
Abstract
Background:
Seasonal variations in the occurrence of toxoplasmosis have been studied only sporadically. We thus examined the seasonal distribution of acute toxoplasmosis in Serbia during a 4-year period (2004–2008).
Materials and methods:
A total of 391 consecutive symptomatic (recent lymphadenopathy) and 715 asymptomatic (women tested for obstetric reasons) patients were tested for Toxoplasma immunoglobulin G (IgG) (including IgG avidity) and IgM antibodies. The distribution of patients with acute infection, and of all patients from both groups, was analyzed for seasonality. In addition, factors (including undercooked meat consumption, contact with cats and with soil) possibly contributing to seasonality were analyzed in patients with acute infection (cases) matched by age, sex, and time (month and year) of infection (symptomatic) or presentation (asymptomatic) with seronegative patients (controls).
Results:
Acute toxoplasmosis was serologically (IgG avidity low, IgM positive) diagnosed in 39 (10.0%) symptomatic and 38 (5.3%) asymptomatic patients. In both groups, monthly distribution of acute infections showed significant (p < 0.0001) seasonality, which was related to the four seasons of the year (p < 0.0001). Importantly, the observed seasonality was not related to the distribution of all examined patients in either group (p < 0.001). In the symptomatic patients, acute infections occurred more often between October and March (p = 0.0486). Although more asymptomatic acute infections were diagnosed between February and July (p = 0.0037), low IgG avidity suggests that infection had occurred within the previous trimester (between November and April). Undercooked meat consumption was shown as a risk factor for symptomatic infection in the October–March period (odds ratio 7.67, 95% confidence interval 1.61–36.45).
Conclusion:
Seasonality patterns should be taken into account in the health education guidelines for the prevention of toxoplasmosis in pregnant women.
Introduction
The phenomenon of seasonal variations in acute human toxoplasmosis has been analyzed in only a few articles, with opposing results in different areas (Meenken et al. 1991, Ryan et al. 1995, Logar et al. 2005). Such differences may reflect variable influence of particular routes of infection between areas (Cook et al. 2000). On the other hand, the issue of seasonal variations may be important when planning toxoplasmosis prevention programs. We therefore conducted a study of the seasonal distribution of acute toxoplasmosis in Serbia and analyzed the contributing factors.
Materials and Methods
Study design
Seasonal variations in the incidence of acute Toxoplasma infection were analyzed in two groups of patients with serologically confirmed acute toxoplasmosis, that is, in symptomatic patients per date of infection, and in the asymptomatic ones per date of presentation. In addition, the risk factors contributing to the seasonal variations in acute infection were analyzed in a case–control study (as described below).
Study area
Serbia (excluding Kosovo) is a country of 77,474 km2 located in southeast Europe, in the centre of the Balkan Peninsula (46°10′–42°13′ N latitude, 18°38′–22°58′ E longitude), with rich fertile plains to the north (Vojvodina province) and hilly and mountainous regions in the central and southern parts of the country. The climate is temperate, with clearly defined seasons, hot summers (average July temperature 22°C), and cold winters (average January temperature 0°C), and slightly colder in the northern part of the country (Peel et al. 2007). The Belgrade District, defined by the outer boundaries of its 17 municipalities, is a highly urban area inhabited by approximately 2 million people. Located along the banks of the Danube and Sava rivers, its microclimate is slightly altered due to the urban/industrial impact.
Study population and samples
The National Reference Laboratory for Toxoplasmosis as the single reference laboratory for the diagnosis of this infection in Serbia does not regularly perform screening. Rather, patients, and occasionally only blood samples, are referred due to ambiguous or discrepant test results obtained in other laboratories. As a consequence, not many patients are tested, and the proportion of acute infections is higher than in the general population. Thus, a total of 391 consecutive patients with recent lymphadenopathy clinically suspected of acute toxoplasmosis and 715 asymptomatic women tested for obstetric reasons were examined between April 1, 2004 and March 31, 2008. Of these, acute toxoplasmosis (immunoglobulin G [IgG] positive and IgG avidity low, IgM positive) was confirmed in 39 symptomatic and 38 asymptomatic patients. Almost two-thirds of the patients (63%) originated from the Belgrade area.
