
Abstract
Corynebacterium ulcerans was isolated from nares of one asymptomatic dog kept in an animal shelter in the metropolitan area of Rio de Janeiro, Brazil. The RNA polymerase beta subunit-encoding gene was sequenced to confirm the species identity. C. ulcerans strains producing phospholipase D, but not diphtheria toxin, are able to cause severe disease in humans, such as pneumonia and granulomatous nodules in pulmonary tissues. The infection rate varies really widely by region, probably because of the variations in the reported infection rates. Dogs with unapparent C. ulcerans infections may be considered as potentially capable of infecting other animals and humans, including pet owners. Medical and veterinary staff should be aware that asymptomatic animals can carry C. ulcerans and cooperate in eliminating infections and monitoring animals also in the developing countries.
Introduction
C. ulcerans can produce diphtheria (DT) and/or phospholipase D (Pld) toxins and may cause human infections mimicking cutaneous and classical respiratory DT with pseudomembranes (Wagner et al. 2001, Dewinter et al. 2005, Tiwari et al. 2008). C. ulcerans is also able to induce clinical signs in the lower respiratory tract such as pneumonia (Hommez et al. 1999, Hatanaka et al. 2003, Mattos-Guaraldi et al. 2008a) and granulomatous nodules in the lungs (Desseau et al. 1995). Similar to nontoxinogenic Corynebacterium diphtheriae strains, the pathogenicity of some C. ulcerans strains may be independent of the DT production. Bacterial strains induce different clinical symptoms depending on the toxin produced and its levels released in the host. Recently, C. ulcerans strains producing DT were isolated from cats with nasal discharge in the United Kingdom (De Zoysa et al. 2005) and from dogs in France (Aaron et al. 2006) and Japan (Katsukawa et al. 2009). Alarmingly, a human case of DT-like illness, caused by a C. ulcerans strain producing a DT-like toxin and likely transmitted by a pet dog with chronic labial ulceration, sneezing, and rhinorrhea, was reported in France (Lartigue et al. 2005).
An emerging infection is one that has newly appeared in the population, or one that has existed but has altered in incidence, geographic range, or character. Many incidences of emergence occur subsequent to the alterations in a combination of pathogen, host, and/or environmental factors. Animal shelters create a uniquely suitable environment for disease emergence. A partial list of factors present in the shelter environment that could promote emergence includes transportation, stress (immunosuppression), increased contact (overpopulation) and exposure, mixing of species, malnutrition, concurrent disease, high animal turnover, and indiscriminant use of antibiotics. Diseases emerging from shelter populations could be risky to animal and/or human populations (Pesavento et al. 2007).
Recently, we described the first case of C. ulcerans human infection in Brazil, and the source of infection was undetermined (Mattos-Guaraldi et al. 2008a). No reports of C. ulcerans infections in animals in the developing countries were found in the literature. Neither was found cases of isolation of C. ulcerans from the nares of asymptomatic dogs in these countries. These facts led us to investigate the occurrence of C. ulcerans in an animal shelter located in the metropolitan area of Rio de Janeiro, Brazil.
Materials and Methods
Ethical procedures
The study was performed in compliance with the guidelines outlined in the Canadian Council on Animal Care (CCAC) and with the Brazilian government's ethical guidelines for research involving animals (Fiocruz Ethic Committee for Animal Experiments—CEUA/FIOCRUZ).
Origin of dogs and clinical evaluation
The occurrence of C. ulcerans was investigated in apparently healthy dogs (adults, puppies, males, and females) kept in an animal shelter located in Niterói city in the metropolitan area of Rio de Janeiro, Brazil. To rule out the presence of any infectious or debilitating diseases, including dermatoses and the more obvious physical and behavioral abnormalities, a general assessment of each animal's condition and nutritional status was recorded as previously described (CCAC 1984).
Clinical evaluation of the animal infected with C. ulcerans included tests for the indicators of renal (urea and creatinine determination) and hepatic (glutamic-oxaloacetic transaminase and glutamic-pyruvic transaminase) functions. Additionally, a blood count including leukogram, an abdominal ultrasound, an echocardiogram, and chest X-rays were performed.
