-day time frame (Table 1), and these were investigated as possible outbreaks involving nosocomial transmission. The eight clusters of interest ranged in size from 4 to 10 cases, with the median being seven cases per cluster. With the exception of one cluster, all were centered over the month of August or September. A total of 57 animals were included in these clusters; of these, 24 (42.1%) were male or female calves, 32 (56.1%) were cows, and 1 (1.8%) was a mature bull. Thirty (52.6%) were clinical salmonellosis suspects presenting with a combination of typical signs (diarrhea, fever, and dehydration) or originating from a farm with a history of Salmonella, while 27 (47.4%) were nonsuspect animals detected through routine surveillance. There were 15 Salmonella serotypes represented, with the most common being Typhimurium, including the Copenhagen variant (33%), Newport (23%), and Agona (12%). Among the 57 animals involved in the 8 clusters under investigation, 42 isolates were available for PFGE analysis. A total of 19 PFGE types were represented (Fig. 1), with the number of isolates corresponding to each type ranging from 1 to 11.
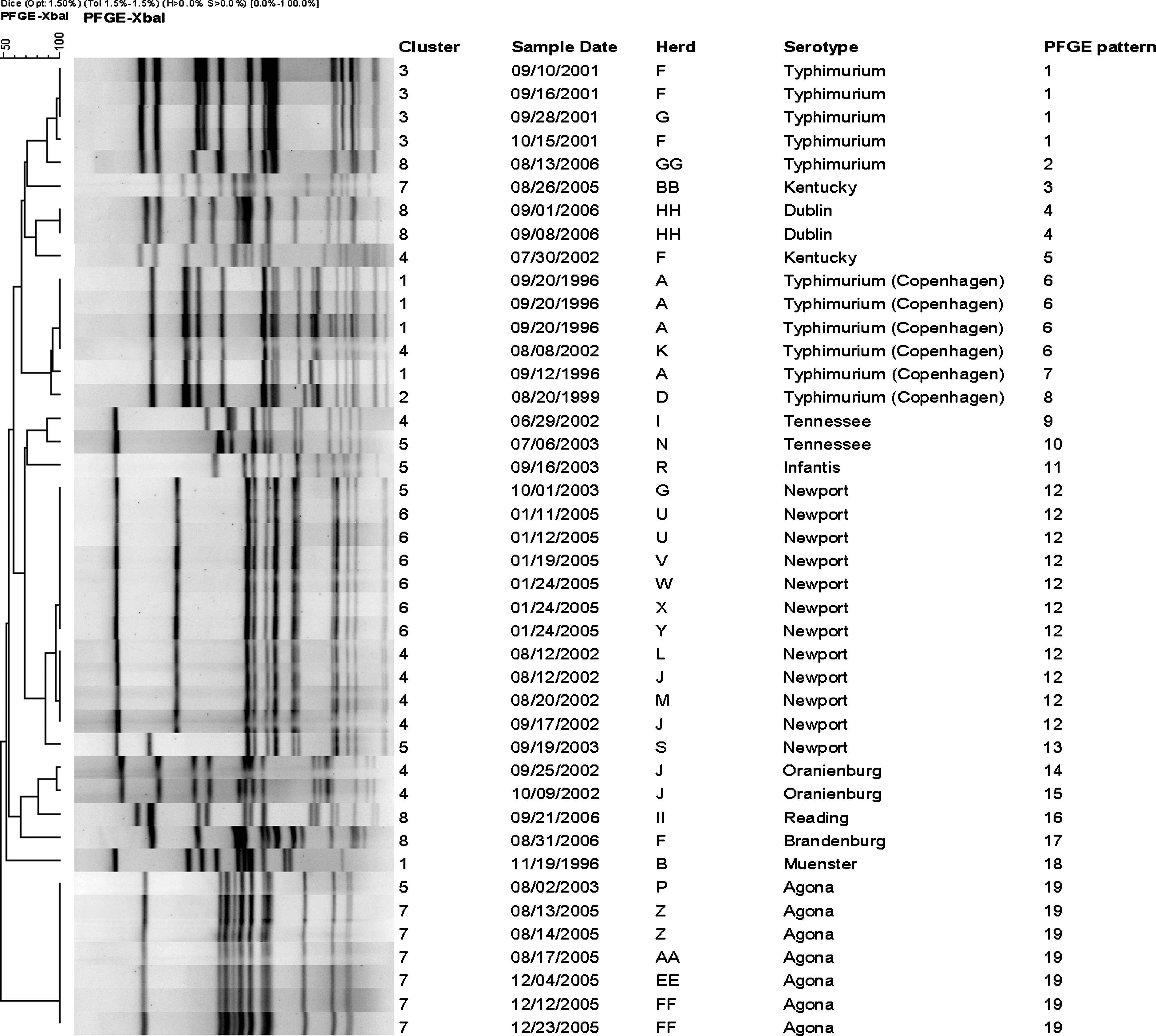
XbaI pulsed-field gel electrophoresis (PFGE) patterns for 42 isolates representing the 8 case clusters under investigation (15 isolates were not available for pulsed-field gel electrophoresis analysis).