For the analysis of the risk factors contributing to infection, patients with acute infection (cases) were matched by age, sex, and date (month and year) of onset of symptoms for symptomatic and of sampling for asymptomatic patients, with seronegative patients (controls) from appropriate groups.
Upon presentation, informed consent for participation in the study was obtained from all patients. The study was approved by a local (Institute for Medical Research) Ethics Committee.
Questionnaire
All patients sampled in the laboratory were interviewed using a standardized questionnaire, which included data on age, sex, date of onset of symptoms (where applicable), and on the lifestyle habits pertaining to infection transmission risk factors. These included consumption of undercooked meat (including undercooked liver and raw and cured meat products such as sausages and ham), exposure to soil (townhouse with garden, farming, and gardening in suburban home), and exposure to cats (pet cat ownership). The answers were recorded in dichotomous form (yes/no); patients were considered exposed to a factor if they gave a positive response to any of its modalities. Full questionnaire data were obtained from 35 of the 39 symptomatic patients and from 34 of the 38 asymptomatic ones, as well as from the same number of matched seronegative controls from appropriate group.
Serology
Detection of specific IgG antibodies and IgG avidity
Specific IgG antibodies were detected using the high sensitivity direct agglutination assay and the VIDAS® Toxo IgG II (BioMerieux, Marcy L’Etoile, France). The high sensitivity direct agglutination assay was performed as described by Desmonts and Remington (1980), using formalin-fixed RH tachyzoites as antigen, kindly obtained from Dr. Ph. Thulliez (Paris, France). Sera were serially diluted twofold starting from 1:20; the first dilution considered positive was 1:40 (2 Iu/m mL according to both the World Health Organization reference serum and a laboratory standard serum). The Toxo IgG II (which uses the enzyme-linked fluorescent assay technique) was performed on the fully automated VIDAS system. Results were interpreted as recommended by the manufacturer, as follows: <4 negative, 4–8 borderline, and >8 Iu/m mL positive. The avidity of the specific IgG antibodies was measured by the VIDAS TOXO IgG avidity (BioMerieux), performed according to the manufacturer's instructions. The results were expressed as avidity indices; index <0.2 indicates low, 0.2–0.3 borderline, and >0.3 high avidity.
Detection of specific IgM antibodies
Specific IgM antibodies were detected using the IgM-immunosorbent agglutination assay and/or the VIDAS Toxo IgM (both BioMerieux), as recommended by the manufacturer. For the immunosorbent agglutination assay, results were expressed as an index on a 0–12 scale, where 0–5 was considered negative, 6–8 borderline, and ≥9 positive. The cut-off for the VIDAS Toxo IgM assay was 0.55, results between 0.55 and 0.65 were considered borderline and >0.65 positive.
Statistical analysis
Seasonal variations (monthly and per season of the year) in the groups of symptomatic and asymptomatic patients were analyzed by the test for seasonality of a time series (seasonality χ 2), while the variations between two periods/year were examined by the χ 2 test (2 × 2 contingency tables). The monthly distribution of symptomatic and asymptomatic patients with acute infection was compared with all patients from the same group by the Kolmogorov–Smirnov test for two populations. The association between Toxoplasma infection and the risk factors was analyzed by the multivariate Wald forward stepwise logistic regression method. The level of statistical significance was 0.05.
Results
Patients with symptomatic acute toxoplasmosis
Of a total of 391 patients presenting with lymphadenopathy, acute toxoplasmosis was serologically diagnosed in 39 (10.0%) patients. These included 28 females and 11 males (p = 0.048), with a mean age of 31.1 ± 10.2 years (range 15–54 years) and no age difference between sexes (p = 0.455).