Collection and culture of microorganisms
Eye and nasal swabs were obtained from 60 dogs and inoculated onto the chocolate tellurite agar plates and incubated at 35°C for 72 h (Mattos-Guaraldi and Formiga 1998, Efstratiou and George 1999). Samples from skin lesions, when present, were also collected with sterile swabs.
C. ulcerans screening tests
Irregular Gram-positive rod strains were subcultured in the sheep blood agar plates, and Corynebacterium-like colonies were preliminarily characterized by Gram staining, colonial morphology, pigmentation, hemolysis (Mattos-Guaraldi and Formiga 1998, Efstratiou and George 1999), and DNase activities. DNase-positive results were mainly observed for C. ulcerans but not Corynebacterium pseudotuberculosis strains (Mattos-Guaraldi et al. 2008a, Pimenta et al. 2008).
C. ulcerans phenotypic characterization
The suspect bacterial isolate was identified as C. ulcerans by conventional biochemical assays and the semiautomated API-Coryne System (BioMérrieux, Lyon, France) (Efstratiou and George 1999, Funke and Bernard 2007, Mattos-Guaraldi et al. 2008a).
C. ulcerans molecular characterization
A multiplex polymerase chain reaction (PCR) assay targeting the genes 16S rRNA, RNA polymerase beta subunit-encoding gene (rpoB), and pld was performed as described previously (Pacheco et al. 2007). Primers targeting the pld gene designed by aligning the pld nucleotide sequences of C. pseudotuberculosis and C. ulcerans (GenBank accession nos. L16587 and L16585) were used. The reverse primer PLD-R1-ATCAGCGGTGATTGTCTTCC- was used in association with the forward primer PLD-F-ATAAGCGTAAGCAGGGAGCA- to amplify the pld genes of both bacteria, while primer PLD-R2-ATCAGCGGTGATTGTCTTCCAGG- excluded C. ulcerans.
Gene sequencing
The rpoB was isolated from the genomic DNA of the C. ulcerans strain, and a partial sequence was generated for molecular characterization. Briefly, the genomic DNA was extracted by a protocol standardized previously (Pacheco et al. 2007), and a highly polymorphic region of the rpoB was amplified by PCR using primers C2700F (5′-CGTATGAACATCGGCCAGGT-3′) and C3130R (5′-TCCATTTCGCCGAAGCGCTG-3′) (Khamis et al. 2004). The resultant 446 bp amplicon was precipitated with 15% (w/v) polyethylene glycol (Kusukawa et al. 1990) and sequenced using the DYEnamic ET Dye Terminator Kit (GE Healthcare, Chalfont St. Giles, UK), following the manufacturer's instructions. The sequence obtained was compared with the previously published C. ulcerans rpoB sequence (GenBank accession no. AY492271) through search for similarity using the basic local alignment search tool-N (Altschul et al. 1990).
Toxigenicity
As C. ulcerans strains may acquire lysogenic corynephages coding for DT, PCR assay for the tox gene (using primer sets Dt1, targeting fragment A [nt 43–294]) and Elek test were performed as previously described (Efstratiou and George 1999, Wagner et al. 2001). The presence of Pld was evaluated by the CAMP test (i.e., inhibition of hemolysis by Staphylococcus aureus) (Funke and Bernard 2007).
Antimicrobial susceptibility profiles
The sensitivity to antimicrobial agents (Oxoid, Hampshire, United Kingdom), penicillin G (10 U), ampicillin (10 μg), cephalothin (30 μg), erythromycin (15 μg), trimethoprim/sulfamethoxazole (1.25/23.75 μg), ciprofloxacin (5 μg), rifampicin (5 μg), and vancomycin (30 μg), was determined by the disk diffusion method using inocula equivalent to a 0.5 McFarland standard, according to the Clinical Laboratory Standards Institute (CLSI) guidelines as previously adopted by other authors (Martínez-Martínez et al. 1995, Sing et al. 2003, 2005, Lartigue et al. 2005, Mattos-Guaraldi et al. 2008a). Plates were incubated at 37°C for 24 h and reconfirmed at 48 h using a cation-adjusted Mueller–Hinton agar with 5% sheep blood. Breakpoints for the susceptible strains were used as suggested by the CLSI for bacteria excluded from table 2A to 2K. As there is not yet a defined standard for interpreting these results, the one proposed in the CLSI document M45-A (ISBN 1-56238-607-7) was used (CLSI 2007). The breakpoints for S. aureus were considered in the cases of penicillin and ampicillin.