PFGE, pulsed-field gel electrophoresis; Amp, ampicillin; Ffn, florfenicol; Fis, sulfisoxazole; Gen, gentamicin; Oxy, oxytetracycline; Sdm, sulfadimethoxine; Spe, spectinomycin; Sxt, trimethoprim/sulfamethoxazole; Tet, tetracycline; Tio, ceftiofur; NA, not available.
Clusters 1, 2, 3, and 4 occurred during the late summer and early fall of 1996, 1999, 2001, and 2002, respectively (Table 1). Cluster 1 contained three calves and one cow from the same herd that was experiencing an outbreak of salmonellosis (herd A), and these animals presented in September 1996. All four were positive for the Copenhagen variant of Typhimurium. Antimicrobial susceptibilities for three of the isolates (from the cow and two of the calves) were determined, and the MIC was measured against a panel of seven antimicrobial agents: ampicillin, ceftiofur, enrofloxacin, gentamicin, sulfisoxazole, tetracycline, and trimethoprim/sulfadiazine. The MIC value for each drug was identical in each of the calf isolates, indicating in vitro resistance to three of the seven antibiotics. The cow isolate displayed the same overall resistance pattern, although the actual MIC value for ceftiofur was higher. The three calf isolates all shared the same PFGE type (type 6, Fig. 1), while the cow isolate differed from this pattern by one band (type 7). Two other animals admitted later in the fall also tested positive for Salmonella and were included in this temporal cluster, but their infections were presumably not nosocomial because both had presented to the hospital with a chief complaint of diarrhea and were positive on the initial admission sample.
Similarly, cluster 2 contained three calves from a herd that was having an outbreak of salmonellosis (herd E), and these animals presented in late September and early October 1999. All were positive for Typhimurium. Antimicrobial susceptibilities for the three isolates were determined, and the MIC was measured against a similar panel of seven drugs (florfenicol replaced sulfisoxazole, and trimethoprim/sulfamethoxazole substituted for trimethoprim/sulfadiazine). The MIC value for each drug was identical in all three isolates, indicating in vitro resistance to five of the seven antibiotics. None of the three calf isolates were available for PFGE typing. The only other animal in this temporal cluster was a cow admitted in August of that year for mastitis, but this cow was found via routine surveillance to be shedding a different serotype with a unique antimicrobial resistance profile.
Cluster 3 comprised nine cases, including five cows from a farm with a history of endemic salmonellosis (herd F). These five were all admitted for surgical repair of a left-displaced abomasum (LDA) between September and October 2001. Four of these animals tested positive for Typhimurium; the fifth was reported as being positive for Salmonella serogroup B (the same serogroup as Typhimurium) but was not serotyped. Antimicrobial susceptibilities for four of the isolates were determined, and the MIC was measured against a panel of nine drugs: ampicillin, ceftiofur, enrofloxacin, florfenicol, gentamicin, oxytetracycline, spectinomycin, sulfadimethoxine, and trimethoprim/sulfamethoxazole. The MIC value for each antimicrobial agent was identical in all four isolates, indicating in vitro resistance to five of the nine drugs. Three of the four isolates were available for PFGE analysis, and these were found to share the same PFGE type (type 1) as well. Also included in this temporal cluster were three calves from a herd that was having an outbreak of salmonellosis (herd H). These animals presented in November 2001, and all were positive for the Copenhagen variant of Typhimurium. Antimicrobial susceptibilities for all three of the isolates were determined, and the MIC was established for the same nine antimicrobial agents; the MIC value for each was the same in all three isolates, again indicating in vitro resistance to five of the nine drugs. None of the three isolates were available for PFGE typing. The final animal in this cluster was a cow admitted in late September of that year for repair of an LDA. Routine surveillance testing revealed that this cow was shedding Typhimurium, and the antimicrobial resistance profile and PFGE type (type 1) of this isolate matched those of the other Typhimurium isolates obtained between early September and mid-October 2001. This was likely a nosocomial infection, but the animal did not develop clinical signs while hospitalized and was discharged shortly after surgery.