Monthly distribution of the patients with acute infection according to the date of onset of clinical symptoms, presented in Figure 1, showed significant seasonality (p < 0.0001). Comparison of the monthly distribution of acute cases with all symptomatic patients (Fig. 2) showed different distribution patterns (p < 0.001, Kolmogorov–Smirnov test), indicating that the monthly distribution of patients with acute toxoplasmosis was not related to the distribution of all symptomatic patients. Analysis per season (January–March winter, April–June spring, July–September summer, October–December autumn) showed that the observed variations were season related (p < 0.0001). Finally, analysis per only two periods (the period April–September referred to as summer and October–March referred to as winter) showed an increased (p = 0.0486) frequency of acute infections during the winter period.
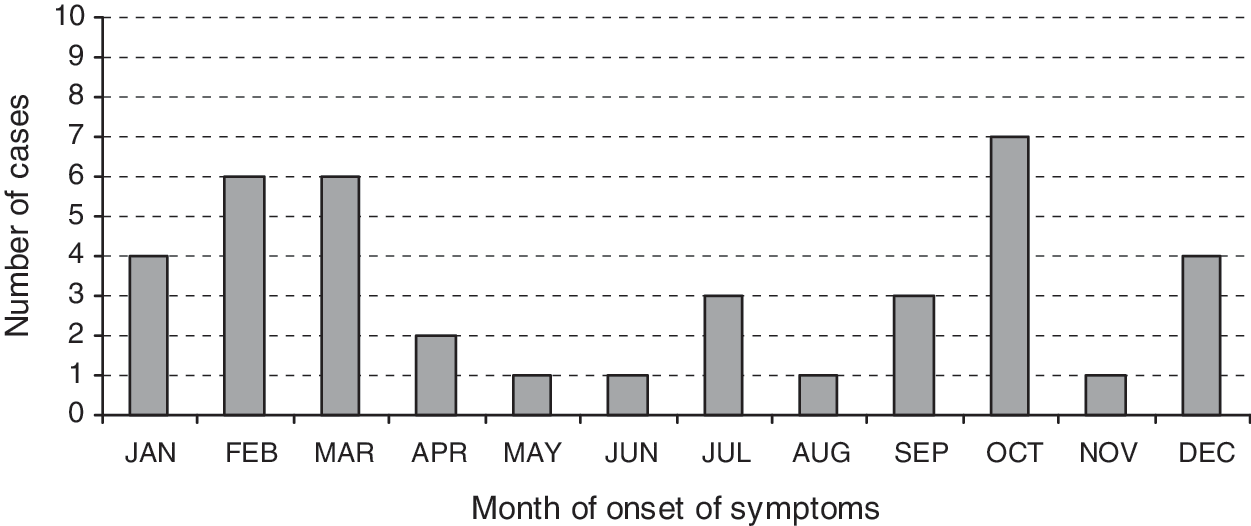
Cumulative distribution (2004–2008) of symptomatic patients (n = 39) with acute toxoplasmosis by the month of onset of symptoms.