Results
C. ulcerans isolation and phenotypic characterization
From a total of 60 shelter animals, bacterial growth on the chocolate tellurite agar medium was observed in the nasal samples collected from 31 dogs. Twenty-seven irregular Gram-positive rod strains subcultured in the sheep blood agar plates were preliminarily characterized as Corynebacterium-like colonies. Five nonpigmented strains isolated from different dogs were DNAse positive, and only one strain was positive for both urease and CAMP-reverse tests, suggestive of C. ulcerans (named BR-AD22) strain. This dog isolate was positive for catalase, urease, alkaline phosphatase, and α-glucosidase. Nitrate, gelatinase, pyrazinamidase, and esculin hydrolysis were negative. Fermentation tests were positive for glucose, maltose, and ribose. However, the API code (0111324) for BR-AD22 strain was a better match for C. pseudotuberculosis (92.7%) than C. ulcerans (7.2%).
C. ulcerans molecular characterization
Results of a multiplex PCR assay performed in an attempt to distinguish between closely related C. ulcerans and C. pseudotuberculosis species are displayed in Figure 1. The rpoB from BR-AD22 strain was sequenced to confirm the species identity. The partial rpoB sequence of the BR-AD22 dog isolate (GenBank accession no. FJ545133) showed 97% of identity (score = 754; E-value = 0.0) with the sequence deposited for the type strain CIP106504 of C. ulcerans (Fig. 1).

Multiplex polymerase chain reaction amplification of 16S rRNA (816 bp), RNA polymerase beta subunit-encoding gene (rpoB) (446 bp), and phospholipase D (pld) (203 bp) gene for differentiation of Corynebacterium pseudotuberculosis and Corynebacterium ulcerans strains. Lane 1, 1 kb Plus DNA ladder marker; lane 2, C. pseudotuberculosis CIP 102968; lane 3, C. ulcerans GUH HJ 01 BM3796.3; lane 4, C. ulcerans 809; lane 5, C. ulcerans BR-AD22 dog isolate. The partial rpoB sequence of the BR-AD22 dog isolate (GenBank accession no. FJ545133) showed 97% of the identity (score = 754; E-value = 0.0) with the sequence deposited for the CIP106504 strain of C. ulcerans.
Clinical evaluation of animal infected with C. ulcerans
C. ulcerans was isolated from the nares of an asymptomatic 5-year-old female canine of undefined breed, weighing 15 kg. General clinical aspects, laboratorial findings, abdominal ultrasound, echocardiogram, and chest X-rays did not reveal any abnormalities, as exemplified in Figure 2. The dog did not have watery eyes, any nasal discharge, or any skin lesions. Laboratorial analysis of blood samples showed 37.4% Hct, 13 g/% Hgb, 2 × 106/mm3 platelets, 1.39 × 104/mm3 white blood cells, 18 U/L glutamic-oxaloacetic transaminase, 26 U/L glutamic-pyruvic transaminase, 32 mg% urea, and 0.6 mg% creatinine. Results obtained for creatine kinase and creatine kinase isoenzyme (CK MB) sensitive and specific indicators of muscular disorders were 123 and 115 U/L, respectively.