Cluster 4 contained a total of 10 cases, including 5 cows from a different farm with a history of endemic salmonellosis (herd J). These animals were all admitted for surgical repair of an LDA between August and October 2002. Two of these animals tested positive for Newport, while the other three were found to be shedding Oranienburg. Antimicrobial susceptibilities for both Newport isolates were determined using the same nine-drug panel. The MIC for each antimicrobial agent was the same in both, indicating in vitro resistance to five of the nine antibiotics; these two Newport isolates also shared the same PFGE type (type 12). This temporal cluster included an additional five animals admitted late in the summer of that year, all from separate herds. Three of these tested positive for serotypes and PFGE types that were unique to those individual animals. However, the other two were found to be shedding Newport; the antibiotic resistance profiles and PFGE types (type 12) of these isolates matched those of the two Newport isolates from the other animals in this cluster, suggesting nosocomial transmission. Notably, both animals had remained in the hospital for an extended period of time. The first was a cow presenting in the beginning of August with a history of lethargy and decreased appetite. This cow developed diarrhea during the latter part of her hospital stay (15 days) and was subsequently found to be shedding Newport. The second animal was a calf presenting in early August with lameness of noninfectious etiology. Near the midpoint of this calf's hospital stay (19 days), a Salmonella culture came back positive for Newport, although this animal never developed clinical signs while hospitalized. Both of these patients were discharged later in the month.
Clusters 5 and 8 occurred during the late summer and early fall of 2003 and 2006, respectively (Table 1). These differed from the previous clusters in that they did not consist primarily of multiple animals from herds that were experiencing either endemic or epidemic salmonellosis. Cluster 5 included two calves and five cows, all from different herds. Two animals had presented to the hospital with diarrhea and were positive on the initial admission sample, and the other five were discovered to be shedding Salmonella through routine surveillance. All were admitted between July and October 2003. Six serotypes were represented in this cluster, with Newport being the only one isolated from more than a single animal. The first cow shedding Newport had been admitted in mid-September for decreased appetite and a possible LDA, while the second cow presented with a chief complaint of diarrhea at the end of that month. However, the two isolates had unique antimicrobial resistance profiles and PFGE types.
Cluster 8 included two calves and three cows admitted during August and September 2006. The calves came from a herd that had experienced a recent rise in calf illness and mortality, with typical signs including fever, lethargy, and anorexia, eventually followed by dyspnea and diarrhea. Adult cattle in this herd were apparently unaffected. Both calves tested positive for Dublin and were ultimately euthanized. Antimicrobial susceptibility testing was performed on both isolates using the same panel, and both had matching MIC values which indicated in vitro resistance to six of the nine antibiotics; these two Dublin isolates also shared the same PFGE type (type 4). The three cows in this temporal cluster each came from different herds. They were not clinical suspects on admission, but all were found to be shedding Salmonella via routine surveillance testing. Serotypes and PFGE types were unique to these three animals.
In contrast to the temporal clusters previously described, clusters 6 and 7 appeared to be caused by nosocomial transmission. Cluster 6 included a total of seven animals, six of which were admitted in January 2005 (Table 1). Around the first of the year, a herd owner from a neighboring state had called to discuss an outbreak of profuse diarrhea among his adult animals (herd U), and the consulting clinician advised a veterinary visit from one of the local ambulatory practices. One week later, however, two cows from this farm arrived unannounced at the hospital, late in the evening on January 10. They presented with fever, dehydration, and severe diarrhea containing blood and mucus. These animals were housed overnight in the main bovine ward of the hospital and were not transferred to the isolation ward until the following morning. Salmonella cultures on both patients were positive for Salmonella Newport. Antimicrobial susceptibility testing was performed on one of the isolates, and the MIC values indicated in vitro resistance to six of the nine antibiotics. Both of these isolates shared the same PFGE type (type 12). Of these two presumptive index cases, one cow died the day after admission while the other recovered and was discharged. Over the remainder of the month, four other animals presenting with various chief complaints all tested positive for Newport at least 1 week past their admission date; these four patients had also been tested at admission and were found to have negative Salmonella culture results at that time. All four Newport isolates had the same PFGE type (type 12) as the first two. Antimicrobial susceptibility testing was performed on three of these isolates, and the resistance profiles matched that of the original Newport isolate (except that one isolate had a lower MIC value for sulfadimethoxine). A calf with pneumonia developed diarrhea and was kept in the hospital until clinical recovery and five negative Salmonella cultures were achieved. A bull admitted for abomasal dysfunction had transient mild diarrhea and fever, but this patient also recovered clinically before being discharged. However, two cows that tested positive for Newport (one presented for right-displaced abomasum (RDA), the other for fatty liver syndrome) developed diarrhea and were ultimately euthanized. Thus, the case fatality rate within this cluster was 50% (3/6), including the index animal that died. The only other animal included in this group via temporal cluster analysis was a calf admitted in late October 2004, but this case appears to have had no relationship with the nosocomial outbreak based on the earlier date of hospitalization.