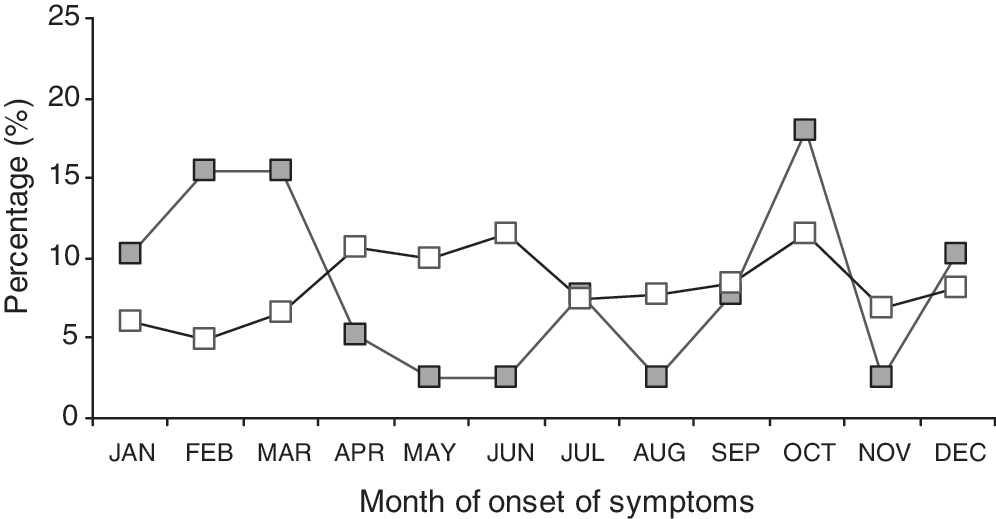
Percentage distribution of symptomatic patients examined between 2004 and 2008 by the month of onset of symptoms. Open squares, all symptomatic patients (n = 391); filled squares, patients with acute toxoplasmosis (n = 39).
Patients with asymptomatic acute toxoplasmosis
Of a total of 715 asymptomatic patients (women tested for obstetric reasons), acute toxoplasmosis was serologically diagnosed in 38 (5.3%) women (age mean 31.34 ± 4.9 years, range 16–41).
Monthly distribution of the asymptomatic patients with acute infection according to the sampling date is presented in Figure 3. As in the symptomatic patients, the monthly distribution of asymptomatic patients with acute toxoplasmosis was not a reflection of monthly variations in the distribution of all asymptomatic patients, because the distribution patterns of these two populations differed significantly (p < 0.001) (Fig. 4).
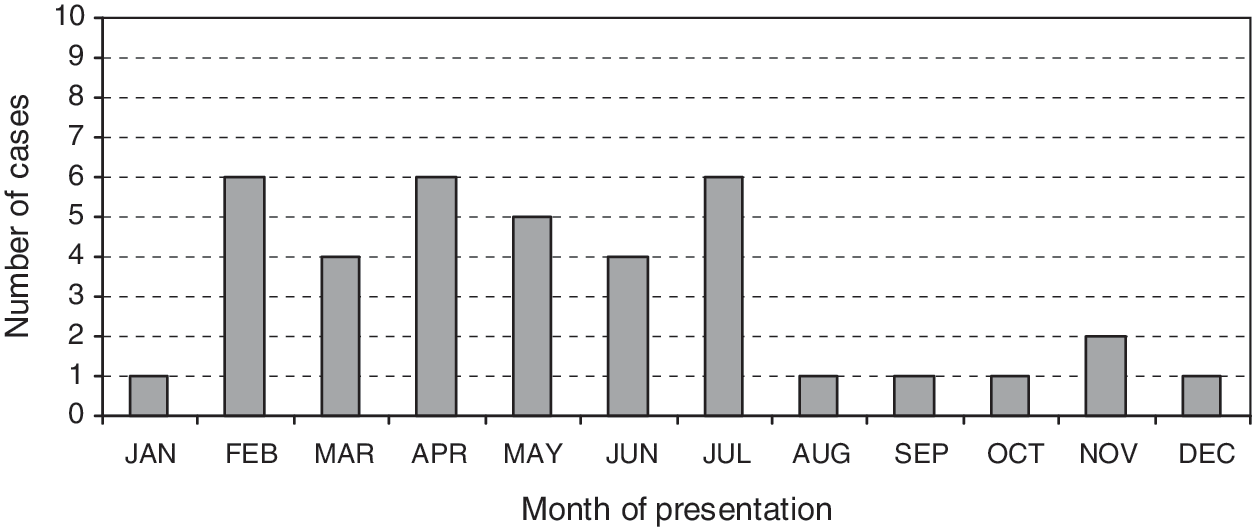
Cumulative distribution (2004–2008) of asymptomatic patients with acute toxoplasmosis (n = 38) by the month of presentation.