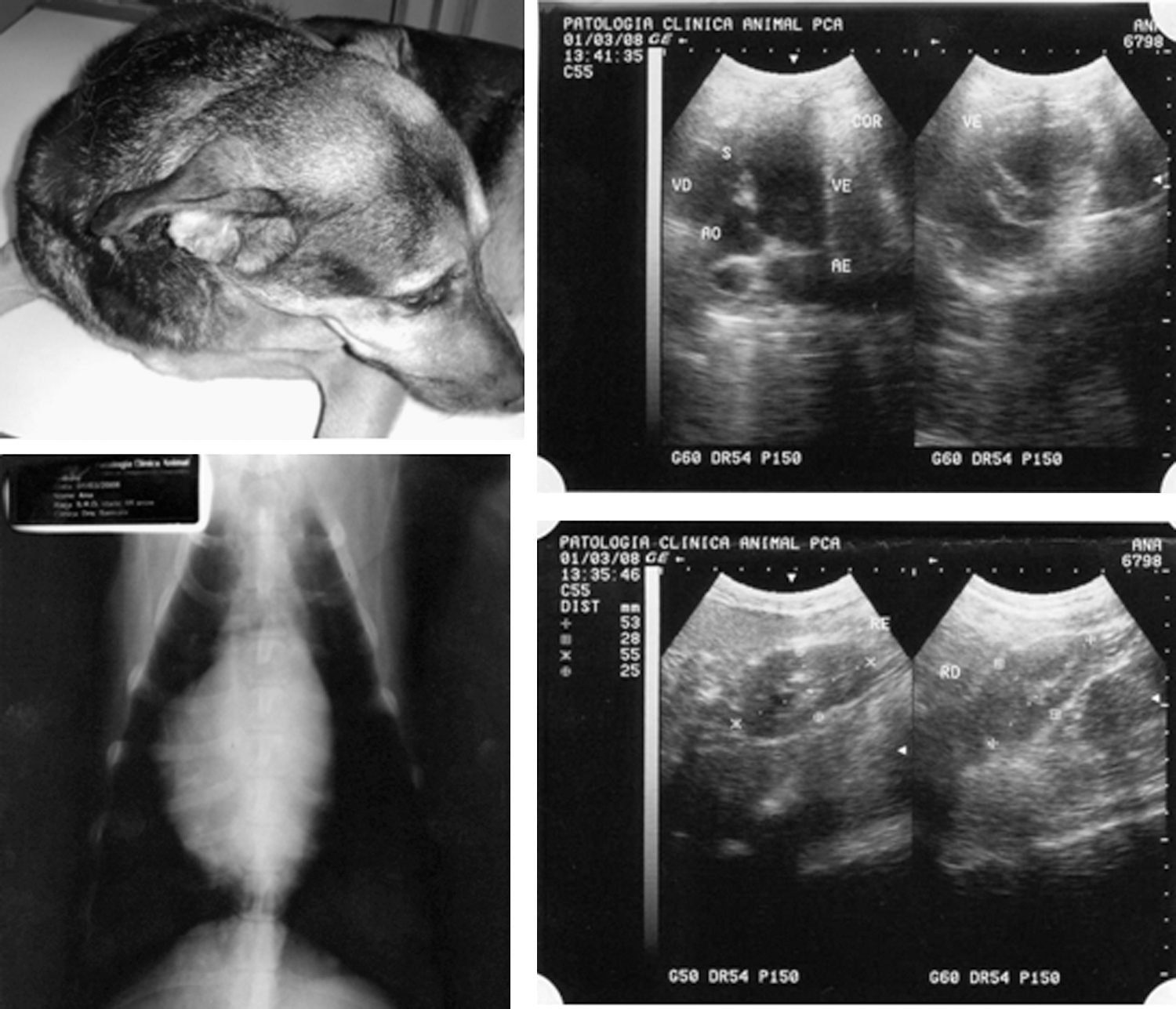
General appearance, frontal chest X-ray, cardiac, and renal ultrasound imaging of the shelter dog colonized by the C. ulcerans BR-AD22 strain.
Toxigenicity
The presence of Pld was confirmed by the positive reverse CAMP test, while the Elek test and PCR assay for the tox gene gave negative results.
Antimicrobial susceptibility profiles
C. ulcerans BR-AD22 strain showed resistance only to penicillin G and susceptibility to ampicillin, cephalothin, erythromycin, trimethoprim/sulfamethoxazole, ciprofloxacin, rifampicin, and vancomycin.