Cluster 7 included a total of nine animals admitted between August and December 2005 (Table 1). Two calves with atresia coli from the same herd were admitted in early August (herd Z), and both developed postsurgical diarrhea. Salmonella cultures on both patients were positive for Agona. Antimicrobial susceptibility testing was performed on these isolates, and the MIC values indicated in vitro resistance to seven of the nine antimicrobial agents. Both of the isolates were available for PFGE analysis, and these were found to share the same PFGE type (type 19). The two calves made uneventful recoveries and were discharged. Over the next few months, four additional calves presenting for various reasons all tested positive for Agona (three of which had also been tested at admission and were initially found to be Salmonella-negative), and all four isolates shared the same PFGE type (type 19) as the first two. Antimicrobial susceptibility testing was also performed on all four of these isolates, and the resistance profiles matched those of the original two Agona isolates. Two newborn calves from the same herd were presented for weakness; one developed a fever and diarrhea while hospitalized, and the other became febrile only. Their Salmonella-positive culture samples were obtained over 2 weeks beyond their admission date. Both recovered clinically and were subsequently found to be Salmonella culture negative before being discharged. Another calf admitted for umbilical hernia also developed diarrhea but recovered before discharge. The fourth calf presented for dyspnea, but there was no clinical evidence of Salmonella infection during hospitalization; this animal was also discharged after successful treatment for an upper airway obstructive disorder. Unlike the previous nosocomial cluster, there was no mortality in this outbreak. The two calves with atresia coli were believed to be the index cases, shedding Salmonella into the environment after corrective surgery. There were also three cows linked with the six calves by temporal cluster analysis, but each had a unique serotype.
Discussion
Cluster analysis is a subjective process, dependent on the criteria used to define the clusters at the outset. In searching for clusters that may have involved nosocomial transmission, it was decided that a cluster had to include at least three positive cattle within a 30-day period to warrant further investigation. Eight of the 23 temporal clusters were selected based upon this guideline. Salmonella infections were regarded as nosocomial if the isolate matched the index strain by serotype, antimicrobial resistance pattern, and PFGE type. Clinical signs of salmonellosis, if present, had to have developed at least 48–72 h after admission; in almost all cases, a positive Salmonella culture result followed an initial negative culture. In particular, PFGE subtyping has been shown to be a highly effective means of analyzing veterinary hospital outbreaks (Amavisit et al. 2001, Schott et al. 2001, Ward et al. 2005, Dunowska et al. 2007) because it facilitates an assessment of epidemiologic relatedness. This study illustrates the utility of combining statistical methods, routine bacteriologic data, and molecular subtyping when conducting surveillance and outbreak investigations.
Bacteriologic culture of feces does not have perfect sensitivity for detecting the presence of Salmonella, and we recognize that some cattle that were shedding Salmonella organisms were presumably missed by culturing. It is also possible that we could have misclassified a Salmonella infection acquired before admission as being nosocomial. However, our classification of cases as nosocomial in origin was supported in all instances by the aforementioned laboratory data used for isolate characterization, in addition to patient historical information.