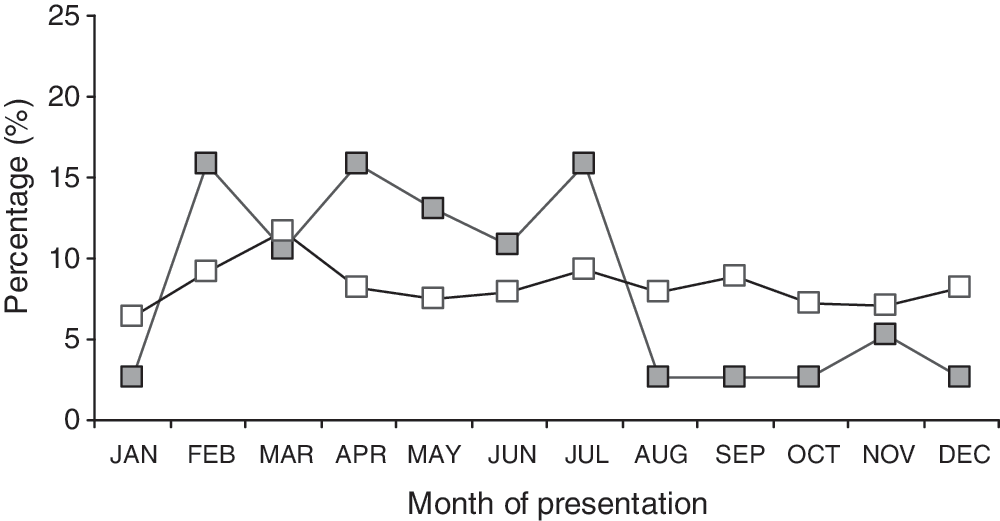
Percentage distribution of asymptomatic patients examined between 2004 and 2008 by month of presentation. Open squares, all asymptomatic patients (n = 715); filled squares, patients with acute toxoplasmosis (n = 38).
The monthly distribution of acute cases had a seasonality pattern (p < 0.0001), and moreover, was related to the four seasons (p < 0.0001). However, the frequency of acute infections did not differ between the summer and winter periods (p = 0.356), but it was significantly higher between February and July than between August and January (p = 0.0037).
Finally, the monthly distribution of acute infections in the symptomatic and the asymptomatic patients was similar (p > 0.1, Kolmogorov–Smirnov test).
Risk factors for acute toxoplasmosis (case–control study)
The potential contribution of Toxoplasma transmission risk factors, including contact with cats, consumption of undercooked meat, and contact with soil, to the observed seasonality of acute toxoplasmosis was analyzed separately for symptomatic and asymptomatic patients in a case–control manner according to the periods of different frequency of infection (Table 1).
OR, odds ratio; CI, confidence interval.
In the symptomatic patients, an increased risk of Toxoplasma infection was shown for undercooked meat consumption in the winter period (odds ratio 7.67, 95% confidence interval 1.61–36.45). During the summer period, the risk of infection was not associated with any examined factor although undercooked meat consumption was close-to-significant (p = 0.056). In the asymptomatic patients, no factor was associated with acute infection in either examined period, but the influence of undercooked meat consumption, approaching significance (p = 0.052) in the period of increased frequency of infection, was higher than in the period of lower infection frequency (p = 0.377).
Discussion
The results of this study show strong seasonality of acute human toxoplasmosis in Serbia during the 4 studied years. Seasonal variations in the incidence of acute infection did not parallel variations in the monthly distribution of all patients, indicating that the observed seasonality was related to Toxoplasma infection.