Carrier state
The dog that was colonized by the C. ulcerans BR-AD22 strain was kept in quarantine for 6 months, and swabs from throat, nares, eyes, skin, vagina, and ears were collected monthly. After 3 months, antimicrobial therapy was started with ciprofloxacin, 500 mg/day for 15 days. All tests after antimicrobial treatment were negative for C. ulcerans, and the animal was considered free of the pathogen. The employees and the other dogs were also examined monthly with no evidence of C. ulcerans carrier state.
Discussion
As the microorganism was found in small groups of apparently healthy dogs during studies performed in both industrialized (Katsukawa et al. 2009) and developing countries, it is safe to assume that dogs may not have any clinically apparent disease when they are colonized by C. ulcerans. These findings certainly increase one's concern for the circulation of this pathogen via asymptomatic dogs, especially in metropolitan areas. Dogs with unapparent C. ulcerans infections may be considered as potentially capable of infecting other animals and humans. Veterinary clinics should implement guidelines for dealing with C. ulcerans. Medical and veterinary staff should be aware that asymptomatic animals can carry C. ulcerans in the throat (Katsukawa et al. 2009) or nares and cooperate in eliminating infections and monitoring animals.
More than 90% of the expected population growth in the coming decades will be in the developing regions. Continuing global population growth, combined with rapid urbanization, means that many millions of city dwellers are forced to live in overcrowded and unhygienic conditions, where lack of clean water and adequate sanitation provide breeding grounds for infectious diseases. Expanding areas of human habitation put additional millions of people at risk from pathogens previously rare or unknown causes of human disease. Millions of people in emerging countries live and work in rural areas. Although most cases of the human patients have risk factors associated with C. ulcerans infections, such as drinking raw milk or contact with farm animals or their waste, interestingly, we found in the literature very few cases of C. ulcerans infections in humans or animals from developing countries.
Virulence mechanisms of C. ulcerans should become a matter of higher interest because of the increase in the number and severity of cases of human infection in different countries, especially those with immunization programs that have rendered DT rare. Similar to C. diphtheriae (Sing et al. 2003, 2005), the pathogenicity of some C. ulcerans strains may be independent of DT toxin production. Like other human or animal pathogens, C. ulcerans strains seem to be endowed with an array of virulence factors other than DT such as catalase, proteases, deoxyribonuclease, and Pld. Different from C. diphtheriae, when the tox gene is absent in C. ulcerans, Pld is the characteristic toxin produced. Dermonecrotic lesions caused by C. ulcerans, including the AD22 dog isolate, exhibit a large extent of yellowish-white fibrinous (fibrin) deposits (Mattos-Guaraldi et al. 2008b). Pld is also the causative agent of severe tissue necrosis in humans. To date, Pld is the most important virulence determinant identified in C. pseudotuberculosis and causes an increase in vascular permeability, has dermonecrotic properties, and reduces viability of neutrophils and macrophages (Schmiel and Miller 1999). C. ulcerans strains producing Pld, but not DT toxin, are able to cause severe disease in humans, such as pneumonia (Hommez et al. 1999, Hatanaka et al. 2003) and granulomatous nodules in pulmonary tissues (Desseau et al. 1995). Consequently, we do believe that the rarity of cases might be not due to a low pathogenicity of C. ulcerans as stated before by Funke and Bernard (2007). C. ulcerans strains unable to produce DT toxin should not be underestimated.
There is a great variation in the rates of infection from region to region; however, this is probably due to the variation in the rate of disease notification, rather than of the incidence itself. Some diseases have certain geographic distribution where the physicians of these areas may be not familiar with them, and most of their knowledge is from the literature.
Footnotes
Acknowledgments
We thank Dr. Samura Ferreira for providing clinical assistance during surveillance and treatment of the quarantined dog. This work was supported by grants from CNPq, CAPES, FAPERJ, SR-2/UERJ, PRONEX of the Brazilian Ministry of Science and Technology, and Programa Nacional de Pós-Doutorado–PNPD (CAPES/MEC).
Disclosure Statement
No competing financial interests exist.