The majority of temporal clusters during this study period were not nosocomial outbreaks. Clusters 1 through 4 were related to the admission of a number of animals from the same herd that was experiencing either endemic or epidemic salmonellosis. Herd outbreaks of salmonellosis are not unusual in the northeastern United States. For example, a recent field study of over 800 dairy herds in this region identified salmonellosis in 11% of herds (93/831) monitored over a 1-year duration; of these, 57% (53/93) had multiple cases (Cummings et al., 2009). Clusters 1 through 4, in addition to clusters 5 and 8, all occurred in the late summer and early fall. Using data from the same time frame to investigate all Salmonella-positive cattle admitted to our hospital during the study period, the authors found previously that there was a significant difference in the seasonal distribution of clinical suspect cattle with positive culture results, with the highest proportion in the fall and the lowest in the spring (Cummings et al. 2009). It has been reported that fecal Salmonella shedding among dairy cattle on farms is more common in the summer and fall (Fossler et al. 2005), and other studies have found increased shedding during the summer months on dairy farms and at livestock markets (Kabagambe et al. 2000, Wells et al. 2001, Pangloli et al. 2008). Two studies on hospitalized horses had similar results; one found that the number of Salmonella cases reached a peak in September, based on data gathered over a period of 11 years (Carter et al. 1986), and the other found the prevalence of shedding over a 1-year period to be highest between late summer and early fall (Smith et al. 1978). This seasonal association is presumably related to temperature and/or moisture conditions that prevail in the summer and fall months, but whether these conditions are impacting the bacteria or the host species is unclear. Salmonella's ability to thrive in warm, moist environments may increase the odds of host exposure and infection, or perhaps heat stress in cattle leads to suppressed immunity. The seasonal pattern of these clusters underscores the need for heightened awareness during the late summer and early fall. The potential for both nosocomial and zoonotic transmission will likely be greater during this time of year. Although none of the aforementioned temporal clusters originated solely from nosocomial transmission, it is very probable that three of the involved animals (one cow in cluster 3 and a cow and calf in cluster 4) did acquire their Salmonella infection in the hospital, based on the timeline of positive culture status and the serotype, antimicrobial resistance, and PFGE data.
Clusters 6 and 7, on the other hand, appeared to directly result from nosocomial Salmonella transmission. In both instances, we believe that we have identified specific bovine patients as the original source of infection. The admission of two cows with profuse diarrhea into the main bovine ward of the hospital (cluster 6) probably occurred because of their unexpected arrival after normal business hours. It is likely that significant contamination of the hospital environment occurred before the transfer of these patients to the isolation ward the following morning. In addition, three of the other animals in this outbreak cluster overlapped temporally with the admission of the index cases; the bull had already been in the hospital for 10 days, and the calf with pneumonia and cow with fatty liver syndrome were admitted the next day. This suggests that hospital personnel (clinicians, students, technicians, and animal care attendants) and shared equipment may have played a role in spreading Salmonella among these patients.
The presumptive index cases in cluster 7 were two calves that presented for atresia coli. These animals obviously did not have diarrhea on admission and were not considered clinical suspects at that time. Both developed diarrhea postsurgically, leading to contamination of the calf housing area of the bovine ward. Four animals were believed to have become infected via nosocomial transmission in the subsequent few months, and all were calves housed in proximity. Thus, it is suspected that the cleaning and disinfection of this area of the hospital was not adequate to completely eliminate the source of infection. Persistence of Salmonella in the environment for months to even years has been documented in a number of outbreaks (Hartmann et al. 1996, Tillotson et al. 1997, Amavisit et al. 2001, Schott et al. 2001, Ward et al. 2005, Dunowska et al. 2007), suggesting that this is an important cause of nosocomial transmission. Areas of the hospital environment that are most likely to harbor Salmonella include floor drains, stall walls and floors, corners and cracks within stalls, and rubber mats such as those used in anesthetic recovery rooms (Tillotson et al. 1997, Ewart et al. 2001, Schott et al. 2001, Alinovi et al. 2003, Ward et al. 2005). The ability of a single Salmonella clone to persist and cause nosocomial infections in a veterinary hospital for a period of up to several years (Amavisit et al. 2001, Dunowska et al. 2007) is truly an alarming prospect, and it emphasizes the significant danger presented by fecal contamination in this setting. Interestingly, the PFGE subtypes responsible for the two nosocomial outbreaks of 2005 (types 12 and 19) had been identified among bovine patients from different herds during the clusters of 2002 and 2003. However, we have found PFGE types 12 and 19 to be relatively common among New York dairy cattle. Combined with the historical information surrounding the 2005 nosocomial outbreaks, these data suggest separate introductions of these PFGE types into our hospital over time.