The frequency of symptomatic acute infections was increased during the period between October and March, and of asymptomatic acute infections between February and July. However, the differences in the periods of increased frequency of infection may actually not be as large as they appear, because the symptomatic patients were analyzed according to the actual date of the onset of symptoms, whereas the asymptomatic patients were analyzed according to the date of sampling. A major criterion for the diagnosis of acute toxoplasmosis in the asymptomatic patients was a low specific IgG avidity index, which is inferred to remain low during 4 months after infection (Montoya and Remington 1995, Bobić et al. 2009). It may thus be assumed that patients with low IgG avidity acquired the infection within the previous trimester, indicating increased frequency of infection between November and April.
Previous studies have showed conflicting results. In a study of pregnant women in Slovenia (Logar et al. 2005), infection was more frequent in the winter–spring than in the summer–autumn period, while in a study of congenitally infected children in Denmark (Meenken et al. 1991), maternal infection was shown to have occurred more frequently between March and May. In contrast, Ryan et al. (1995) did not find significant seasonal trends of toxoplasmic lymphadenopathy or eye disease in adults in England and Wales. In addition to the differences in the study populations and geographical areas, as well as the wide time period among these studies, the conflicting findings may indicate differences in the influence of particular routes of infection and/or their seasonal changeability among areas.
Infection is generally acquired by ingestion, of oocysts from contaminated soil or through contact with cats, or of cysts from undercooked meat. Although summer is the period when more time is spent outdoors allowing for increased exposure to environmental contamination, a possible decline in the incidence of acute infection has been suggested during the warmer and drier season because of a reduction in the number of viable oocysts in the environment. However, this is also the period when meat dishes (barbecues) tend to be more lightly cooked (reviewed in Hall et al. 2001). In view of these considerations, it is challenging to explain our results on no influence of contact with soil (or cats) in any patient group at any period of the year, and of significant influence of undercooked meat consumption in the patients with symptomatic acute infection in the winter and not in the summer period. The influence of undercooked meat consumption was also suggested in the asymptomatic patients in the period of increased frequency of infection.
Consumption of undercooked meat is not part of the Serbian culture, such as it is for instance in France. However, despite a dramatic change in the prevalence of Toxoplasma infection over the past three decades in Serbia, which has at present reached an all-time low of around 30%, undercooked meat consumption has repeatedly been shown to be a major route of infection (Bobić et al. 1998, 2007). Thus, its changing influence during the year shown in this study may be explained by features of the local culture. Food animals in Serbia have a high prevalence of Toxoplasma infection (Klun et al. 2006), and animals raised traditionally, which are still an important source of meat in Serbia, have a higher prevalence than animals raised in intensive farming systems. Traditionally, in semi-rural and rural areas of the Balkans, these animals are slaughtered during autumn and early winter (mostly in November and December), and meat is prepared for curing, and sausages and other traditional meat products are made. These products are often seasoned to taste while raw and also eaten before the necessary curing period has elapsed. On the other hand, winter dishes are prepared with less vegetables and more meat. In addition, Serbian culture includes celebration of the family patron saint (such as St. George, St. Michael, St. Nicolas, St. John), a kind of an open-house day attracting lots of guests, and dishes served necessarily include roasted young pigs and other meats and meat products. Most of these holidays fall between November and February, providing an opportunity for more people to contract the infection from a single source, such as accidentally improperly prepared meat. This favors winter peaks in the occurrence of trichinellosis in Serbia (Anonymous 2005) as well as in the neighboring countries of Bulgaria and Romania (Kurdova-Mintcheva et al. 2009, Neghina et al. 2009) and is likely to contribute to an increased incidence of toxoplasmosis as well.
One limitation of this study may be the rather small number of cases of acute infection involved. However, the statistically strong seasonality shown in a relatively modest sample size emphasizes the phenomenon itself.
The seasonality patterns described in this study should be taken into account in programs for the prevention of toxoplasmosis, by including considerations on higher risk periods in the health education guidelines for pregnant women.
Footnotes
Acknowledgment
The study was financially supported by a grant (project No. M145002) from the Ministry of Science and Technological Development of Serbia.
Disclosure statement
No competing financial interests exist.