The issues that played a role in facilitating these two nosocomial outbreaks are common to large animal hospitals in general, and similar factors have been implicated in multiple Salmonella outbreaks among horses (Hartmann et al. 1996, Tillotson et al. 1997, Schott et al. 2001, Ward et al. 2005). Other factors have also been hypothesized to have contributed to the spread of Salmonella infection during equine outbreaks, and these should be considered as well when dealing with infections among hospitalized cattle. High-pressure power sprayers may be less effective at removing bacterial contamination than scrubbing by hand, and they may in fact promote the aerosolization of infectious particles (Hartmann et al. 1996, Tillotson et al. 1997). This could conceivably lead to inadvertent exposure of patients in neighboring stalls. Rodents located in a teaching hospital during an outbreak have been found to be infected with the same Salmonella serotype (Tillotson et al. 1997); thus, they may serve as vectors of infection, perhaps by contaminating the feed supply.
Antimicrobial resistance was widespread among the cluster isolates; susceptibility testing was performed on 51 of the isolates, and 47 of them (92.2%) displayed in vitro resistance to at least two antimicrobial agents. Although studies of fecal Salmonella shedding among clinically healthy cattle have shown antimicrobial resistance to be uncommon (Wells et al. 2001, Blau et al. 2005, Ray et al. 2007), multidrug resistance was found to be highly prevalent among isolates from cattle with clinical salmonellosis in the northeastern United States (Cummings et al., 2009), particularly among those serotypes that were predominant in the present study (Typhimurium, Newport, and Agona). An association between clinical disease and multidrug resistance would suggest that antimicrobial therapeutic options are likely to be limited when treating cattle with salmonellosis, and it has clear public health implications as well.
The zoonotic potential of Salmonella adds a crucial element to the outbreak clusters reported here, regardless of whether or not they involved nosocomial transmission. While we are unaware of any human cases associated with these clusters, the risk of zoonotic transmission should never be overlooked. Clinicians and hospital administrators are obligated to educate students and clients regarding protective hygiene practices such as washing well after handling animals, thoroughly disinfecting boots and equipment, and not taking boots and coveralls home. Particular care should be taken to prevent exposure of high-risk individuals such as children, the elderly, and those with immunosuppressive health conditions.
A number of measures have been taken in our hospital to reduce both nosocomial and zoonotic transmission of salmonellosis, including biosecurity training sessions for hospital personnel, restriction of human traffic, disinfectant foot mats (The Coburn Company, Whitewater, WI) with Trifectant (Vetoquinol USA, Buena, NJ) in front of every stall and at the entrance to each hospital ward, hand disinfection stations on the walls throughout the wards and at all hand-washing sinks, and disposable gowns and booties for working with neonatal calves, all clinical suspect cattle, and cattle from herds with a history of Salmonella. There is a general decrease in the use of shared equipment between patients; for example, separate thermometers are used for each individual patient and are stored outside the stall. Other types of equipment, such as feed buckets, oral specula, stomach tubes, and balling guns, are disinfected or sterilized after each patient use. All noncleanable surfaces and equipment, such as wooden feed carts, have been removed or replaced with something having a nonporous surface. Any animal that presents as a salmonellosis suspect is admitted directly to the isolation ward, and those cattle that are found to be asymptomatic shedders through surveillance testing are promptly transferred to isolation. Floors throughout the hospital are disinfected with Trifectant or a similar product at least twice daily, using an industrial walk-behind scrubber (Advance Convertamatic; Nilfisk-Advance, Inc., Plymouth, MN). Upon discharge of each bovine patient, the stall is thoroughly cleaned and disinfected with Trifectant. If a given patient was not a clinical suspect but was found to be shedding Salmonella during its stay, that animal's stall is not cleared for subsequent use until Salmonella culture of the stall environment (floor, walls, and feed and water containers) is determined to be negative. In addition, a designated member of the hospital's infection control committee collects at least 15 samples monthly for environmental Salmonella surveillance culture, focusing on floors and drains throughout the hospital, stall walls and floors, and equipment. Finally, the use of PFGE is increasingly being combined with other forms of isolate characterization (serotype and antimicrobial resistance pattern) to monitor for persistence of particular Salmonella strains within the hospital environment and to more quickly recognize potential hospital outbreaks.
Footnotes
Disclosure Statement
No competing financial interests exist.